IJCRR - 4(22), November, 2012
Pages: 140-145
Date of Publication: 24-Nov-2012
Print Article
Download XML Download PDF
ISOLATED PANCREATIC INJURY FOLLOWING BLUNT TRAUMA ABDOMEN
Author: A. Ramesh, C.P.Ganesh Babu, Sudeepta Kumar Swain, K.Raghuram, T.Tirou Aroul
Category: Healthcare
Abstract:A 27-year-old male presented with the complaints of abdominal pain and distension for two weeks following blunt abdominal trauma. Abdominal examination revealed a large tender mass in epigastrium, Left hypochondrium and lumbar regions. Contrast Enhanced Computed Tomography (CECT) imaging showed Necrotic pancreatitis. He was initially managed conservatively for a period of five weeks. As patients general condition worsened with increasing abdominal pain and significant weight loss, he was subjected to Laparotomy and Necrosectomy. Patient developed high output pancreatic fistula, which was managed conservatively for a period of six weeks with Partial Parentral Nutrition and Endoscopic Retrograde Cholangio Pancreatogram (ERCP), was done which was not contributory. This case report is presented for an uncommon presentation of isolated pancreatic injury following blunt trauma abdomen.
Keywords: Pancreas, Necrosectomy
Full Text:
INTRODUCTION
Pancreatic and biliary injuries are uncommon but may be associated with high morbidity and mortality, particularly if diagnosis is delayed. Pancreatic and biliary injuries may be more subtle. Moreover, these injuries may be overlooked in patients with extensive multiorgan trauma. Isolated pancreatic injuries are rare, occurring in less than 2% of blunt abdominal trauma patients, and associated injuries, especially to the liver, stomach, duodenum, and spleen, occur in over 90% of cases. Symptoms and clinical findings are often non-specific and unreliable. Imaging will show evidence of pancreatic injury. The main source of delayed morbidity and mortality from pancreatic trauma is disruption of the pancreatic duct.
Imaging Findings in Pancreatic Injuries Due to Blunt
Trauma Direct findings
Pancreatic enlargement, Laceration (focal linear non enhancement), Comminution Inhomogeneous enhancement
Secondary findings Peripancreatic fat stranding Peripancreatic fluid collections, which may communicate with a laceration Fluid between the splenic vein and pancreas Hemorrhage Thickening of the left anterior pararenal fascia Associated injuries to adjacent structures
Case Report
A 27-year-old male patient with complaints of abdominal pain, abdominal distension and fever for the past two weeks. He gave a history of blunt trauma (injury during a fist fight) 2 weeks prior to admission. He consumes alcohol occasionally for 5 years. On examination, patient was haemodynamically stable. Per Abdomen: A large tender fixed mass present in epigastrium, left hypochondrium and lumbar region. No evidence of peritonitis. Chest: Features of Right lower zone consolidation with pleural effusion. Clinical Impression: Traumatic Pancreatitis with Pseudocyst.
Investigations
Serum Amylase – 51 IU/L, Serum Calcium – 7.9 mg/dl; Complete Blood Count, Renal Function Test, Liver Function Test, Serum Electrolytes – Within Normal Limits
Ultra Sonogram Abdomen
Minimal free fluid in abdomen, Thickened omentum, Bowel distended, Bilateral pleural effusion Right > Left, Pancreas obscured by poor window.
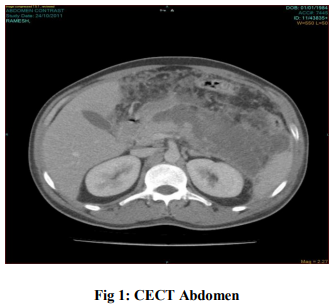
Contrast Enhanced Computed Tomography (CECT) Abdomen
Acute Necrotizing Pancreatitis with Retroperitoneal fluid collection Minimal ascites, bilateral pleural effusion Patient managed conservatively with IV antibiotics and proton pump inhibitors. Follow up Contrast Enhanced Computed Tomography Abdomen after 3 weeks: Necrotic pancreatic parenchyma in the body and tail with localized pancreatic fluid collection and Left Pleural Effusion. Mild resolution of inflammatory changes compared to previous CT. Patient’s condition improved and discharged after 10 days Final Diagnosis: Traumatic acute necrotizing pancreatitis 10 days later, patient was readmitted for persistent pain. Abdominal examination showed large tender mass in epigastrium, left hypochondrium and lumbar regions. Investigations Hemoglobin: 9.5 gm/dl, Total Count: 16,700 cells/cu.mm, Differential Count: N70L23E3, Serum Calcium: 8.9 mg/dl; Serum Amylase: 76 IU/L, Renal Function Test, Serum Electrolytes, Liver Function Test: Within Normal Limits, Blood Culture and Sensitivity – Sterile.
Ultra Sonogram Abdomen
Heterogeneous appearing mass in body and tail region of Pancreas? Infected cyst, Minimal ascites, Left pleural effusion. Patient first managed conservatively but the symptoms were worsening with weight loss and fever. He was subjected to exploratory laparotomy.
Operative Findings
• Plastered peritoneal contents with thick adhesions
• Frank pus draining from lesser sac.
• Cavity extending to left paracolic gutter.
• Necrosis of the body and tail of pancreas.
• Pancreatic duct shows no evidence of disruption.
Pancreatic Necrosectomy was done. Two 30F drains were put into the necrotic bed. Pus Culture revealed Acinetobacter Spp. IV antibiotics were started as per Culture and Sensitivity.
Drain Fluid Amylase
Post Operative Day 4 - 9,940 U/L, Post Operative Day 12 - 40,300 U/L, Post Operative Day 32 - 815 U/L (30-40 ml/day) Subsequent Culture revealed Klebsiella pneumoniae and E.coli showing sensitivity to Ciprofloxacin.
Post Operatively
Fistulogram revealed residual blind ending tract in the left upper abdomen with no evidence of communication to Pancreatic Duct. Patient managed conservatively with Partial Parentral Nutrition and Endoscopic Retrograde Cholangio Pancreatogram (ERCP) was done which was not contributory.
Follow Up
- Post Operative Day 50 - Drain fluid 10 ml/day, Drain removed
- Post Operative Day 60 - Wound healthy, Patient discharged
- Post Operative Day 75 - Patient came for follow up, No specific complaints, Good weight gain (5 kg in 1 month)
DISCUSSION
Injury to the pancreas after blunt abdominal trauma is less frequent than that of other solid organs, such as the liver and spleen. Pancreatic injuries occur in less than 2% of all patients with abdominal trauma. Penetrating injuries are three to four times more common than blunt injuries (1) . Pancreatic injuries are usually associated with injuries to adjacent organ and major vascular structure. Mortality due to blunt trauma is about 15-50%. Mostly death results from the hemorrhage from nearby vascular structures (2) . Second most common cause of death is delayed mortality from intra-abdominal sepsis. Frequently noted in the history in traumatic pancreatitis is impact of the epigastric area of the patient with the steering wheel of a car in head-on collision. Cyclists involved in accidents are peculiarly liable to pancreatic injury, the blow to the abdomen being delivered by the handlebars or direct blow by assault. Pancreatic contusion is generally believed to involve rupture of minor or major components of the duct apparatus with consequent effects due to activity of liberated enzymes. The area of the pancreas most likely to be damaged as a result of a blow or crushing force is that which overlies the vertebrae (3).Although the middle segment of the pancreas is the most vulnerable, injuries of the head and the tail do occur. Typical mode of trauma is the clue and high index of suspicion is required to diagnose the pancreatic injury (4). They present with mild epigastric pain, abdominal tenderness or other non-specific abdominal findings. Investigations will show increased hematocrit, Increased Total Leukocyte Count, absent psoas shadow in plain x-ray abdomen. Serum amylase has been claimed to be neither sensitive nor specific in the diagnosis of pancreatic injury (5) . Serum amylase is increased in 90% case of pancreatic trauma (6) . Even if elevated, there is no correlation to the severity of the injury (7) . Contrast-enhanced computerized tomography (CE-CT) has been used to predict the severity of an attack of acute pancreatitis (8).The presence of gas within an area of necrosis shown by CE-CT is highly suggestive of infection. Management: The management of patients with blunt pancreatic injuries should be individualized. Selected patients with stable abdominal signs without pancreatic ductal injuries may be carefully observed. Any deterioration of clinical situation or demonstration of pancreatic ductal injury should mandate an exploratory laparotomy. The treatment has to be tailored to individual situations especially in patients with severe concomitant injuries. 1. Initial Management: Pancreatic injuries rarely occur alone and are often associated with other intra-abdominal injuries. Hence, these patients must be managed as all other trauma patients with the aim of ensuring hemodynamic stability first before any specific treatment of the pancreatic injuries if such treatment is required (9) . 2. Antibiotics: The gastrointestinal tract is thought to be the major source of organisms infecting necrotic pancreatic tissue. Increased translocation of bacteria and toxins is known to occur in acute necrotizing pancreatitis (10,11) . Prophylactic antibiotic use may reduce the incidence of septic complications particularly infection involving areas of pancreatic necrosis (12,13). In a recent prospective trial (14), the incidence of gram-negative pancreatic infection and late mortality (deaths more than two weeks after the onset of pancreatitis) were significantly reduced in patients with necrotizing pancreatitis who were treated with selective gut decontamination (14) . 3. Nutrition: Early introduction of nutrition via the gastrointestinal tract may also help to restore mucosal integrity and reduce bacterial translocation. A number of studies in patients with major trauma, surgery and burns showed that enteral nutrition significantly decreased the acute phase response and incidence of septic complications when compared with total parenteral nutrition. It can be concluded that enteral nutrition is safe in patients with severe acute pancreatitis and there is some evidence that it may be preferable to parenteral nutrition (15) . 4. ERCP: ERCP is an invaluable tool in the overall management of pancreatic trauma. In the early stages or pre-operatively, it is able to provide real-time diagnostic images and allow guided intervention. It can even be performed intraoperatively or in the late stages of pancreatic trauma. Through its interventional ability by placement of an endoscopic stent, major surgery can be averted even in the presence of pancreatic ductal injuries. ERCP is also useful in managing post-injury or post-operative complications. Pseudocysts, pancreatic fistulae and chronic pancreatitis are some of these conditions, which could be diagnosed and managed endoscopically without major surgery (16, 17) . 5. Non-Surgical management: Sterile pancreatic necrosis should initially be managed nonoperatively. Non-surgical management, including early antibiotic treatment, should be used in all patients with sterile pancreatic necrosis (18). In contrast other authors have observed a similar mortality in patients undergoing necrosectomy between those with sterile and those with infected necrosis(19) . 6. Surgical management: Timing of surgery is critical. Necrosectomy is technically difficult during the first week but becomes progressively easier with time (20) .
The Aims of Operative Management
- To control hemorrhage
- Treatment of other associated injuries
- Debridement of non-viable tissues
- Preservation of maximal viable tissues
- Adequate drainage of exocrine pancreas
Indications for surgical intervention Absolute:
Presence of infected pancreatic necrosis shown by CE-CT or FNAB. Relative: In a patient with >50% pancreatic necrosis, failure to improve appreciably after 2 - 3 weeks, unexplained deterioration, or a suspicion of infected pancreatic necrosis even in the absence of firm evidence on CE-CT and FNAB. Necrosectomy has traditionally been undertaken by an open route (21). Following laparotomy the lesser sac is opened if possible, the colon is mobilized downwards and the pancreas identified. Necrotic pancreas is debrided by blunt finger dissection and wide bore suction drainage. If opening of the lesser sac is not possible, direct access from the infracolic compartment via the left transverse mesocolon (Space of Riolan) is an alternative. Adequate debridement is usually achieved with a single visit to theatre. Any associated fluid collections are drained by the most direct route. Large drains and irrigating catheters are left within the retroperitoneal area and continuous irrigation is continued post surgery (21) . In addition, the longer surgical intervention can be delayed after the onset of acute necrotizing pancreatitis, the better survival is, probably because of improved demarcation between viable and necrotic tissue at the time of operation. The role of delayed necrosectomy (after the resolution of multisystem organ failure) in patients with sterile acute necrotizing pancreatitis also remains controversial. Some investigators advocate debridement in patients who remain systemically ill four to six weeks after the onset of acute pancreatitis, with fever, weight loss, intractable abdominal pain, inability to eat, and failure to thrive (22,23) .
Outcome
Operative outcome of necrotizing pancreatitis is related to the timing of surgery; the later the surgery, better the outcome. In a stable uncomplicated patient, delaying surgery may decrease the morbidity of an attack (24) .
CONCLUSION
Trauma accounts for approximately 2 - 4 per cent of cases of acute pancreatitis. Following an upper abdominal injury, acute pancreatitis should always be suspected. Isolated pancreatic injuries are rare in blunt trauma abdomen, patient usually present late, can be diagnosed if suspicion is high based on mode of trauma and CECT abdomen. A latent period may intervene before appearance of symptoms. Operation is not necessary in all cases of pancreatitis following injury. The conservative nonoperative management which has greatly reduced the mortality in the usual types of pancreatitis is advocated for cases following nonpenetrating abdominal injury, if serious injury to other organs and massive hemorrhage can be ruled out. Indications for surgical intervention are penetrating wounds, injury to the important blood vessels, injury to adjacent viscera as spleen, liver or gastro-intestinal tract, and failure to respond promptly to conservative management or for subsequent pancreatic collections. If one cannot diagnose the exact grade of injury preoperatively or intraoperatively, conservative surgery is the best option, but in appropriately selected patients, pancreatic resection can be performed with good results.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Hendel R, Rustrals CH. Management of pancreatic trauma. Can J Surg 1985;28: 359- 62.
2. Ivatury R, Nallathambi M, Rao P. Penetrating pancreatic injuries. Analysis of 103 consecutive cases. AmJ Surg 1990; 56: 90- 93.
3. Howard, J. M.: Surgical physiology of pancreatitis, S. Clinics of No. America, 29:1789-1800, Dec. 1949. Ivy, A. C., Gibbs, G. E.: Pancreatitis: A review, Surgery, 31:614-642, April 1952.
4. Craiq MH, Talton DS, Hanser CJ, Poole GV. Pancreatic injuries from blunt trauma. Ann Surg 1995; 61(2): 25-28.
5. Olsen WR. The serum amylase in blunt abdominal trauma. J Trauma 1973;13:200- 204.
6. Bradley EL 3rd, Young PR Jr, Chang MC, et al. Diagnosis and initial management of blunt pancreatic trauma:guideline from a multiinstitutional review. Ann Surg 1998;227(6): 861-69.
7. Buechter KJ, Arnold M, Steele B, Martin L, Byers P, Gomez G, Zeppa R, Augenstein J. The use of serum amylase and lipase in evaluating and managing blunt abdominal trauma. Am Surg 1990; 56:204-8.
8. Nordestgaard AG, Wilson SE, Williams RA. Early computerized tomography as a predictor of outcome in acute pancreatitis.Am J Surg, 1986;152:127-132.
9. Miller PR, Croce MA, Bee TK, Malhotra AK, Fabian TC. Associated injuries in blunt solid organ trauma: implications for missed injury in nonoperative management. J Trauma 2002; 53:238-42.
10. Runkel NS, Moody FG, Smith GS, Rodriguez LF, LaRocco MT,Miller TA. The role of the gut in the development of sepsis in acute pancreatitis. J Surg Res, 1991;51:18- 23.
11. Wang X, Andersson R, Soltesz V, Leveau P, Ihse I. Gut origin sepsis, macrophage function, and oxygen extraction associated with acute pancreatitis in the rat. World J Surg, 1996;20:299-308.
12. Howes R, Zuidema GD, Cameron JL. Evaluation of prophylactic antibiotics in acute pancreatitis. J Surg Res, 1975;18:197- 200.
13. Finch WT, Sawyers JL, Shenker S. A prospective study to determine the efficacy of antibiotics in acute pancreatitis. Ann Surg, 1976;183:667-671.
14. Luiten EJ, Hop WC, Lange JF, Bruining HA. Controlled clinical trial of selective decontamination for the treatment of severe acute pancreatitis. Ann Surg 1995;222:57-65.
15. Moore EE, Felaciano DV, Andrassay RJ. Early enteral feeding compared with parenteral reduces postoperative septic complications: the results of a Meta analysis. Ann Surg, 1992;216:172-183.
16. Thomas H, Madanur M, Bartlett A, Marangoni G, Heaton N, Rela M. Pancreatic trauma--12-year experience from a tertiary center. Pancreas 2009; 38:113-6.
17. Kim HS, Lee DK, Kim IW, Baik SK, Kwon SO, Park JW, Cho NC, Rhoe BS. The role of endoscopic retrograde pancreatography in the treatment of traumatic pancreatic duct injury. Gastrointest Endosc 2001; 54:49-55.
18. Rau B, Pralle U, Uhl W, Schoenberg MH, Beger HG. Management of sterile necrosis in instances of severe acute pancreatitis.J Am Coll Surg, 1995;181:279-288.
19. Fernandez-del-Castillo C, Rattner DW, Makary MA, Mostafavi A, McGrath D, Warshaw AL. Debridement and closed packing for the treatment of necrotizing pancreatitis. Ann Surg, 1998; 228:676-684.
20. Mier J, Leon EL, Castillo A, Robledo F, Blanco R. Early versus late necrosectomy in severe necrotizing pancreatitis. Am J Surg,1997;173:71-75.
21. Beger HG, Büchler M, Bittner R, Block S, Nevalainen T, Roscher R. Necrosectomy and postoperative local lavage in necrotizing pancreatitis. Br J Surg, 1988;75:207-212.
22. Rattner DW, Legermate DA, Lee MJ, Mueller PR , Warshaw AL. Early surgical debridement of symptomatic pancreatic necrosis is beneficial irrespective of infection. Am J Surg 1992;163:105-10.
23. Ho HS, Frey CF. Gastrointestinal and pancreatic complications associated with severe pancreatitis. Arch Surg 1995;130:817- 23.
24. Vege SS, Baron TH: Management of pancreatic necrosis in severe acute pancreatitis. Clin Gastroenterol Hepatol 2005;3:192-95.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





