IJCRR - 4(22), November, 2012
Pages: 91-98
Date of Publication: 24-Nov-2012
Print Article
Download XML Download PDF
A STUDY ON THE EFFICACY OF PATELLAR TAPING FOR KNEE OSTEOARTHRITIS AS COMPARED TO CONVENTIONAL PHYSICAL THERAPY
Author: Arnab Chandra, K. S. Sharad, Anwer Shahnawaz, Siddhartha Shankar Sikdar
Category: Healthcare
Abstract:Background: Taping has been successfully used by physiotherapists in management of sports injuries. It has been proposed that it can be used to treat degenerative joint disease like osteoarthritis however there is a lack of evidence. Purpose: To compare the effectiveness of taping technique along with conventional physical therapy versus conventional physical therapy alone in patients with patellofemoral joint osteoarthritis. Methods: Thirty subjects with mean (SD) age of 55\?6 years were randomized into 2 groups. Subjects in group A were treated with McConnell taping technique along with ultrasound therapy and supervised exercise protocol while subjects in group B were treated with ultrasound therapy and supervised exercise protocol. The outcome measures were Visual Analogue Scale (VAS); Western Ontario McMaster Universities index (WOMAC), Timed Up and Go test (TUG) and Timed Stair Ambulation Test (TSAT) which were assessed prior and after 2 weeks of intervention. Results: Both the groups showed significant improvement in pain scores. Between groups comparison found that group A displayed statistically significant improvement in terms of pain intensity, WOMAC score, TUG and TSAT. Conclusion: Patients in taping group had greater gains in attaining functional abilities and pain relief compared to conventional group, though there was no significant difference in improvement in timed stair ambulation test between the two groups. Therefore, application of taping can be considered beneficial for pain relief and functional ability improvement in subjects with patellofemoral joint osteoarthritis.
Keywords: Patellofemoral osteoarthritis, McConnell taping, WOMAC.
Full Text:
INTRODUCTION
Osteoarthritis (OA) of knee is a common disease affecting thousands of Indian citizens1 . It is a prevalent musculoskeletal condition in older age group, causing pain, physical disability, and decreased quality of life2 . It also imposes a considerable economic burden on the health care system3 .The patellofemoral joint (PFJ) is one compartment of the knee that is usually affected by OA and is a source of symptoms. Within the PFJ, the lateral compartment is more frequently affected by the OA process than the medial4 . There is no specific treatment to alter the disease; current treatment is focused in reducing symptoms and enhancing function5 . Analgesic and anti-inflammatory drugs are used widely, in spite of potential side effects and uncertainties about their efficacy6 . Simple, inexpensive treatment is required for common disorders such as knee OA, which is not life threatening but can cause pain and disable a large number of people in the community. Physical therapy management includes various treatment modalities like Short wave diathermy, Ultrasound therapy, and other heating modalities along with Exercise therapy, with variable outcomes. Exercise is recognized as an essential component of the long-term management of OA. The aim of exercise is to reduce pain and disability by strengthening muscles, improving joint stability, aerobic fitness, and proprioception and increasing range of motion7 . Since early days, tape has been used to support joints and prevent injury in athletes. Nowadays, knee tape is used by physiotherapists to treat knee pain. Many studies have shown that patellar taping decrease pain in patient with Patellofemoral pain syndrome (PFPS) and in patellofemoral osteoarthritis8 , although the mechanism for this improvement remains unknown. Taping is proposed to achieve its effect by both mechanical and functional mechanisms. Mechanically, the ROM at the joint is reduced by taping and the force required to displace the joint is increased9, 10. Functionally, taping can cause reflex stimulation of skin, encourage learning process due to skin drag, enhance proprioception and alter underlying muscle contraction. Knee taping is believed to relieve pain by improving alignment of the patellofemoral joint and/or unloading inflamed soft tissues11. More recently, there has been speculation that there may be a more suitable role of patellar taping in providing sensory feedback and influencing the proprioceptive status and neuromuscular control of the patellofemoral joint12 . Therefore, this study is designed to compare the efficacy of therapeutic taping adjunct to conventional physical therapy for the treatment of chronic patellofemoral joint osteoarthritis.
METHODS
Subjects
Thirty subjects were selected from the cases referred by the outpatient department (OPD) of National Institute for the Orthopaedically Handicapped (NIOH) and were randomly allocated into two groups. The inclusion criteria were: All referred and pre diagnosed case of knee osteoarthritis involving patellofemoral joint, anterior- or retro-patellar knee pain aggravated by at least two activities that load the PFJ (e.g. stair ambulation, squatting and/or rising from sitting), pain during these activities present on most days during the past month, pain severity >4 in VAS scale. Subjects were excluded if they had concomitant pain from other knee structures, hip or lumbar spine, history of tape allergy, recent knee injections (prior 3 months), history of any knee or hip surgery and moderate to severe concomitant tibiofemoral joint osteoarthritis. This study was approved by the Institutional Ethical Committee (IEC) of NIOH and written consent was taken from every subject. The nature and purpose of the study and its potential risks / benefits and expected duration of the study, and other relevant details of the study were explained to every subject in their own language. Participation of subjects in study was voluntary and that subjects were free to withdraw at any time, without giving any reason, without his/her medical care or legal right being affected.
Procedure
Subjects in group A received conventional physical therapy in the form of ultrasound therapy and supervised exercise protocol along with taping based on McConnell procedure. Subjects received continuous ultrasound therapy for 6 sessions (alternate day for 2 weeks) with the intensity set at 1.5 watt/cm2 for 8 minutes with 1 MHZ frequency. The subjects exercised for 6 sessions. The duration of each session was 20 minutes. The exercise performed were as follows:13 walking for 1 minute at normal pace, active knee range of motion (with in the limit of pain) for 2 minutes, free active movement of the hip and ankle joint for 2 minutes, flexibility exercises in which the following muscles (group) were stretched14 (Hamstring, Quadriceps, Hip adductor, Hip flexors, Gastronomies and Hip extensors). They did strengthening exercises which were progressed from non weight bearing to weight bearing.15 Non weight bearing exercises included: Isometric quadriceps, straight leg rising exercise, hamstring setting exercise, short arc terminal extension exercise and strengthening of vastus medialis. Mini squats were done as weight bearing exercises.
Taping procedure
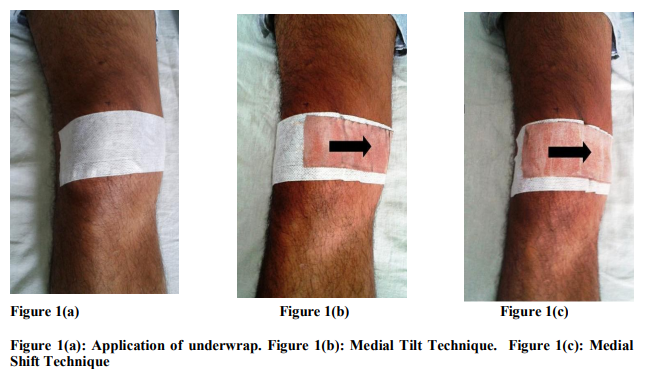
Subjects laid supine with their knees extended and the quadriceps relaxed. Skin was shaved prior to tape application. Two tape were taken; one is adhesive tape of 2 inch width (adhesive, nonelastic, made by physiomed company) and another is leucopore (made of cotton by Johnson and Johnson company) for under wrap. At first, the under wrap was applied by leucopore anteriorly from lateral femoral condyle to just posterior to medial femoral condyle as in figure 1(a) to cover the patella completely. Over the under wrap, rigid adhesive tape was applied on the patella in the direction of medial glide and medial tilt. Medial glide technique: One end of the tape was secured to the lateral patellar border and the patella was glided medially by the use of the thumb while maintaining tension of the tape. It was applied up to medial border of medial hamstring tendon as in figure 1(b). Medial tilt technique: The tape was secured at the middle portion of patella and then pulled medially to tilt the lateral border of patella; correcting the tilt and it was applied up to the medial border of medial hamstring tendon as in figure 1(c). In both cases the medial soft tissues were brought over the medial femoral condyle toward patella to obtain a more secure fixation. The tape was applied on each subject for 6 sessions (alternate day for 2 weeks). Subjects were instructed to maintain the tape for at least 24 hours which was then removed by subject him/herself. Subjects were asked to check the skin for damage and apply antibiotic lotion to restore skin moisture. Same treatment protocol was given in group B except taping technique.
Outcome Measures
Baseline and post intervention data (after 2 weeks) were taken by using VAS scale16 , WOMAC Index of Osteoarthritis17, Timed stair ambulation test18 and Time up and go test19 . WOMAC Index is used to assess patients with osteoarthritis of the knee in terms of pain, stiffness, and physical function using 24 parameters where for knee possible pain score ranges from 0-20, for stiffness range 0-8 and for function 0-68. The pain, stiffness, and physical function was assed using 5 point ordinal scale (0- much improved, 1-improved, 2-no change, 3- worse, 4-much worse). Maximum total score is 96, and minimum is 0. So, higher WOMAC scores indicate poorer outcome. The timed stair ambulation test involves the participant ascending and descending a set of nine standard steps at their usual pace and the total time taken is recorded. Longer the time taken; poorer is the physical function. Time up and go test is a valid and reliable test of function in older individuals. Participants were instructed to rise from a standard arm chair, walk around a cone on the floor 3 meters away, return to the chair and sit down again, whilst being timed by a stop watch. Participants performed the test bare foot, once only and at their own pace.
STATISTICAL ANALYSIS
Analysis of data was done using SPSS 17.0 Software (SPSS Inc., Chicago, USA). The observed values measured by VAS, TSAT and TUG were tested by the fisher’s t test (independent t- test) to test for differences between the groups. Mann Whitney U test was used to analyze WOMAC scale scores in between groups. A statistically significant difference was defined as p≤ 0.05 at 95% confidence interval.
RESULTS
The study population belongs to middle age group with mean age 55 (SD ±6) years and male: female ratio - 1:1.6. The mean and SD for between groups comparison of all 4 parameters are represented in figures 2 to 5. When comparing between groups, all outcome measures showed significant improvement (p≤0.05) in group A as shown in table 1 and 2.
DISCUSSION
The result of present study shown that taping group had beneficial effect as compare to ultrasound therapy and supervised exercise alone. Study done by Hinman et al evaluated the effects of knee tape in a population with osteoarthritis, and 25? reduction in pain was observed in patient with patellofemoral joint disease by taping the patella medially for four days20. Few of the authors suggested that this effect is not produced by medialization of patella. Bockrath et al21 also argued that patellar tape may elicit neural inhibition by facilitating large afferent fiber input. Herrington22 proposed that patellar taping may lead to altered large fiber afferent input to the dorsal horn, decreasing the perceived pain that may be contributing to quadriceps inhibition. He also suggested that there is potential for restoration of quadriceps function through increased alpha motor neuron excitation. Additionally, cutaneous stimulation from the patellar tape may change the order and timing of motor unit recruitment23. Changes in Electromyographic (EMG) activity of the Vastus medialis obliquus (VMO) relative to Vastus lateralis (VL) after the application of patellar tape has been reported in several studies24 . The present study demonstrated that the application of ultrasound therapy with supervised exercise protocol had shown significant changes in pain as well as physical function within the group. In the present study WOMAC index was used to assess overall knee function since its validity and reliability is already established25 . There was also significant difference in WOMAC index in all the subjects after the 2 weeks therapeutic interventions of taping, ultrasound therapy, and supervised exercises. However, it was noted that WOMAC index was highly reduced in the subjects treated by taping. In the present study, group A had shown significant changes in pain and functional activities than group B which indicated that combination of patellar taping, ultrasound therapy and supervised exercise protocol was helpful in reducing pain and improving physical functional status of subjects with knee osteoarthritis. So this treatment could be used as an effective conservative management for pain relief and improving physical function. Further clinical research is needed in this field before using only the above treatment as a standard therapy, and as the best treatment approach requires a long term therapy for osteoarthritis knee.
CONCLUSION
The present randomized clinical trial provided evidence to support the use of physical therapy regimen in the form of ultrasound therapy, supervised exercise protocol and patellar taping in relieving pain and improving physical function in subjects with chronic osteoarthritis of knee joint. In addition, results supported that combination therapy is of great value which can be useful in improving quality of life as knee osteoarthritis is a heterogeneous condition.
ACKNOWLEDGEMENTS
We wish to thank all the staffs of Indoor Physiotherapy department of NIOH, Kolkata for their guidance throughout the study. We also thank Dr. Ratnesh Kumar, Director, NIOH for allowing us to conduct our study. Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Manjusha Vagal. Medial taping of patella with dynamic thermotherapy — A combined treatment approach for osteoarthritis of knee joint. The Indian Journal of Occupational Therapy 2004;36(2):32 – 36.
2. Felson DT, Naimark A, Anderson J, Kazis L, Castelli W, Meenan RF. The prevalence of knee osteoarthritis in the elderly. The Framingham Osteoarthritis Study. Arthritis Rheum 1987;30:914–18.
3. The Arthritis Foundation of Australia. The prevalence, cost and disease burden of arthritis in Australia. Canberra: Access Economics Pty Limited, Canberra ACT, 2001.
4. Iwano T, Kurosawa H, Tokuyama H, Hoshikawa Y. Roentographic and clinical findings of patellofemoral arthritis. Clinical Orthopaedicsand Related Research 1990; 252:190-7.
5. Dieppe PA. Management of osteoarthritis of the hip and knee joints. Current Opinion in Rheumatology 1993;5:487-93.
6. Dieppe PA, Frankel SJ, Toth B. Is research into the treatment of osteoarthritis with nonsteroidal anti-inflammatory drugs misdirected? Lancet1992;341:353–4.
7. Rebecca Grainger, Flavia M Cicuttini. Medical management of osteoarthritis of the knee and hip joints, MJA 2004;180(5):232- 236 8. Cushnaghan J, McCarthy C, Diappe. Taping the patella medially: a new treatment for osteoarthritis of the knee. British Medical Journal 1995;308:753-755.
9. Vaes P H, Duquet W, Casteleyn P, Handelberg F, Opdecam P. Static and dynamic roentgenographic analysis of ankle stability in braced and nonbraced stable and functionally unstable ankles. Am J Sports Med 1998;26:692–702.
10. Larsen, E. Taping the ankle for chronic instability. Acta Orthopaedica Scandinavica 1984;55(3):551–53.
11. Hunter DJ, March L, Sambrook PN. The association of cartilage volume with knee pain. Osteoarthritis and Cartilage 2003;11:725-9.
12. Mokhtarinia H, Ebrahimi-Takamjani I, Salavati M, Goharpay S, Khosravi A .The effect of patellar taping on knee joint proprioception in patient with patellofemoral pain syndrome. Acta Medica Iranica 2008;46(3):183-190
13. Carolyn Kishner, Lynn Allen Colby. The Knee. Therapeutic exercise foundations and technique, 5th edition. Philadelphia, Davis Plus 2007. p. 687 – 757.
14. Laprade J, Culham E, Brouwer B. Comparison of five isometric exercises in the recruitment of the vastusmedialis oblique in persons with and without patellofemoral pain syndrome. JOSPT 1998;27:197-204.
15. Doucette, SA and Goble, EM. The effect of exercise on patellar tracking in lateral patellar compression syndrome. Am J Sports Med 1992;20:434.
16. Huskisson EC. Visual analogue scales. In [Melzark R] (ed.) Pain measurement and assessment. New York: Raven 1983;33-7.
17. Bellamy N, Buchanon WW, Goldsmith CH, Campbell J, Stitt L. Validation study of WOMAC: a health status instrument for measuring clinically-important patientrelevant outcomes following total hip or knee arthroplasty in osteoarthritis. Journal of Rheumatology 1988;15:1833-40
18. Kennedy DM, Stratford PW, Wessel J, Gollish JD, Penney D. Assessing stability and change of four performance measures: a longitudinal study evaluating outcome following total hip and knee arthroplasty. BMC Musculoskeletal Disorders 2005;6:3.
19. Podsiadlo D, Richardson S. The timed ‘up and go’. A test of basic functional mobility for frail elderly persons. J Geriatric Soc 1991;39:142-48
20. Hinman RS, K. L. Bennell, K. M. Crossley, J McConnell. Immediate effects of adhesive tape on pain and disability in individuals with knee osteoarthritis. Journal of Rheumatology 2003;42:865-869.
21. Bockrath K, Wooden C, Worrell T, Ingersoll CD, Farr J. Effects of patellar taping on patella position and perceived pain. Medicine and Science in Sports Exercise 1993; 25(9):989-92.
22. Herrington L. The effect of patellar taping on quadriceps peak torque and perceived pain: a preliminary study. Phys Ther Sport 2001;2:23–28.
23. Cowan SM, Bennell KL, Hodges PW. Therapeutic patellar taping changes the timing of vasti muscle activation in people with patellofemoral pain syndrome. Clinical Journal of Sports Medicine 2002;12(6):339- 347.
24. Gilleard W, McConnell J, Parsons D. The effect of patellar taping on the onset of vastusmedialisobliquus and vastuslateralis muscle activity in persons with patellofemoral pain. Phys Ther 1998;78:25– 32.
25. Thumboo J, Chew LJ, Soh CH. Validation of the Western Ontorio and McMaster University Osteoarthritis Index in Asians with osteoarthritis in Singapore. Osteoarthritis Cartilage 2001; 9(5):440-446.
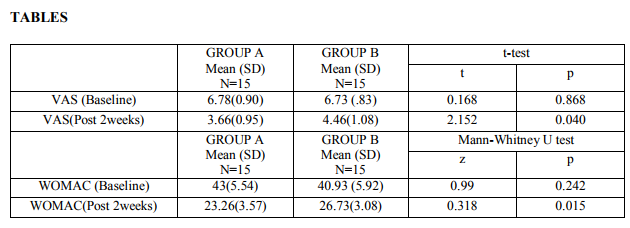
Table 1: It shows the between groups comparison of baseline and post intervention data of Visual Analogue Scale (VAS) and Western Ontario and McMaster University Osteoarthritis Index (WOMAC) along with the results of statistical tests. Baseline VAS and WOMAC scores of group A and group B were 6.78±0.90, 43±5.54 and 6.73±0.83, 40.93±5.92 respectively. Post intervention VAS and WOMAC scores of group A and group B were 3.66±0.95, 23.26±3.57 and 4.46±1.08, 26.73±3.08 respectively. All p values are ≤ 0.05 thus showing significant difference was present between pre and post intervention data.

Table 2: It shows the between groups comparison of baseline and post intervention data of Timed Stair Ambulation Test (TSAT) and Timed Up and Go Test (TUG) along with the results of statistical tests. Baseline TSAT and TUG scores of group A and group B were 21.86±3.73, 19.80±1.85 and 21.66±3.08, 19.06±1.83 respectively. Post intervention TSAT and TUG scores of group A and group B were 16.73±3.91, 14.80±1.65 and 19.13±2.06, 16.33±1.67 respectively. All p values are ≤ 0.05 thus showing significant difference was present between pre and post intervention data.

|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





