IJCRR - 4(22), November, 2012
Pages: 105-108
Date of Publication: 24-Nov-2012
Print Article
Download XML Download PDF
THE ACCESSORY NAVICULAR BONE - A RADIOLOGICAL FINDING AND DISCUSSION OF ITS CLINICAL PRESENTATION
Author: S.D. Desai, Sahana B. N., Monish Bami
Category: Healthcare
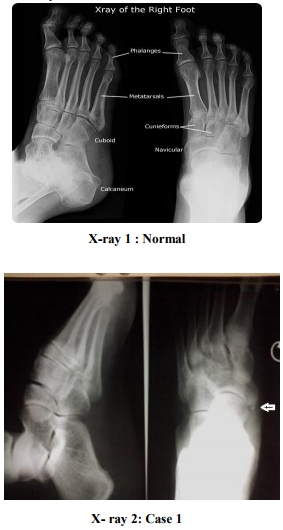
Abstract:Introduction- The accessory navicular is located on the posteromedial aspect of the foot, in close proximity with the navicular bone. This radiographic variant has been described in the anatomic and orthopaedic literatures with a variation of names such as ostibiale externum, osnaviculare secundarium, osnaviculare accessorium, osscaphoidea accessoria and pre-hallux. We report here two cases to better the understanding of this condition. Case Report- Two X-rays with asymptomatic accessory navicular bones were obtained from the department of orthopaedics. Case 1: A 43 year old male patient came to orthopaedic OPD with fracture of lower one third of left tibia, both leg and foot was radiographed for the same. Case 2: A 27 year old female patient came with left ankle sprain for which X- ray of foot along with ankle joint was taken. Conclusion- Though asymptomatic, they were at risk of developing symptoms related to accessory navicular later in life. Therefore the findings are to be considered by radiologists, orthopaedicians and physicians before treating a patient with complaints of pain at ankle joint or foot and a high degree of clinical suspicion must be kept in mind in patients with persistant pain.
Keywords: Accessory navicular, ostibiale externum, prehallux, X ray.
Full Text:
INTRODUCTION
The navicular bone is uniquely situated in the midfoot. The accessory navicular was first described by Bauhin in 1605. This radiographic variant has been described in the anatomic and orthopaedic literature1 . 10% to 14 % of normal feet have an accessory navicular bone, which may exist unilaterally or bilaterally2 . Bilateral location occurs in 50–90% of cases and there is a higher prevalence in females3 . It is located on the posteromedial aspect of the foot, in close proximity with the navicular bone4 . Accessory bones of the foot are anomalies that develop during ossification5 . It arises from a separate ossification centre in the navicular tuberosity region6 . In most cases, these bones are inconsequential; however, when they are associated with trauma they can result in acute or chronic foot pain. To appropriately diagnose and treat foot problems, it is essential to know the location of accessory bones. The accessory navicular bone has been classified by various authors into three primary types. Type I also referred to as "ostibialeexternum" occurs mainly as a round sesmoid within the substances of the distal posterior tibial tendon. It is rarely associated with symptoms. Type II also referred to as "prehallux” is associated with a synchondrosis within the body of the navicular at risk for disruption either from traction injury or shear forces in this region. Type III also known as a “navicular beak” or a “cornuatenavicular”, occurs with the fusion of accessory navicular bone to the body of the navicular4, 7 .
CASE REPORT
We report two cases of unilateral accessory navicular bone found accidently during X- ray imaging of foot. Case 1: A 43 year old male patient came to orthopaedic OPD with fracture of lower one third of left tibia, both leg and foot was radiographed for the same. Case 2: A 27year old female patient came with left ankle sprain for which X- ray of foot along with ankle joint was taken. In both these cases accessory navicular were found but was asymptomatic, when right foot X- ray was taken there was no evidence of accessory navicular in both the cases.

DISCUSSION
Clinical presentations: Typical young female (10- 20 years of age) complaining of mid foot/arch pain which may be insidious or post trauma. Difficulty with footwear’s, prominentnavicular, tenderness over the prominence, pesplanus, painful navicular syndrome and posterior tibialis tendinopathy (PTT). The type II accessory navicular is the most commonly symptomatic variant with localized chronic or acute on chronic medial foot pain and tenderness with associated inflammation of overlying soft tissue8 . In the setting of chronic medial foot pain, especially occurring after stress or physical exercise accessory navicular bone should be suspected. PTT: The presence of either an accessory navicular type 2 or type 3 (cornuatenavicular) is a risk factor for PTT, since the accessory navicular acts as it were a native navicular with the bulk of the posterior tibialis tendon inserting onto the accessory navicular9 . Diagnosis of this condition relies on radiographic evaluation. Routine standing anteroposterior and lateral view are enough to look for accessory navicular but in some cases the 45-degree eversion oblique view of the foot is useful in identifying this condition, although several different imaging techniques can be used. Treatment of this condition includes both surgical and nonsurgical options. Ultimately, surgery yields the best outcome for young patients, though conservative management has relevance for less active patients8 . Asymptomatic accessory navicular is non-operative. If the symptoms persist and ultrasonography demonstrates changes in the synchondrosis, operative intervention may be performed. There are 2 surgeries that can be performed depending upon the condition and symptoms. First is simple surgical excision. Second is Kindler procedure, in this the ossicle and navicular prominence is excised as in simple excision but along with the posterior tibial tendon advancement. Posterior tibial tendon is split and advanced along the medial side of foot to provide support to longitudinal arch4 . In the present cases no active treatment was given as they were asymptomatic. They were treated for their presenting conditions and were advised for follow up in case of symptoms related to accessory navicular bone. In a study done by Evangelos Perdikakis & EleniGrigoraki & Apostolos Karantanas Accessory navicular bone was identified in 34 cases (20%) of the 170 exams. It was detected in 14 male and 14 female patients with the following incidence: 11.15% type I (19cases), 4.11% type II (7 cases) and 4.74% type III (8 cases)1 . FarhanAli, James A. Fernandes reported a case of osteomyelitis of an accessory navicular bone in a young girl aged 11-years to make treating clinicians aware of this rare possibility2 . Chen et al. described degeneration of the accessory navicular synchondrosis in adults and its confusion with tendinitis of the posterior tibial tendon with distruption10 .
CONCLUSION
In conclusion, we should look for an accessory navicular bone on radiography in patients with flatfoot or PTT abnormalities. Conversely, patients with an accessory navicular bone type 2 or 3 and medial foot pain or flatfoot should be examined by MRI for insertion abnormalities of the PTT or painful accessory navicular. The findings are to be considered by radiologists, orthopaedicians and physicians before treating a patient with complaints of pain at ankle joint or foot. Clinicians should also be aware that these accessory bones are possible sources of foot pain that may lead to disability.
Limitations
Plain radiographic identification of the accessory navicular is insufficient to attribute symptomatology. Instead ultrasound can be done which allows for comparison with the asymptomatic side and localization of pain. Bone scintigraphy is another option that has high sensitivity but positive findings lack specificity. Magnetic resonance imaging is of high diagnostic value for demonstrating accessory navicular along with both bone marrow and soft tissue oedema.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors/editors/publishers of all those articles journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Perdikakis E, Grigoraki E, Karantanas A. Osnaviculare: the multi-ossicle configuration of a normal variant. Skeletal Radiol 2011; 40:85–8.
2. Ali F, Fernandes J A. Osteomyelitis of the accessory navicular bone in the foot- A case report. ActaOrthop. Belg 2004;70:287-9.
3. Lawson J P, Ogden J A, Sella E, Barwick K W. The painful accessory navicular. Skeletal Radiol 1984;12:250–62.
4. Canale S T. Pesplanus. In: Canale S T, editor. Campbell’s operative orthopaedics, vol 4, 10th ed. United States of America; Mosby; 2005:4027-8.
5. Requejo S M, Kulig K,Thordarson D B. Management of foot pain associated with accessory bones of the foot: two clinical case reports. J Orthop Sports Phys 2000;30(10):580-91.
6. Standring S. Foot and ankle.In: Standring S, editor. Gray's Anatomy, 39th ed. Churchill Livingston: Elsevier; 2005.p.1515.
7. Choi Y S, MD, Lee K T, Kang H S, Kim E K. MR imaging findings of painful typeII accessory navicular bone: correlation with surgical and pathologic studies. Korean J Radiol 2004;5(4):274–9.
8. Fredrick LA, Beall DP, Ly JQ, Fish JR. The symptomatic accessory navicular bone: a report and discussion of the clinical presentation.Current Problems in Diagnostic Radiology 2005;34(2):47-50.
9. Bernaerts A, Vanhoenacker F M, Van De Perre S, De Schepper A M, Parizel P M. Accessory navicular bone: not such a normal variant. JBR–BTR 2004;87(5):250-2.
10. Chen Y J,Hsu R W, Liang S C. Degeneration of the accessory navicularsynchondrosis presenting as rupture of the posterior tibial tendon. J Bone Joint Surg Am 1997;79(12):1791-8.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





