IJCRR - 4(20), October, 2012
Pages: 99-105
Date of Publication: 20-Oct-2012
Print Article
Download XML Download PDF
PREVALENCE OF OVERWEIGHT AND OBESITY AMONG ADOLESCENT SCHOOL GOING CHILDREN (12-15YEARS) IN URBAN AREA, SOUTH INDIA
Author: Prasanna Kamath B.T., Girish M. Bengalorkar, Deepthi R., Muninarayan C., Ravishankar S.
Category: Healthcare
Abstract:Background: Prevalence of overweight and obesity has increased for the past few decades. World Health Organization refers obesity as a global epidemic. There is a need to assess the prevalence and to find the factors responsible, so as to implement timely interventions. Aims: To assess the prevalence of overweight and obesity among school going children and the factors responsible for the same. Method: The study was conducted in children studying at a private school in Bangalore aged 12-15years. Obesity was assessed using International Obesity Task Force criteria based on the body mass index. Pretested and semi structured questionnaire was used to collect the data on physical activity, eating habits and leisure time activity. Results: The overall prevalence of overweight was 10% and obesity was 5% among 761 adolescents studied. The prevalence of overweight and obesity was 11% and 4% among boys and 9% and 5% among girls respectively. Factors like junk food, chocolate eating, physical inactivity and time spent in watching television and computer gaming were directly related to overweight and obesity. Conclusion: Overweight and obesity are multifactorial and needs a multi pronged interventions at the earliest for control and prevention.
Keywords: Overweight, Obesity, leisure time activity, Commutation, Body mass index, adolescence
Full Text:
INTRODUCTION
Childhood overweight and obesity are global problems that are on the rise.1 Obesity is one of the most prevalent nutritional diseases of children and adolescent in many developed and developing countries. During the past two decades, the prevalence of overweight and obesity in children has increased worldwide.2 Obesity in childhood and adolescence has adverse consequences on premature mortality and physical morbidity in adulthood.3 Outcome related to childhood obesity includes hypertension, type 2 diabetes mellitus, dyslipidemia, left ventricular hypertrophy, nonalcoholic steato-hepatitis, and obstructive sleepapnea, orthopaedic and psychological problems. Childhood obesity is associated with a higher chance of obesity, premature death and disability in adulthood. In addition to increased future risks, obese children experience breathing difficulties, increased risk of fractures, hypertension, and early markers of cardiovascular disease, insulin resistance and psychological effects.4 Once considered a problem of affluent developed countries, obesity is fast growing to enormous proportions in many developing countries also. Rapid economic growth has overcame the nutritional, socio-economic and health status of many countries.5 Obesity has increased markedly with this nutritional evolution in most Asian Countries. A similar nutritional transition is underway in India as well. In addition to the nutritional and socio-economic transitions, the behavioural transition of children is also possibly contributing significantly to the rapidly rising prevalence of obesity. Unhealthy eating habits and physical inactivity are the major culprits There is significant increase in the consumption of fats, sugars and energy rich foods. Rising income and urbanization leads to substitution of servants or appliances for physical household work and motor vehicles for short distance travelling, instead of walking or cycling.6 Junk food and fast food has replaced healthy homemade meals due to paucity of time. This attitude has altered the lives of school children in terms of bad eating habits, lack of exercise, habits like computer gaming and television viewing replacing the outdoor games. The causes of childhood obesity are multifactorial. Overweight and obesity in children and adolescent is generally caused by a lack of physical activity, unhealthy eating patterns resulting in excess energy intakes, or a combination of both.7 Changes in dietary and physical activity patterns are often the result of environmental and societal changes associated with development and lack of supportive policies in sectors such as health, agriculture, transport, urban planning, environment, food processing, distribution, marketing and education.8 Added to this, academic competitiveness, overzealous parents and teachers leave the children little or no time to play or exercise. Studies on urban Indian school children from selected regions report a high prevalence of obese and overweight children.9 Hence this study was undertaken to assess the prevalence of overweight and obesity among high school children (12-15years) and to determine the factors responsible for it.
METHOD Design:
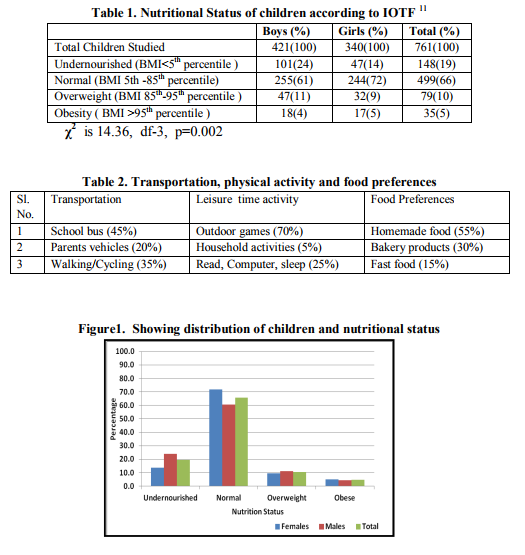
A cross-sectional study was conducted in a private school in an urban fast growing city, Bangalore. All the children belonging to 8th, 9th and 10th standard (12-15years) were included for the study. A prior informed consent for the study was taken from the school administration. Those children who were absent on those days of study were called on a separate day and a sincere effort was made to cover all children. Data regarding physical activity, leisure time activity, mode of commuting to school, food preferences, eating chocolates, fast food and junk foods, time spent for television viewing, computer gaming were collected using a pre-tested, semi-structured questionnaire. The anthropometric data, height and weight were also recorded for all the children using the standard equipments. Weight was recorded using a calibrated and standardized mechanical bathroom weighing scale to nearest 100grams. Height was recorded using the standard wall mounted anthropometric height board to the nearest 0.1 cm. Two readings of height and weight were taken and the mean was considered as final. BMI was calculated using the standard formulaweight (kilograms)/height (meter2 ) and BMI percentile was calculated according to Barlow SE and Expert Committee recommendations.10 Assessment of overweight and obesity: International Obesity Task Force (IOTF) classification was referred for the classification of the adolescent children as overweight or obese.11 Overweight was defined as children BMI value between 85th -95thpercentile for a specific age and gender. Similarly obesity was defined as with BMI value above 95th percentile for that specific age and gender. On completion of the study, we provided health education and created awareness regarding overweight and obesity, their implication on their health and how they can inculcate healthy lifestyle practices. Statistical analysis Sample size was calculated as 788 considering the prevalence of overweight as 17.8% and e=2.67 as in the study.12 The data collected was collated using Excel spreadsheets with double checking of errors. The results were assembled in tabular and graphical formats. All data was expressed as percentage. Comparison of nutritional status between boys and girls was done by using chi square test. P <0.05 was considered statistical significant. RESULTS A total of 761 children in the age group of 12- 15years were included in the study. Among them 421children (55.32%) were boys and 340 (44.68%) were girls. The Table 1 depicts the summary of the assessed children’s BMI for age and their classification into those who are overweight and obese as per International Obesity Task Force (IOTF).11 On the whole there were 10% (76) of the children who were overweight i.e. BMI value equal to or more than 85th percentile but less than 95th percentile for that age and sex. There were 5% (38) children who were obese i.e. BMI value equal to or more than 95th percentile for that age and sex. Another incidental point of note worth is the presence of 19% of undernourished children. The prevalence of overweight 11% among boys and 9% among girls and 4% and 5% were obese respectively, according to IOTF.11 As observed in table1, the difference in the nutritional status among boys and girls was statistically significant. (p=0.002). But the difference in overweight and obesity among them was found to be not significant statistically. Data regarding the leisure time activity during games period at school, after school at home and on holidays, revealed that 70% of the children involved in playing outdoor games while among the remaining 5% were involved in household activities and the rest spent time either reading, gaming on the computer or sleeping. Regarding the mode of transportation from home to school and back 45% used school bus, 20% were dropped by their parents in their own vehicles and the remaining walked or came by cycling. About 55% of children brought home made food for lunch, while 30% brought bakery products and the remaining ate at the fast food centres near their school.
DISCUSSION
The overall prevalence of overweight among children was 10% and obesity was 5%. The prevalence of overweight was 11% among boys and 9% among girls; 4% and 5% were obese respectively. In a study by Kotian MS et. al, it was reported that prevalence of overweight was 9.9% and obesity was 4.8%.13 They also reported that overweight and obesity among boys was 9.3% and 5.2% and among girls was 10.5% and 4.3%. Our study reflects similar findings. A similar study in Hyderabad showed that the prevalence of overweight was 7.2% among 12-17year group.14 In this study, it was observed that there was not much difference in the prevalence of overweight and obesity between genders. It was 11% and 4% for boys and 9% and 5% for girls, respectively. Prevalence of overweight and obesity was more in the males as compared to females in the studies conducted at Delhi, India14 and Punjab.9 Prevalence of overweight was 14.3% among boys and 9.3% among girls and obesity was 2.9% in boys as compared to girls which was 1.5% as reported by Ramesh Goyal et al.8 The presence of overweight and obesity on almost same level in our study may be attributed to the equal amount of encouragement and participation of both girls and boys in the physical activities. This is to be appreciated on the part of the school administration in inculcating this attitude. One of the major reasons for childhood obesity was watching television, using computers for long durations instead of outdoor games. Physical activity during leisure period either at school or at home was found to be related inversely to overweight and obesity. Children with outdoor game activity in association with good eating habits were found to be healthy and protected from obesity and overweight. Similar reports were given by a study by Kotian MS et al 13, Laxmaiah A et al at Hyderabad 14 and Eisenman JC et al in US 16 Supreet et al in a study at Punjab.9 Moazeri H et. al reported that the analysis of association between BMI and physical activity in children revealed that as the amount of physical activity increased the prevalence of overweight and obesity decreased in Tehran17 and similar findings were reported by Foldmark CE et al18 Kelishadi R et al.19 In our study as in table 2, 70% of the children have mentioned that one of the chief passtime is television viewing. Similarly Bar-or O et al have reported that the sedentary lifestyle of children and adolescents has been attributed to television viewing, computer games, internet, overemphasis on academic excellence and ever increasing automated transport.20 The habit of eating chocolates and junk food was more in those who were overweight and obese than other children. This is similar to the one reported by Ramesh K Goyal et al.8 In their study they have stated that junk food and chocolate eating habit have positive relation with prevalence of obesity and overweight. These correlate well with previous reports which suggest that junk food(bakery items, pizza, burger, cheese, butter, oily items) and chocolate intake tends to be more common among overweight and obese adolescents than among normal weight adolescents.21,22 A study by Bhave S et al have reported that food in urban areas has been replaced by high calorie snacks and junk foods and also that unsafe roads, lack of free space for playing and increased television viewing and computer use has made life sedentary comparable this study.23 Some of the children who were obese were found to be academically low achievers, rarely mingled with others and spent most of their free time sleeping, eating junk food or reading nonacademic books. This may be either their low achieving nature clubbed with eating habits made them obese or it may be that the combination of obese, loneliness made them low achievers- point which needs further study. The best measure available to prevent and protect the child from overweight and obesity is to start at their young age itself, for the dietary habits and practices instilled at their young age will last their entire lifetime. Limitations of this study- In our study waist-hip ratio and skin fold thickness were not used for assessing the nutritional status of overweight and obesity, the application of international standards of BMI in an Indian setting may have limitations. Quantification of physical activity and calorie intake could have been done before correlating with overweight and obesity. Information regarding the parents’ and familial history of overweight and obesity could have been considered.
CONCLUSION
To conclude, among the 761 children in the study, the overall prevalence of overweight was 10% and obesity was 5%. Overweight and obesity were 11% and 4% among boys and 9% and 5% among girls respectively. The prevalence was high among children who were physically inactive, using motor vehicles for commuting, eating junk foods, chocolates and those who were spending more time indoor either watching television or computer gaming. This problem of obesity and overweight is truly a multifactorial one.
The obese adolescents reach adulthood and add to the spiralling problem of diabetes, heart disease and hypertension. The impact of this on the health scenario of our country will be devastating and alarming. Obesity does not have any mentioning in the nutritional health status of school children, may be, due to the large number of undernourished children in our country even to this day of commendable growth and development in other fields. Unless effective interventions and preventive strategies are initiated at the local and national level, the present increasing trend of obesity suggests that the trend of increasing cardiovascular diseases in adults observed in the recent decades will increase even further. This calls for concerted effort targeted at improving lifestyles of children and adolescents. It is appropriate time that both under-nutrition and over-nutrition are given equal importance during health assessment of children annually. Measures have to be taken to improve the dietary habits which last, life time if imparted and implemented at young age itself. The physical growth and development has to be made a part of the overall personality development on par with academic excellence. If done at the earliest with right earnest, our children can grow up into healthy young adults with better health indices and parameters for a better India.
ACKNOWLEDGEMENTS
We would like to thank the head of the institution, the teachers and more so the students for having been very co-operative in the collection of the data. We thank our entire department faculty for being encouraging and supportive throughout this study. Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. No financial funding was taken for preparation of this manuscript.
ETHICS COMMITTEE APPROVAL
Name of committee- Institutional Ethics Committee of Sri Devaraj Urs Medical College, Kolar, Karnataka, India. Approval reference number- No: DMC/KLR/MEU/IECCER/229/2011-12. DATED 16-05- 2012.
References:
1.World Health Organization. Preventing chronic diseases. A Vital investment. World Global Report.Geneva: World Health Organization; 2005. (Accessed January 4, 2010, at http://www.who.int/chp/chronic_disease_report /full_report.pdf)
2. De Onis, M.; Lobstein, T. Defining obesity risk status in the general childhood population: Which cut-offs should we use? Int J Pediatr Obes 2010; 5: 458-60.
3. Reilly, J.J.; Kelly, J. Long-term impact of overweight and obesity in childhood and adolescence on morbidity and premature mortality in adulthood: Systematic review. Int J Obes 2011; 35: 891-98.
4. Raj M, Sundaram KR, Paul M, Deepa AS, Kumar RK. Obesity in Indian children: Time trends and relationship with hypertension. Natl Med J India 2007; 20:288-93
5. WHO Technical Report Series 916. Diet, nutrition and prevention of chronic diseases. Geneva: WHO; 2003. (Accessed January 4, 2010, at http://whqlibdoc.who.int/ trs/who_trs_916.pdf)
6. Waker H. Simple obesity in children. A study on the role of nutritional factors. Med Wieku Rozwoj 2006; 10:3-191.
7. US Department of Health and Human Services. Childhood Obesity. (Accessed January 4, 2010, at http://aspe.hhs.gov/health/reports/child_obesity /htm)
8. Goyal RK, Shah VN, Saboo BD, Phatak SR, ShahNN, Gohel MC, et al. Prevalence of overweight and obesity in Indian adolescent school going children: Its relationship with socio- economic status and associated lifestyle factors. J Assoc Physicians India 2010; 58:151- 58.
9. Chhatwal J, Verma M, Riar SK. Obesity among pre-adolescent and adolescents of developing country(India). Asia Pac J ClinNutr 2004; 13:231-5
10.Barlow SE. Expert Committee recommendations regarding the prevention, assessment and treatment of child and adolescent overweight and obesity: Summary report. Pediatrics 2007; 120 (suppl 4):164-92.
11.Cole JC, Mary CB, Katherine MF, William HD. Establishing a standard definition for child overweight and obesity worldwide: International survey. Br Med J 2000; 320: 1240-43.
12.Prevalence of overweight in urban Indian adolescent school children’ by Ramachandran A et al published in Diabetes Research and Clinical Practice Volume 57, Issue 3, Page 185-190, September 2002.
13.Kotian MS, Kumar SG, Kotian SS. Prevalence and determinants of overweight and obesity among adolescent school children of South Karnataka, India. Indian J Community Med 2010; 35:176-8.
14.Laxmaiah A, Nagalla B, Vijayaraghavan K, Nair M. Factors affecting prevalence of overweight among 12-17year old urban adolescents in Hyderabad, India. Obesity 2007; 15:1384-90.
15.Supreet Kaur, Sachdev HRS, Dwivedi SN, Lakshmy R, Kapil U. Prevalence of overweight and obesity amongst school children in Delhi, India. Asia Pac J Clin Nutr 2008; 17:592-96.
16.Wiseman JC, Bartee RT, Wang MQ. Physical activity, television viewing and weight in US youth: Youth risk behavior survey. Obes Res 1999; 10:379-85.
17.Moazeri H, Bidad K, Zadhoush S, Gholami N, Anari S. Increasing prevalence of iron deficiency in overweight and obese children and adolescents (Tehran Adolescent Obesity study). Eur J Pediatr 2006; 165:813-14.
18.Foldmark CE, Marcus C, Britton M. Interventions to prevent obesity in children and adolescents: a systematic literature review. Int J Obes 2006; 30:579-89
19.Kelishadi R, Pour MH, Sarraf-Zadegan N, Sadry GH, Ansari R, Alikhassy H, et al. Obesity and associated modifiable environmental factors in Iranian adolescents. Isfahan Healthy Heart Program-Heart Health Promotion from Childhood. Pediatr Int 2003; 45:435-42
20.Bar-Or O, Foreyt J, Bouchard C, Brownell KD, Dietz WH, Ravussin E,et al. Physical activity, genetic, and nutritional considerations in childhood weight management. Med Sci Sports Exerc 1998, 30:2-10
21.Klesges RC, Klesges LM, Shelton ML. A longitudinal analysis of accelerated weight gain in preschool children. Pediatrics 1995; 95:126- 30.
22.Wolfe WS, Campbell CC, Frongillo EA, Haas JD, Melink TA. Overweight school children in NewYork state: prevalence and characteristics. Am J Public Health 1994; 84:807-13
23.Bhave S, Bavdekar A, Otive M. IAP National task force for childhood prevention of adult disease; Childhood Obesity. Indian Paediatr 2004; 41:559-75.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





