IJCRR - 4(20), October, 2012
Pages: 112-118
Date of Publication: 20-Oct-2012
Print Article
Download XML Download PDF
SIGNIFICANCE OF VARIOUS SACRAL MEASUREMENTS IN THE DETERMINATION OF SEX IN SOUTH INDIAN POPULATION
Author: Mamatha H., Sandhya, Sushma R.K., Suhani S., Naveen Kumar
Category: Healthcare
Abstract:Introduction: In the identification of sex in human skeletal remains, sacrum is an important bone of the human skeletal system. Being a component of axial skeleton and because of its contribution to the pelvic girdle and in turn to the functional differences in the region between the sexes, it has an applied importance in determining the sex and related disorders with the help of measurements carried upon it. Therefore a study for sex determination was carried on 50 sacra, in the department of Anatomy Kasturba medical college, Manipal. India Materials and methods: The parameters used for the study were the different dimensions of the sacrum. Using the same the sacral index, auricular index were calculated. The morphology of the sacral hiatus and the extensions of the auricular surface were also studied. All the measurements were carried out using the digital vernier calliper. The readings were recorded and their mean and standard deviations were calculated. Results and conclusion: All the parameters chosen for the study were found to be reliable in sexing the sacra and identifying the related disorders.
Keywords: Sacrum, sacral index, auricular index, sacral hiatus, auricular surface, sex determination
Full Text:
INTRODUCTION
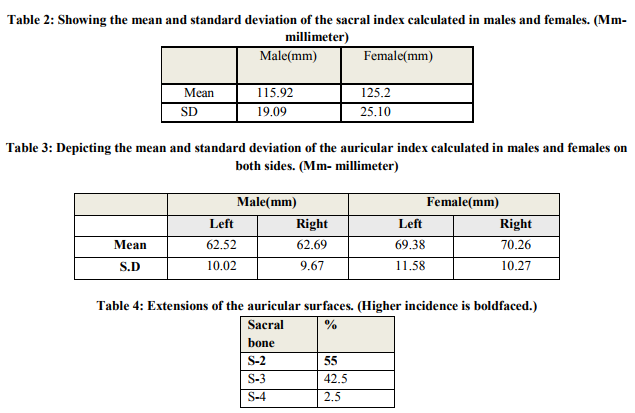
Sex determination of a skeleton is a problem of concern to paleoanthropologists, paleodemographers, forensic scientists and anatomists. Pelvic bones are most important for sex determination, followed by skull and the long bones. Forensic expert is often faced with a single specimen on whom he is asked to pronounce an opinion about its origin in general terms; or it may be necessary to establish as probably belonging to a given person when the identity is already suspected on circumstantial evidence (Kanika et al, 2011) The sex classification of a bone is possible with a degree of certainty only when it can be compared to a series of bones of known sexual dimorphism. Otherwise, a female bone could be classified as a male when the series to which it belonged was particularly robust. (Kanika et al, 2011) It has long been customary among anatomists, anthropologists and forensic experts to judge the sex of the skeletal material by non-metric observations. Lately, sexual divergence has been based upon actual measurements in different bones (Mishra SR et al, 2003). Sacrum is one such important bone for the identification of sex in human skeletal system. Since it is a component of axial skeleton and because of its contribution to the pelvic girdle and in turn to the functional differences in the region between the sexes, it has an applied importance in determining sex with the help of measurements carried upon it (MM Patel et al, 2003). Sacrum is a large, triangular bone formed by fusion of five vertebrae and forms postero-superior wall of pelvic cavity, wedged between the two innominate bones. Its blunted caudal apex articulates with the coccyx and its superior wide base with the fifth lumber vertebra at the lumbosacral angle. Since it is a component of axial skeleton and because of its contribution to the pelvic girdle and in turn to functional differences in the region between the sexes, it has an applied importance in determining the sex with the various measurements carried upon it (Standrig et al, 1988). The sacral hiatus is an opening present at the caudal end of the sacral canal. It is formed due to the failure of fusion of laminae of 5th sacral vertebra. Sacral hiatus has been utilized for administration of epidural anaesthesia in obstetrics as well as in orthopaedic practice for treatment and diagnosis. The area of auricular surface defines the magnitude of weight transmission to the hip bones (Standrig et al, 1988). Though sacrum is often considered to be an important bone, while dealing with sex differences in skeletal material, there is paucity of metrical data available for this bone. Metrical study of sacrum has been done by various authors (Wilder H. in 1920, Faweet E. in 1938, Davivongs V. in1963). Jit I et al, (1968) and Singh S et al (1968) advocated the demarking point, which identify the sex with 100% accuracy. Singh S et al (1968) have reported that even within the same general population, mean value may be significantly different in bones from different zones. Singh and Singh have shown that demarking point should be calculated separately for different regions of population because the mean of a parameter differs in values in different regions. The available literature clearly shows that the Indian sacra have not been studied widely except by Mishra et al (2003), Singh et al (1988)and Raju et al (in 1981), Jana et al (1988). The materials studied by them are from Agra, Varanasi and Burdwan and regions respectively. Therefore, the present study was undertaken with a view to study the sexdifferences in the South Indian population. MATERIALS AND METHODS The present study was performed on 50 adult sacra (25 male and 25 female) obtained from the Department of Anatomy, Kasturba Medical College, Manipal, India. All the sacra were normal and fully ossified. The following parameters of sacrum were measured using digital Vernier calliper. (Figure I) 1. Maximum width of the sacrum: was measured on the anterior surface with the sliding calliper by taking two points at the upper part of auricular surface anteriorly (or lateral most part of alae of sacrum). 2. Maximum height / length of sacrum: measured along the midline from the anterosuperior margin of the promontory to the middle of antero-inferior margin of last sacral vertebra. 3. Width of base / transverse diameter of the body of 1st sacral vertebra: measured by taking one point on each side of the lateral most part on the superior surface of the body of 1st sacral vertebra. 4. Transverse diameter of the wing (ala): measured on both the sides by taking one point on the lateral most part of superior surface of the body of 1st sacral vertebra and another point on the lateral most part of the alae. 5. Auricular surface length: It is the vertical auricular length, measured on the lateral aspect of sacrum by taking one point on the upper most part of auricular surface and another point on the lower most part of the auricular surface. 6. Extensions of auricular surface in relation to the sacral segments and morphology of the sacral hiatus were also observed. Using the above parameters sacral index, auricular index on either side were calculated. 7. Sacral index: Width × 100 / Height.
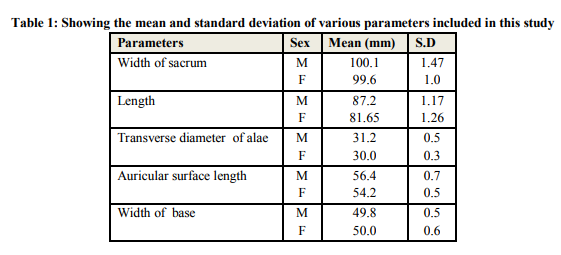
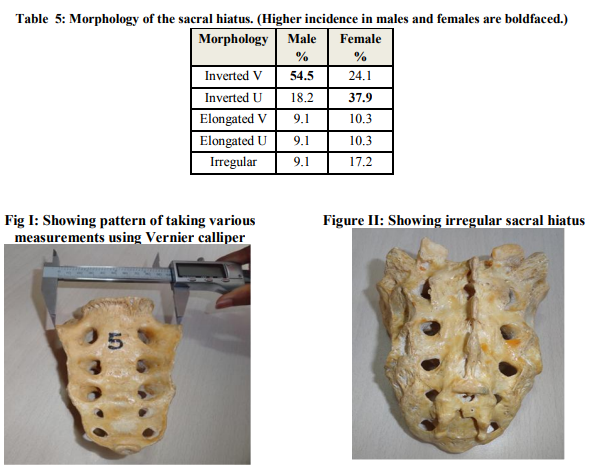
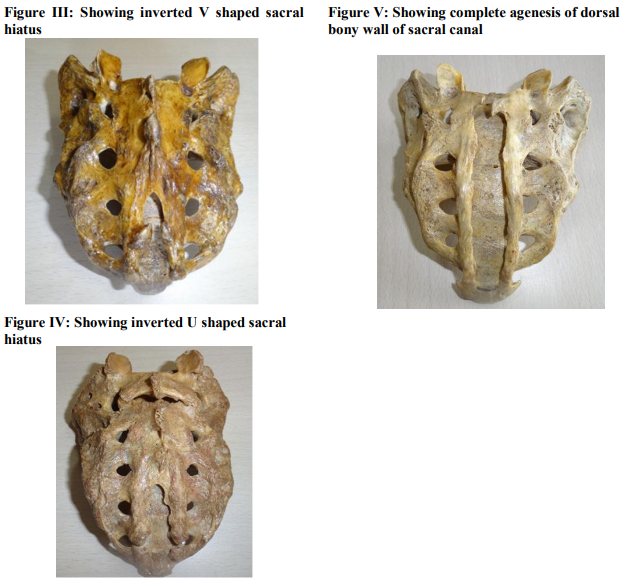
8. Auricular index: Length of auricular surface × 100 / Width The readings were recorded, tabulated and subjected for statistical analysis. RESULTS The mean and standard deviations of various parameters are given in Table1. The mean values of width and height of the sacrum, transverse diameter of the wing and the auricular surface length was more in males as compared to females. However the width of the base was higher in females than in males. The mean values of sacral index (Table 2) and auricular index (Table 3) is higher in females than in males. The extension of the auricular surface corresponding to the sacral segments was also noted. (Table 4) Morphology of the sacral hiatus was also studied (Figure II, III, IV) and tabulated in Table 5. Also complete agenesis of dorsal bony wall of sacral canal (Figure V) was observed in one of the sacra. DISCUSSION The sacrum has always attracted the attention of the medico-legal experts for establishing the sex, because of its contribution to pelvic girdle and associated functional sex differences. While teaching sex differences in bones much stress is laid on the importance of sacrum. Actually, very little data is available to test the validity of the number of parameters described to identify the sex of sacra (Devivongs V, 1963). The demarking points of various parameters will help to identify the sex with certainty, which is of paramount importance in medico-legal cases. The mean length (Table1) of the male sacra in the present study is 87.2mm, which is lower when compared to that of Agra region (107.53mm) studied by Mishra et al. and the Varanasi region (104.96mm) studied by Raju et al (1981). The mean length of the female sacra (81.65mm) is also shorter when compared to Agra and Varanasi regions. Comas and Charles (1961) reported a wide variation between the male and female in the Chinese, Negroes and Bushmen. Davivongs (1963) in his study of Australian aboriginal sacra has re-ported mean length of sacrum to be 96.52mm and 88.12mm in the male and female respectively, which is very much in agreement with the measurements in the present study. The mean width (Table 1) of the male sacra in the present study is 100.1mm which is close to similar observations made by Mishra et.al (2003).in the Agra region (105.34mm) and Raju et al. (1981) in the Varanasi region (105.33mm) respectively. However, in the females the present study showed a lesser value (99.6mm) than that of Agra and Varanasi regions. In the Australian aboriginal females, the maximum width of sacrum was 101.24mm, which is higher than that of males (99.92mm) of the same race (Davivongs V, 1963). Thus there exists a regional and racial difference in the length and width of the sacrum. The female ranges of transverse diameters of body of S1 (Table 1) are narrower than that of males and fall within the corresponding male ranges. The result is that the separation of any female sacrum from the males by the above measurements alone is impossible. The differences in the length of auricular surface (Table 1) between the males and females is significantly higher in male than in female supporting the normal description in the text books of Anatomy that the auricular surface for articulation with ilium is shorter in females than that of males. Based on the sacral index, anthropologists have classified the sacra into specific groups. The mean sacral index (Table 2) of the male and female sacra in the present series are 115.92mm and 125.2mm respectively falls under the platyheiric group (sacral index>106). Similar observation was reported by Martin (1960) (males: 112.4mm and females: 114.8mm), Raju et al (1981) and Davivongs (1963). However Mishra et al., in his study has classified the male sacra (sacral index: 98.22mm) under dolichoheiric group (narrow sacrum with sacral index up to 99.9) and female sacra (sacral index: 125.2 mm) under platyheiric group similar to the present study. Any way an attempt to use the sacral index for ethnic discrimination is very doubtful (Davivongs, 1963). However, its importance in sex determination cannot be denied since the differences between the males and females are highly significant. The mean auricular index (Table 3) is more in females (Left: 69.28mm; Right: 70.26mm) than males (Left: 62.52mm; Right: 62.69mm), unlike the observations made by Mishra et.al. in the Agra region wherein the latter had reported the auricular index to be higher in males (59.78mm) and females (51.69mm). The extensions of the auricular surface (Table 4) when observed, a majority of 55% was found to extend up to S2 vertebral level. The available literature does not mention about length and the extensions of the auricular surface in any of the sacra. The study on the morphology of the sacral hiatus (Table 5) revealed the most common to be is the inverted V shaped hiatus in 54.2% of males and inverted U in 37.9% of females. Elongated V, U and irregular shapes were also observed. Nagar S.K (2004) in his study had noted the shapes of sacral hiatus, most common being inverted U (41.5%) and inverted V (27%) similar to our study. In 13.3% its outline was dumbbell shaped, while in 14.1% it was irregular. Bifid hiatus was seen in 1.5% which was not present in our study. Vinod Kumar et al (1992) had also observed various shapes of sacral hiatus, most common being inverted V and inverted U in 76.23% of sacra, 7.43% were dumb bell shaped. There was complete agenesis of dorsal bony wall of sacral canal in 2% sacra of the present study. This is similar to that reported by previous workers namely Nagar S.K. (2004) 1.5%, Trotter (1947)1.8% and Vinod Kumar et al (1992) 1.49%. CONCLUSION Since sacrum is a component of pelvic girdle with functional differences between the two sexes, it itself becomes important for identification of sex in the human skeletal system. All the parameters used in the present study contribute to the sex determination in a positive way, the most significant being the sacral index and the auricular index. However a single parameter may not be of much use in sexing the sacra. Hence, it can be concluded that for the determination of sex of sacrum, maximum number of parameters should be taken to attain 100% accuracy. In addition to sex differences, regional and racial differences of the sacra are also stressed upon in the present study. The extension of the auricular surface varies in human sacra. These variations are associated with differential load bearing at the sacral joints. The position of the auricular surface can explain or possibly predict low back pain situations. The anatomical variations of the sacral hiatus are to be understood for it may be useful in improving the success of caudal epidural anaesthesia. In the present study inverted U and inverted V shapes were found in a significant percentage, which should be kept in mind while giving caudal anaesthesia in the South Indian population. Therefore to conclude, this study will be useful for the anatomists, anthropologists and experts in forensic medicine for accurate sexing of sacra and various other clinical tenacities.
References:
1. Kanika Sachdeva, Rajan Kumar Singla, Gurdeep Kalsey, Gaurav Sharma (2011), Role of Sacrum in Sexual Dimorphism- A Morphometric Study, J Indian Academy Forensic Med., 33(3): 0971-0973
2. Mishra SR, Singh PJ, Agarwal AK, Gupta RN (2003), Identification of Sex of Sacrum of Agra Region, J Anat. Soc. India, 52(2):132- 136
3. MM Patel, BD Gupta, TC Singel (2005), Sexing of Sacrum by Sacral index and Kimura’s Base Wing Index, J Indian Academy Forensic Med., 27(1):0971-0973
4. Standring Susan, Borley NR, (1988), Collins Patricia, Crossman AR et al, Gray’s Anatomy, 40th edition, London Press, 724 – 728, 1359.
5. Wilder HH (1920), A laboratory manual of anthropometry, P. Blakistons sons and Co. Philadelphia, 193.
6. Faweet E, (1938). The sexing of the human sacrum, Journal of Anatomy London, 72: 638.
7. Davivongs V (1963), The pelvic girdle of the Australian aborigines- Sex difference and sex determination, American Journal of Physical Anthropology, 21: 443-455.
8. Jit I, Singh S (1966), Sexing of the adult clavicle, Indian Journal of Medical Research, 54: 551-571.
9. Singh S, Gangrade KC (1968), Sexing of adult clavicle verification and applicability of demarking point, Journal of Indian Academy of Forensic Science, 7: 20-30
10. Singh H, Singh J, Bargotra RN (1988). Sacral index as observed anthropometrically in the region of Jammu, Journal of Anatomical Society of India, 37:1.
11. Singh, S, Raju PB (1977), Identification of sex from the hip bone-demarking points, Journal of Anatomical Society of India, 26 : 111- 117.
12. Jana TK, Koley T K, Saha SB, Basu D, Basu SK (1988), Variation and sexing of adult human sacrum, Journal of Anatomical Society of India, 37 : 2-3
13. Raju PB, Singh S, Padmanabhan R (1981), Sex determination and sacrum, Journal of Anatomical Society of India, 30 : 13-15
14. Comas J, Charles C, Manual of Physical anthropology (revised and enlarged English edition) 1961, Thomas Springfield, Illinois, USA, 415-416
15. Martin, Cited by Comas J, Manual of Physical Anthropology (1960) 2nd Edition, Charles C, Thomas Springfield, Illinois U.S.A., 415
16. Nagar S K, Study of sacral hiatus in dry human sacra, Anatomical Society of India (2004), 53(2): 18-21
17. Vinod Kumar, Pandey SN, Bajpai RN, Jain PN, Longia GS. Morpho-metrical study of sacral hiatus, Journal of Anatomical Society of India,(1992), 41 (1):7-13.
18. Trotter M .Variations of the sacral canal; their significance in the administration of caudal analgesia, Anaesthesia and analgesia, (1947), 26 (5): 192-202.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





