IJCRR - 4(20), October, 2012
Pages: 94-98
Date of Publication: 20-Oct-2012
Print Article
Download XML Download PDF
CLINICAL OUTCOMES OF AO PHILOS PLATING FOR PROXIMAL HUMERUS FRACTURES
Author: Annamalai Regupathy
Category: Healthcare
Abstract:This was a retrospective analysis study done to identify the results of Philos plating for the proximal humeral fractures. The analysis was done on 11 patients with fracture to proximal humerus. The clinical and functional outcome based on X ray, Constant score, DASH score were analyzed and complications were studied in detail and discussed with literature following which the conclusions were made in this study.
Full Text:
INTRODUCTION
Trauma to proximal humerus often presents a real challenge to orthopedic surgeons (Peter S Rose et.al). It accounts for 2% to 3 % of all fractures to upper limb and treatment is controversy. There are various treatment options from non surgical to surgical management with numerous implants. There is no clear evidence from the literature to state the optimal method of surgery and the best implant. Wide ranges of internal fixation devices are available for treating the proximal humeral fractures (Bjorkenheim JM et.al). The latest addition in the implant list is AO Philos plate which is an anatomically contoured rounded plate with combined holes, which will allow a case specific adaptable treatment for fractures of the proximal humerus (Baker P N et.al). The principal advantage of this system is that it provides improved fixation using multiple screws at divergent angles which are locked to the plate via a thread in the screw head and a matching thread in the screw hole in the plate. Whilst the fixed angle locking screw design of the plate has been designed to improve the quality of fixation in osteoporotic bone, there have been reports in the literature of failure of fixation using the Philos plate (D M Wright et.al).
AIM AND OBJECTIVES:
The main aim of the study is to in investigate the clinical outcomes after Philos plating for proximal humeral fractures with the Objectives 1) To perform a retrospective analysis on cohort of patients who have had internal fixation for proximal humeral fractures with Philos plate.2) To determine clinical outcome in terms of pain relief and function, using appropriate scoring systems. 3) To determine the incidence of implant failure and complications with this procedure.
MATERIALS AND METHODS
The study was carried out in Ninewells Hospital during June 2003 to March 2007. The planed detail of the study was submitted for Caldicott approval and University of Dundee’s Code of Practice for Research Ethics on Human Participants committee approval. There were total of eleven patients in the study. The inclusion criteria were 1) Fractures with skeletal maturity 2) Delayed presentation 3) Closed fractures and 4) Osteoporotic fractures. The exclusion criteria were 1) Open fractures 2) Fractures without skeletal maturity and 3) Pathological fractures. Fractures were classified following Neers classification. Out of the eleven patients, nine were females and three were males. The mean age in the study group was 54.4 years and ranged from 17 years to 81 years. In the above selected patients the nature of injury, the fracture pattern, neurovascular deficit and any previous significant history of hospitalization were recorded in a proper performa. Patients underwent surgery either under regional, general or combined anaesthesia. Fracture was approached through the deltopectoral approach. Long 5 holed plate or short 3 holed Philos plate was used. Standard post operative physiotherapy protocol was followed in the study. Patients were followed up till the fracture union. X rays were taken to evaluate the radiological union and Constant score, DASH score were followed to assess the functional outcome.
RESULTS
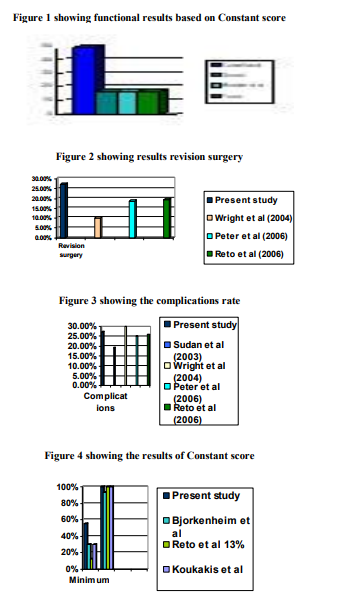
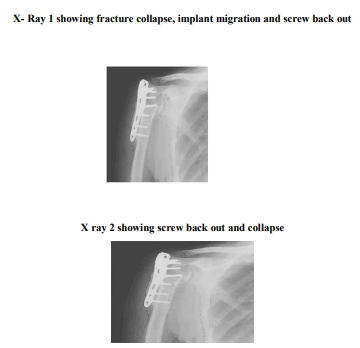
There were total of 11 patients in which 9 were females and 2 were males. The age group in the study was from 18 years to 81 years with mean of 54.45 years. The maximum age incidence was between 41 years to 60 years. There were 8 patients with 2 part fractures and 3 patients with 3 part fractures. Ten patients had fracture on right side and one patient had fracture on left side. The commonest mechanism of injury was following trivial trauma like fall with out stretched hand in old population and in younger group the mode of injury was following high velocity injury. All the patients were taken for surgery and fracture was approached through deltopectoral approach. For seven patients 3 holed Philos plate was used to fix the fracture and for four patients 5 holed Philos plate was used. Patients were regularly followed up till fracture union. Physiotherapy was started from second post operative day. There were complications seen in three patients. They included impingement of screws, loss of abduction, continuous pain, collapse of head and implant back out (X-ray 1 and 2). All these patients underwent implant removal. The functional outcome was measured based on Constant score and DASH score. The mean Constant score was 81.16 with minimum of 55 to maximum of 100 (Figure 1). The results based on Constant score was classified as excellent of 50% cases, 16.6% of good result, 16.6% of moderate and 16.6% of poor results. The mean DASH score was 13.03 with minimum of 0.83 to maximum of 41.9.
DISCUSSION
The results of the present study were compared with various literatures. The sex incidence, age incidence were compared with Peter et al. 1 series, Baker et al. 2 study, Bjorkenheim et al. 3 , Reto et al. 4 study. The total revision surgery (Figure 2) rate in the present study was 27.27%. Reto et al.4 reported 25.94 % of complications (Figure 3) which included loss of reduction, screw perforation, loosening, implant breakage and avascular necrosis. There revision surgery rate was 19.6%. The complications rate reported by Sudan et al.5 was 19.34% and included implant breakage, avascular necrosis and non union. Wright et al.6 reported 30% of fracture collapse and 10% of revision surgery. Peter et al.1 reported 25% of complication rate in their study and 18.75% of revision surgery rate. . The mean constant score in the study was 81.16 which ranged from 55 to 100. There were 50% excellent result, 16.6% good result, 16.6 % moderate result and 16.6% poor result. The mean Constant score in Bjorkenheim et al.3 series was 73 which ranged from 30 to 93. The mean Constant score in Reto et al.4 series was 73 and ranged from 13 to 100. In the study reported by Koukakis et al7 . the mean Constant score was 76.1 and ranged from 30 to 100 (Figure 4). The mean DASH score in the study was 13.03 with the minimum of 0.83 and maximum of 41.9. The mean DASH score in Baker et al. (2004) study was 33.9 and ranged from 4 to 92.
CONCLUSION
From the present retrospective study following conclusions may be drawn
1) Proximal humeral fractures are difficult fractures to treat and that even though with the fixed angle screw system on the plate has been designed to avoid cut out in osteoporotic bone, the failure rate is high (about 30%).
2) Due to the spherical shape of the humeral head with 2-D screening there is risk of penetration of screws into the glenohumeral joint.
3) It is a technically demanding surgery thus a longer learning curve.
4) The results are similar to the published literature in terms of complication rates. Limitations in the study: The present study is from a small group with less follow up sample. Further recommendation: A further multi centric study with large group with more representation in all age group and a comparative study with other procedures may be necessary for better conclusion.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. I extend my sincere thanks to Dr L Cochrane, Mr. David Nicoll, Mr. C A Wigderowitz and Prof J Abboud, Department of Orthopaedics, Ninewells hospital, University of Dundee, UK for their esteemed guidance and untiring help during the study.
References:
1. Peter S Rose, Christopher R Adam and Michael E Torchin. Locking plate fixation for proximal humerus fractures, initial result with new implant. J shoulder and elbow surgery, 2007. March-April:16(2) 202-7.
2. Baker P N, Candal Couto J, Ranan A and Bennison K. Clinical outcomes followingPhilosplatefixationproximalhumerus,f ractures,www.bess.org.uk/meetings/archive.asp ?aspyear=2005andabstract=218
3. Bjorkenheim JM, Pajarinen J and Savolaine V. Internal fixation of proximal humerus fractures with locking compression plate, Acta Orthop Scand December 2004; 75(6): 741-745.
4. Reto H Babst, Christoph Sommer, Christian Bahrs, Rainer Heuwinkel, Christain Hafner, Parvo Rillman, George Kohut and Mathias Muller, Open reduction and internal fixation of proximal humerus fractures with an angular stable form plate, www.hwbf.org/ota/am/ota06/otapa/OTA06126 5.htm
5. Marc Saudan, Richard E Stern, Anne Lubbeke, Robin E Peter and Pierre Hoffmeyer. Fixation of fractures of the proximal humerus: Experience with a new locking plate, www.hwbf.org/ota/ota3/otapa/OTA03634.htm
6. D M Wright, A Acharya, R H Austin and J C Kaye. Complications and suggestions encountered with the philos plating system, J Bone Joint surgery 2004; 87-B:165e.
7. Koukakis Athanasios, Apostolou Constantinos, Taneja Tarun. Fixation of proximal humeral fractures using the philos plate, early experience, Clinical orthopaedics and related research 2006; 115-120.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





