IJCRR - 9(6), March, 2017
Pages: 30-33
Date of Publication: 31-Mar-2017
Print Article
Download XML Download PDF
Correlation between Serum Ferritin and Glycated Hemoglobin Level in Patients of Type 2 Diabetes Mellitus
Author: Poonam Arora
Category: Healthcare
Abstract:Introduction: The complications of diabetes mellitus are influenced not only by the duration of the diabetes mellitus but also by the average level of blood glucose along with glycated haemoglobin. Raised serum ferritin may possibly be related to the occurrence of long term complications of diabetes, both microvascular and macrovascular.
Objective: The aim of this study is to establish a correlation between serum ferritin, fasting plasma glucose and glycated hemoglobinin type 2 diabetes mellitus patients.
Materials and Methods: This was a cross-sectional study of 100 cases, visiting medical outpatient department of SGT Medical College and Hospital, Budhera, Gurugram, Haryana. Sample were analysed for the measurement of FPG, HbA1c and Serum Ferritin (by ELISA).
Results: The mean FPG, HbA1c and serum ferritin levels were significantly higher with P< 0.01 in diabetic group compared to controls. Serum ferritin was significantly related to the duration of diabetes (P< 0.05). As the duration of diabetes increased, serum ferritin levels were also increased. Also there was a positive correlation between serum ferritin and FPG, HbA1c. Serum ferritin is significantly related to FPG (r-0.903, P< 0.01) in diabetic patients. Serum ferritin is also positively related to HbA1c (r-203, P< 0.05).
Conclusion: Findings of this study concludes that serum ferritin is elevated in patients with type 2 diabetes mellitus when compared to healthy individuals and it indicates that serum ferritin can be used as a marker for glycemic control in diabetic patients. .
Keywords: Serum Ferritin, Glycated Hemoglobin, Type 2 Diabetes Mellitus
Full Text:
Introduction:
Diabetes is a metabolic disorder characterized by hyperglycemia from defects in insulin secretion, insulin action, or both1. People with type 2 diabetes mellitus develop characteristic microvascular complications such as retinopathy, nephropathy and neuropathy. There is also increased risk of macrovascular complications such as cardiovascular, cerebrovascular and peripheral vascular disease2.
Complications due to diabetes are a major cause of disability, reduced quality of life and death. Approximately 5.1 million people aged between 20 and 79 years died from diabetes accounting for 8.4% of global all cause mortality in this age group3. In India 65.1 million in the age group of 20 to 79 have diabetes (8.56%) and expected to rise to 109 million by the year 20354.
The pathogenesis of type 2 diabetes mellitus (T2DM) is complex and involves the interaction of genetic and environmental factors. Individuals with (T2DM) show both insulin resistance and beta cell defects5. The complications of diabetes mellitus are influenced not only by the duration of the diabetes mellitus but also by the average level of blood glucose along with glycated haemoglobin2.
Serum ferritin is an acute phase reactant, and is a marker of iron stores in the body6. Iron is a transitional metal that can easily become oxidized and thus act as an oxidant7. Elevated iron stores may induce diabetes through a variety of mechanisms, including oxidative damage to pancreatic beta cells, impairment of hepatic insulin extraction by liver, and interference with insulin’s ability to suppress hepatic glucose production 8.
Raised serum ferritin may possibly be related to the occurrence of long term complications of diabetes, both microvascular and macrovascular 9,10.
Recent studies have shown that serum ferritin was proportional to serum glucose concentration, diastolic blood pressure, HDL cholesterol, and insulin resistance. In fact, the higher the ferritin levels, the higher the incidence of type 2 diabetes mellitus11,12. Amongst the various markers of glycemic control, glycated hemoglobin has now been established as the most reliable. However, ferritin’s role as a marker of iron overload in pancreatic damage and peripheral insulin resistance or its role as an inflammatory marker is not clear13.
Hence this study was carried out to examine the association between serum ferritin and glycated hemoglobin levels in T2DM and to establish a correlation between serum ferritin, Fasting Plasma Glucose (FPG) and Glycated Hemoglobin (HbA1c).
Materials and Methods:
This was a cross-sectional study of 100 cases, visiting medical outpatient department of SGT Medical College and Hospital, Budhera, Gurugram, Haryana. The study was approved by institutional ethical committee. 50 diabetic patients were compared with 50 age and sex matched normal healthy controls. A written informed consent was also taken from the cases with detailed history.
Inclusion Criteria: Clinically diagnosed type 2 diabetes mellitus patients on treatment in the age group of 35-70 years.
Controls: Healthy controls in the age group of 35-70 years.
Exclusion Criteria:
Chronic Infections
Chronic Liver Disease
Chronic Renal Disease
Overt Thyroid Dysfunction
Patients on Corticosteroids Therapy
Anemia (Hb<10 gm/dL)
5 mL of fasting blood sample was collected and centrifuged for serum/plasma separation. Sample were analysed for the measurement of plasma glucose by glucose oxidase-peroxidase method, whole blood taken in EDTA vial for HbA1c by ion-exchange resin method and serum ferritin was assessed by ELISA method by commercially available kit provided by Calbiotech.
Statistical Analysis:
Statistical analysis was done using the SPSS software version 24. The data was represented by counts, percentage and mean± standard deviation. Statistical analysis of the biochemical parameters, FPG, HbA1c and serum ferritin were done by t-test to compare these parameters in cases and controls. Pearson’s correlation coefficient was used for comparison of variables. A P –value of <0.05 was considered significant and P-value >0.05 as non-significant.
Results:
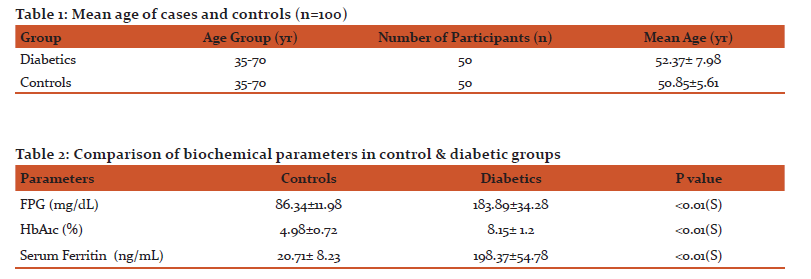
In this study majority of patients were male (68% vs 32%). The mean age of diabetic patients was 52.37± 7.98 years and that of the controls was 50.85±5.61 years. (Table 1) There was no statistical significant difference of age between the two groups in either gender.
The age of onset of diabetes in 80% of cases was between 40 and 50 years. In majority of patients (64%) the duration of diabetes was between 5-10 years and more than 10 years in 36%. 76% patients were on oral hypoglycaemic drugs and 24% were on insulin therapy.
The mean FPG, HbA1c and serum ferritin levels were significantly higher with P<0.01 in diabetic group compared to controls (Table 2). Serum ferritin was significantly related to the duration of diabetes (P<0.05). As the duration of diabetes increased, serum ferritin levels were also increased.
Also there was a positive correlation between serum ferritin and FPG, HbA1c. Serum ferritin is significantly related to FPG (r-0.903, P< 0.01) in diabetic patients. Serum ferritin is also positively related to HbA1c (r-203, P<0.05)
Discussion:
Type 2 diabetes mellitus is a chronic metabolic disorder and its prevalence has been increasing steadily all over the world. People living with type 2 diabetes mellitus are more vulnerable to short and long term complications, which often lead to their premature death14.
Oxidative stress has been implicated in the pathogenesis of the complications seen in T2DM15. Superoxide and hydrogen peroxide appear to be the primary generated species. These species may then play a role in the generation of additional and more reactive oxidants, including the highly reactive hydroxyl radical in which iron salts play a catalytic role in a reaction. This reaction is commonly referred to as the metal catalyzed Haber-Weiss reaction 16.
 Fe3+ + O2 Fe2+ + O2
Fe3+ + O2 Fe2+ + O2
 Fe2+ + H2O2 Fe3+OH + OH-
Fe2+ + H2O2 Fe3+OH + OH-
 O2- + H2O2 OH. + OH-
O2- + H2O2 OH. + OH-
Iron is the most abundant trace element in the body, and almost all iron occurs bound to proteins. Iron is a double-edged sword. In moderate quantities and leashed to proteins, it is an essential element in all cell metabolism and growth, but it is toxic when unleashed17.
Because of its ability to switch back and forth between ferrous and ferric oxidation states, iron is both a strong biological oxidant and reductant. Although the exact mechanism of iron-induced diabetes uncertain, it is likely, to be mediated by three key mechanisms: Insulin deficiency, insulin resistance and hepatic dysfunction18.
The central importance of iron in the pathophysiology of disease is derived from the ease with which iron is reversibly oxidized and reduced. This property, while essential for its metabolic functions, makes iron potentially hazardous because of its ability to participate in the generation of powerful oxidant species such as hydroxyl radical16.
Another endogenous source of catalytic free iron is the iron released when the heme ring is opened by hemeoxygenase7. The intracellular generation of apoferritin is a cytoprotective antioxidant stratagem of endothelial cells 19, 20, since serum ferritin is increased in T2DM.
Ferritin is considered a positive acute phase protein and is up regulated intracellularly in many cell types, and extracellularly, in the plasma as a result of an increase in cellular secretion. An important role of ferritin during the acute phase response is to restrict the availability of iron by sequestration into the cavity of the ferritin protein shell 14.
The role of iron in the pathogenesis of diabetes is suggested by an increased incidence of type 2 diabetes in diverse causes of iron overload and reversal or improvement in diabetes (glycemic control) with a reduction in iron load achieved using either phelobotomy or iron chelation therapy 18. The importance of protein glycation is well known in the pathogenesis of diabetic vascular complications. Transition metals also play a role in protein glycation induced by hyperglycemia. It has been shown that glycated proteins have a substantial affinity for the transition metals, and the bound metal retains redox activity and participates in catalytic oxidation. Thus, should similar glycochelates form in vivo, reactions mediated by the chelates could be involved in the vascular complications of diabetes 21.
Different theories regarding the role of ferritin in T2DM have been suggested. Ferritin has been referred as a marker for insulin resistance possibly due to iron deposition in the liver leading to hepatic insulin resistance and increased hepatic glucose production11,22. Others has determined that ferritin just as a marker of pancreatic inflammation, while pancreatic damage due to some degree of subclinical hemochromatosis has been considered in some cases of diabetes 13.
Two large epidemiological studies reported a strong association between elevated serum ferritin concentration and increased risk for diabetes 23, 24. In present study a statistical significant increase in fasting plasma glucose, glycated hemoglobin and serum ferritin levels were observed in patients of T2DM as compared to healthy controls. This finding is supported by various studies 14, 25, 26, 27, 28, 29. A prospective case control study conducted by Thilip Kumar G et al reported that patients with T2DM had significantly higher serum ferritin level when compared to healthy controls but there is no correlation between serum ferritin with mean blood glucose and HbA1c 2. A study by Jose- Manuel Fernandez 22 reported a correlation between serum ferritin with basal plasma glucose and no correlation with HbA1c in diabetics and normal controls. So there is a need for further studies to confirm the implications of serum ferritin as a marker for type 2 diabetes mellitus and its role in pathogenesis of T2DM.
Conclusion:
Based on this study it is concluded that serum ferritin is elevated in patients with type 2 diabetes mellitus when compared to healthy individuals and it indicates that serum ferritin can be used as a marker for glycemic control in diabetic patients.
Acknowledgement:
Author acknowledges the immense help received from the scholars whose articles are cited and included in references of this manuscript. The author is also grateful to authors/editors/ publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
- Valdez R, Liu T, Yoon PW, Khoury MJ. Family history and prevalence of diabetes in the U.S. population. Diabetes Care 2007; 30: 2517-22.
- Thilip Kumar G, Saravanan A, Ramachandran C and John Nitin Ashok. Mean blood glucose level and glycated haemoglobin level in patients of non-insulin dependent diabetes mellitus and its correlation with serum ferritin level. Int J Med Sci 2011; 4 (1and 2): 13-17.
- Roglic G, Unwin N. Mortality attributable to diabetes: estimates for the year 2010. Diabetes Res Clin Pract 2010; 87(1): 15-19.
- IDF Diabetes Atlas, 2013; 6th edn. Chapter-2.1;34.
- National Diabetes Data Group. Classification and diagnosis of diabetes mellitus and other categories of glucose intolerance. Diabetes 1979; 28: 1039-57.
- Koorts AM, Viljoen M. Acute phase proteins: Ferritin and ferritin isoforms. University of Petoria, South Africa 2011; 154-84.
- Herbert V, Spencer S, Jayatilleke E, Kasadan T. Most free radical injury is iron-related: Itis promoted by iron, heme, holoferritin and vitamin C and inhibited by desferoxamine and apoferritin. Stem Cells 1994; 12: 289-303.
- Gallou G, Guilhem I, Poirier JY, Ruelland A, Legras B, Cloarec L. Increased serum ferritin in insulin-dependent diabetes mellitus: relation to glycemic control. Clin Chem 1994; 40: 947-8.
- Kim NH. Serum ferritin in healthy subjects and type 2 diabetes mellitus. Med Korea 2000; 41: 387-92.
- Eshed I, Elis A, Lishner M. Plasma ferritin and type 2 diabetes mellitus. Endocr Res 2001; 27: 91-7.
- Forouhi NG, Harding AH, Allison M, Sandhu MS, Welch A, Luben Re et al. Elevated serum ferritin levels predict new-onset type 2 diabetes: results from the EPIC-Norfolk prospective study. Diabetologia 2007; 50: 949-56.
- Wrede CE, Buettner R, Bollheimer LC, Scho lmeirch J, PalitzschK-D and Hellerbrand C. Association between serum ferritin and the insulin resistance syndrome in a representative population. Eur J Endocr 2006; 154: 333-40.
- Sharifi F and Sazandeh Sh. Serum ferritin in type2 diabetes mellitus and its relationship with HbA1c. Acta Med Iranica 2004; 42(2): 142-45.
- Padmaja P, Shabana S and Shariq Mas. Serum ferritin and HbA1c in type 2 diabetes mellitus. Int J Clin and Biomed Res 2015; 1(3): 30-37.
- Radoi V, Lixandru D, Mohara M, Virgolici B. Advanced glycation end products in diabetes mellitus: Mechanism of action and focused treatment. Proc Rom Acad Series B 2012; 1: 9-19.
- Halliwell B, Gutteridge JMC. Role of free radicals and catalytic metal ions in human disease: an overview. Meth Enzymol 1990; 186: 1-85.
- Herbert V. Everyone should be tested for iron disorders. J Am Diet Assoc 1992; 92: 1509-76.
- Swaminathan S, Fonseca VA, Alam MG, Shah SV. The role of iron in diabetes and its complications. Diabetes Care 2007; 30 (7): 1926-33.
- Balla J, Jacob HS, Balla G, Nath K, Vercellotti GM. Endothelial cell hemeoxygenase and ferritin induction by heme proteins: a possible mechanism limiting shock damage. Trans Assoc Am Phys 1993; 105: (in press).
- Balla G, Jacob HS, Balla J, Rosenberg M, Apple F, Eaton JW, Vercellotti GM. Ferritin: a cytoprotective antioxidant stratagem of endothelium. J Biol Chem 1992; 267: 18148-53.
- Qian M, Liu M, Eaton JW. Transition metals bind to glycated proteins forming redox active “glycochelates”: implications for the pathogenesis of certain diabetic complications. Biochem Biophys Res Comm 1998; 250: 385-89.
- Fernandez-Real JM, Richard- Engel W, Arroyo E, Balanca R, Casamitjana-Abella R. Serum ferritin as a component of the insulin resistance syndrome. Diabetes Care 1998; 21(1): 62-68.
- Ford ES, Cogswell ME. Diabetes and serum ferritin concentration among U.S. adults. Diabetes Care 1999; 22: 1978-83.
- Tuomainen TP, Nyyssonen K, Salonen R, Tervahuta A, Korpela H, Lakka T et al. Body iron stores are associated with serum insulin and blood glucose concentration: Population study in 1,013 eastern Finnish Men. Diabetes Care 1997; 20(3): 426-28.
- Thanna RC, Nigosker S. Level of serum ferritin and glycated haemoglobin in type 2 diabetes mellitus. Int J Med and Health Sci 2016; 2(2): 49-51.
- Momeni A, Behradmanesh MS, Khieri S, Abasi F. Serum ferritin has correlation with HbA1c in type 2 diabetic patients. Adv Biomed Res 2015; 4: 74.
- Rawat N, Mathur N, Harikrishnan R, Choudhary J, Rawat K, Mathur M. A study of correlation of serum ferritin with glycated haemoglobin in diabetes mellitus type 2 patients: a case control study. Asian Pac J Health Sci 2016; 3(4): 83-88.
- Pramiladevi R, Boke U, Kora S. Serum ferritin levels in type II diabetes mellitus. Sch J App Med Sci 2013; 1(5): 472-75.
- Raj S, Rajan GV. Correlation between elevated serum ferritin and HbA1c in type 2 diabetes mellitus. Int J Res Med Sci 2013; 1(1): 12-15.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





