IJCRR - 4(20), October, 2012
Pages: 119-124
Print Article
Download XML Download PDF
A STUDY ON PREVALENCE OF ISCHEMIC HEART DISEASE IN YOUNGER AGE GROUP (40 YEARS) IN PATIENTS WITH METABOLIC SYNDROME
Author: Rajesh Khoiwal, Sandeep Vaishnav
Category: Healthcare
Abstract:Objective \- we estimate the prevalence of ischemic heart disease in younger age group (< 40 years) patients with metabolic syndrome. Research Design and Methods\- 100 patients who satisfied the selection criteria were thoroughly examined and undertook relevant routine investigation to assess the diabetic status, hypertension, and lipid profile. Anthropometry i.e. height, weight, Body Mass Index, waist circumference and diabetic complication, were selected for Tread Meal Test. Those who are Tread Meal Test positive were taken for study. Results\- The mean value of metabolic syndromes of Waist Circumference, Triglyceride, High Density Lipoproteins, Systolic Blood Pressure , Diastolic Blood Pressure and Fasting Blood Sugar in ischemic heart disease patients was (95.67+8.22), (193.10+36.92), (36.63+3.2), (148.04+12.63), (89.43+4.94) and (130.60+25.83) respectively. All criteria of metabolic syndrome were significantly different in between Ischemic Heart Disease and non Ischemic Heart Disease group. Conclusions-The finding of the present study clearly reveals that high prevalence of Ischemic Heart Disease in younger metabolic syndrome patients.
Keywords: acute ischemic stroke, C- reactive protein, Serum lipid profile
Full Text:
INTRODUCTION
Customary health variations are a worldwide problem. Lessening of preventable human suffering caused by insufficient access to healthcare amenities is being advocated worldwide. But what is the scenario for human being health in developing countries where there is an increased risk of adult chronic diseases against a backdrop of persistent catastrophe of infectious diseases, environmental degradation, and political apathy? (1)A major pattern is that of cardiovascular disease (CVD). Studies showed that CVD has arrived at epidemic peak in many developing countries. In India, mortality attribute to CVD is anticipated to go up by 103% in men and by 90% in women from 1985 to 2015 (2). More importantly, the disease grabs Indians young. Therefore, to stop the callous attack of CVD in developing countries, there is an urgent need to describe the disease in the health plan of these countries. A cost effective preventive approach will necessitate to center on plummeting risk factors both in the individual and in the population at large. Therefore, it is vital to carry out some prospective studies in developing countries such as India to identify CAD risk factors, particularly modifiable. However, scientific evidence for modifiable CAD risk factors (elevated serum total and low density lipoprotein cholesterol) [LDL-C], low high-density lipoprotein cholesterol [HDL-C], smoking, diabetes, hypertension, low level of physical activity, and obesity) in this population may be supportive in inventing a straight CAD prevention policy. (3)
The occurrence of Ischemic Heart Disease(IHD) has increased noticeably for the period of last decade, not only in urban areas but in rural areas also, but it is not that abrupt because life style variation have affected populace in urban areas more than in rural areas.(4) This syndrome is often related with obesity, diabetes mellitus, dyslipidemia, and hypertension. All of these abnormalities promote a cardiovascular disease risk, and collectively they are categorizing as the insulin resistance syndrome or the metabolic syndrome. (5) Although the all entities of the metabolic syndrome are evidently connected with increased risk for coronary heart disease (CHD), we wanted to quantify the increased prevalence of CHD among people with metabolic syndrome. The current study was designed to evaluate the cross sectional relationship between the metabolic syndrome (defined by the ATP III criteria) and the prevalence of ischemia heart disease in Indian subjects.
MATERIAL AND METHOD
This study was conducted in the Department of Medicine and Cardiology, JLN Medical College and Hospital, Ajmer. The study included the patients who attended the medical OPD and get admitted in the wards during June 2008 to May 2009. Selection Criteria: 1. Asymptomatic patient having no history of chest pain suggestive of coronary artery disease. 2. Obese personalities. 3. Age less than 40 years. 4. Patient irrespective of blood sugar / blood pressure level but fit for TMT. Exclusion Criteria 1. Follow up patient of myocardial infarction / CVA / angina. 2. Patient of valvular heart disease. 3. Patient of conduction defect. 4. Patient of COPD / bronchial asthma. 100 patients who satisfied the selection criteria were thoroughly examined and underwent relevant routine investigation to assess the diabetic status, hypertension, lipid profile. Anthropometry i.e. height, weight, BMI, waist circumference and diabetic complication were selected for TMT. Those who are TMT positive were taken for study.
RESULTS
Age of the patients varied between 29 - 40 years. Mean age of patients was 36.05 years. Out of 100 patients, 62 were males and 38 were females. Mean age of male patients was 36.30 and mean age of female patients was 35.57 years. There was no case found below 29 years. All age group had male predominance except 29-31 years of age group where all the patients were females. This can be due to less number of patients studied. Maximum numbers of patients were in age group 38-40 years. Out of 100 patients 46 were Tread Meal Test positive (having Ischemic Heart Disease). Out of these 46 patients, 24 (52.17%) were male and 22 (47.83%) were female. In non-IHD group out of 54 patients, 38 (70.37%) were male and 16 (29.62%) were female. The prevalence of IHD among males was found to be 38.70% (24/62) and that in females was 57.89% (28/38).P value is 0.0674 denote that ischemic heart disease is equally distributed in male and female and there is no sex correlation. As in our study 52.17% male and 47.83% female had ischemic heart diseases those were fulfilling the criteria for metabolic syndrome. Out of 100 patients with metabolic syndrome, 31 (31.00%) had both IHD and blood sugar level >110 mg/dl. Out of 46 patients with IHD, 31 (67.39%) had blood sugar level >110 mg/dl. In males with IHD, out of 41 patients, 15 (36.58%) had blood sugar >110 mg/dl. In females with IHD, out of 38 patients, 16 (42.10%) had blood sugar >110 mg/dl. Female patients having high blood sugar level and IHD was more in comparison to male.
Out of 100 patients with metabolic syndrome, 44 (44.00%) had both IHD and high blood pressure (BP >130/85 mmHg).Out of 46 patients with IHD, 44 (95.65%) had blood pressure >130/85 mmHg. In male patients 24/62 (38.70%) had IHD and hypertension. In female patients 20/38 (52.63%) had IHD and hypertension. Percentage of females having high blood pressure and IHD was more than males. Out of 100 patients with metabolic syndrome, 45 (45.00%) had both low High Density Lipoprotein (HDL) level and IHD. Out of 46 patients with IHD, 45 (97.83%) had low HDL level (below cut off value).In male patients, 23/62 (37.1%) had both IHD and low HDL level (150 mg/dl. Out of 46 patients with IHD, 42 (91.30%) had TG >150 mg/dl.In males out of 62, 23 (37.09%) had TG >150 mg/dl and in females out of 38, 19 (50.00%) had TG >150mg/dl. Percentage of females with increased TG (50.00%) was more than males (37.09%). Out of 100 patients with metabolic syndrome, 26 (26.00%) had both IHD and increased waist circumference. Out of 46 patients with IHD, 26 (26/46 - 56.52%) had both IHD and waist circumference more than cut off value. In male patients, out of 62, 10 (10/62 - 16.12%) had both IHD and increased waist circumference above cut off value. In female patients out of 38, 16 (16/38 - 42.10%) had both IHD and increased waist circumference above cut off value. Percentage of females with increased waist circumference and having IHD (42.10%) was more than the percentage of males (16.12%).
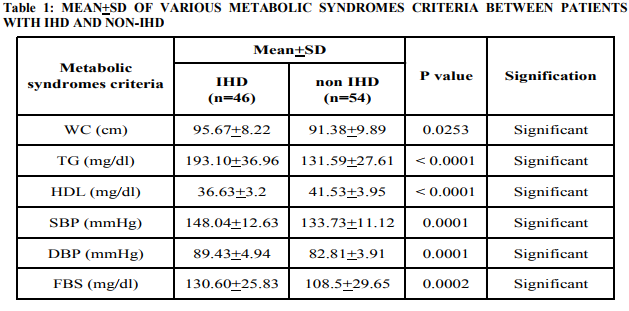
The mean value of metabolic syndromes of Waist Circumference (WC), Triglyceride (TG), High Density Lipoprotein (HDL), Systemic Blood Pressure (SBP), Diastolic Blood Pressure (DBP) and Fasting Blood Sugar (FBS) in ischemic heart disease patients was (95.67+8.22), (193.10+36.92), (36.63+3.2), (148.04+12.63), (89.43+4.94) and (130.60+25.83) respectively. It was observed that mean values of 4 criteria of metabolic syndrome except HDL were higher in IHD patients group as compared to non IHD patient group. Mean value of HDL was lower in IHD patients as compared to non IHD patients. All criteria of metabolic syndrome were significantly different in between 2 groups (IHD/non IHD group).
DISCUSSION
The study was carried out in the Department of Medicine and Cardiology, JLN Medical College and Associated Group of Hospitals, Ajmer on the patients who were referred for TMT. All patients who fulfill the NCEP ATP III criteria were included in this study. This study was conducted on 100 patients, attending Medicine outdoors and wards found to have metabolic syndrome. In our study we categorized metabolic syndrome group patients into two groups TMT positive patients and TMT negative patients. Metabolic syndrome is very common with 44% of the western countries population over 50 years of age meeting the NCEP ATP III diagnostic criteria.(5)It is estimated that it affect 65% male and 47.8% female in India (6).Recent study showed that the metabolic syndrome is associated with an increased prevalence of IHD. One possible reason for the high prevalence of IHD associated with metabolic syndrome is the direct effect of insulin resistance on the heart and arteries (7). A study was conducted by the National Centre for Health Statistics (NCHS) 3 Centre for Disease Control and Prevention in two phases - Phase I (1988-1995) and Phase II (1991-1994) showed that excess prevalence of IHD was attributed to metabolic syndrome and/or diabetes was 37.4% in the group with metabolic syndrome. In our study, there were 100 patients with metabolic syndrome, out of which 38 were female and 62 were male. Mean age among total patients was 36.05 years. The mean age among male was 36.30 years and mean age of female patients was 35.57 years. Out of 100 patients with metabolic syndrome 46 (46%) were found to have IHD. Among these 46 IHD patients 24 (52.17%) were male and 22 (47.83%) were female. The prevalence of IHD among male was found to be 38.70% (24/62) and that in female was 57.89% (22/38). There is no significant correlation between sex and IHD (P=0.0674). In contrast to our observation a study carried out by NCHS (8) showed prevalence of IHD is 38%. In our study it was 46% because in our study all criteria of metabolic syndrome were present. A study carried out by R. Gupta (2002) (4) showed the prevalence rate of IHD in urban males was 60.98 per thousand and rural males was 67.01 per thousand while in urban females prevalence rate was 30.82 per thousand and rural females was 27.33 per thousand. But in our study the prevalence of IHD among male and female was comparable. This was due to less number of patients studied. Among 46 IHD patients maximum numbers of patients were present between age group 38 - 40 years. In our study, criteria of age is restricted to only younger patients (110 mg/dl and out of 46 patients with IHD, 31 (67.39%) had blood sugar >110. In male with IHD out of 41 patients, 15 (36.58%) had blood sugar >110 mg/dl and in female with IHD, out of 38 patients, (42.10%) had blood sugar >110 mg/dl. Out of 100 patients with metabolic syndrome 44 (44.00%) had both IHD and high blood pressure. Out of 46 patients with IHD, 44 (95.65%) had blood pressure >130/85 mmHg. In males patients 24/62 (38.70%) had IHD and hypertension. In females 20/38 (52.63%) had IHD and hypertension. Percentage of females having high blood pressure and IHD was more than males. Elevated blood pressure is a risk factor of prime importance and established association with coronary atherosclerosis. Naik (1968) (11) reported that 36% cases of IHD were hypertension, But in our study high blood pressure was present in 44 (95.65%) with IHD because in our study all metabolic syndrome criteria were present which increases coronary atherosclerosis. Out of 100 patients with metabolic syndrome 45 (45.00%) had both low HDL and IHD. Out of 46 patients with IHD, 45 (97.83%) had low HDL (below cut off value). In males, 23/62 (37.1%) had both IHD and low HDL level (M)]. In the Framingham Heart Study (1986) (12), IHD was present in 44% patients with low HDL level (150 mg/dl and out of 46 patients with IHD, 42 (91.30%) had TG >150 mg/dl. Further in males out of 62, 23 (37.09%) had TG >150 mg/dl and in females, out of 38, 19 (50.00%) had TG >150 mg/dl. Percentage of females with increased TG (50.00%) was more than males (37.09%). A prospective cohort study was carried out by Nordegestgard BG et al (2007) (13) in 7857 women and 6394 men with high TG levels (>150 mg/dl) and were followed up from 1976 to 2004. They found that 1567 women (19.94%) and 1912 men (29.90%) developed IHD. But in our study prevalence of IHD was 37.09% in males and 50% in females with high TG levels. High prevalence in males and females in our study was due to presence of all metabolic syndrome criteria. In comparing IHD and WC, out of 100 patients with metabolic syndrome, 26 (26.00%) had both IHD and increased WC. Out of 46 patients with IHD, 26 (26/46 - 56.52%) had both IHD and WC. In males, out of 62, 10 (16.12%) had both IHD and increased WC (>102 cm) and in females out of 38, 16 (42.10%) had both IHD and increased WC (>88 cm). Percentage of females with increased WC and having IHD (42.10%) was more than the percentage of males (16.12%). Philip WJT (2005) (14) studied prevalence of IHD in patients with increased WC (female >88 cm, male >102 cm) and showed that prevalence was 16%. But in our study prevalence of IHD was 26%; this was because of presence of all criteria of metabolic syndrome. In comparison of mean of various criteria for metabolic syndrome patients among IHD and Non-IHD patients (Table 1). We found that the mean values of metabolic syndrome criteria for waist, TG, HDL, SBP, DBP and BS in IHD patients was (95.67+8.22), (193.10+36.96), (36.63+3.2), (148.04+12.63), (89.43+4.94), (130.60+25.83) respectively. It was observed that mean value of metabolic syndrome criteria (except HDL) were higher among IHD patients as compared to Non-IHD patients. Whereas the mean value of HDL was low in IHD compared to Non-IHD patients.
CONCLUSION
From this study it is concluded that TMT positive ischemic heart disease in metabolic syndrome patients have more waist circumference, high fasting plasma glucose, high blood pressure and high TG level but low HDL level. So there is a high prevalence of IHD in younger metabolic syndrome patients.
References:
1. Sharma M, Ganguly N K. Premature Coronary Artery Disease in Indians and its Associated Risk Factors. Vasc Health Risk Manag. 2005 September; 1(3): 217–225.
2. Bulatao RA, Stephens PW. Global estimates and projections of mortality by cause, 1970- 2015. Preworking paper 1007. Washington: Population Health and Nutrition Department, World Bank; 1992.
3. Aggarwal A, Aggarwal S, Goel A, Sharma V, Dwivedi S.A retrospective case-control study of modifiable risk factors and cutaneous markers in Indian patients with young coronary artery disease. J R Soc Med Cardio 2012; 1: 8
4. Gupta R, Gupta VP, Sama M et al: Prevalence of coronary heart disease and coronary risk factor in urban Indian population: Jaipur Heart Watch-2. India Heart 2002; 54: 59-66.
5. Adult Treatment Panel III, Executive summary of third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation and treatment of high blood cholesterol in adult. JAMA, 2001; 285: 2486-2497.
6. Coronary Heart Disease in India.Park a Textbook of Preventive and Social Medicine, 17th ed, 2001: 274.
7. Stout RW: Insulin and atheroma, 20 year prospective study. Diabetes Care, 1990; 13:631-54.
8. Alexander EM, Landsman PB, Teutehsm, and Hattner SM: NCEP defined metabolic syndrome diabetes and prevalence of coronary heart disease among NHANES III participants aged 50 years and older. Diabetes 2003; 52: 1210-1214
9. Mukherjee AB: Precious ischemic heart disease. IMA 1968; 512: 207.
10. 10.Bhargava RK, Husain SA, Dave AS, Narang NK, Banerjee A, Gupta U. Incidence of heart diseases in Rajasthan. J Assoc Physicians. India. 1966; 14 (1):15-23
11. Naik CH. Incidence and epidemiology of coronary artery disease in Gujarat. Indian Heart J. 1968 Jan; 20(1):3-10.
12. Castelli WP, Garrison RJ, Willson PW, Abbot RD, Kannel WB : Incidence of coronary heart disease and lipoprotein cholesterol levels; the Framinghan Study. JAMA 1986; 256: 2835-2838.
13. Nordestgaard BG, Benn M, Schnohr P, Tybjaerg-Hansen A. Nonfasting triglycerides and risk of myocardial infarction, ischemic heart disease, and death in men and women. JAMA. 2007; 298(3):299-308.
14. James WPT. The SCOUT study: risk-benefit profile of sibutramine in overweight high-risk cardiovascular patients. Eur Heart J 2005;7(Suppl. L):L44–L48.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





