IJCRR - 4(22), November, 2012
Pages: 74-84
Date of Publication: 24-Nov-2012
Print Article
Download XML Download PDF
FINE NEEDLE ASPIRATION CYTOLOGY (FNAC) OF PALPABLE LESIONS OF HEAD AND NECK REGION
Author: Richa Sharma, D.R. Mathur
Category: Healthcare
Abstract:Objective: This study is done to evaluate the diagnostic accuracy of FNA in palpable lesions of head and neck region and find out false positive / negative data to analyze the value and limitations of fine needle aspiration cytology (FNAC) in lesions of head and neck region with Cyto-histopathological correlations. Materials and Methods: From 125 cases, fine needle aspiration smears were taken and stained with Giemsa and PAP. Fine needle aspiration cytology results were examined according to the anatomical location and all the lesions were classified into inflammatory and euplastic pathology. The cytological findings were correlated with those of histopathology whenever sent by surgeon. Results: Among 125 cases, histopathological correlations were available only in 71 cases. The sensitivity, specificity, predictive value of the positive test, predictive value of the negative test and were 89.28%, 90.69%, 86.20% and 92.86% respectively. The investigative accuracy of the lymph node, salivary gland, Thyroid gland and soft tissue lesions were 90.14%. Conclusion: It can be concluded from the present study that fine needle aspiration cytology offers a simple method of diagnosis of neoplastic and nonneoplastic lesions of head and neck region. Fine needle aspiration cytology is a simple, quick, economical and non traumatic procedure can easily be carried out in outpatient department or bed sides.
Keywords: FNAC, histopathology, thyroid gland, lymph nodes, salivary glands, soft tissue.
Full Text:
INTRODUCTION
“Fine Needle Aspiration Biopsy (FNAB) is diagnostic procedure in which needle tip functions as a cutting instrument and a negative pressure is created in a syringe and as a result of pressure difference, cellular material is drawn into the needle. It is a harmless, simple, cost effective and precise technique for tissue sampling. The purpose of fine needle aspiration is to obtain diagnostic material for cytological studies from organs that do not shed cells spontaneously. The modern method of fine needle aspiration cytology was originally described and was advocated by Martin and Ellis in 1930 (1), fine needle aspiration cytology has become an important diagnostic technique which has to some extent replaced tissue biopsy in many situations, Stewart (1933) for the first time studied smear obtained by aspiration with the help of 18G needle and diagnosed various tumors arising from prostate, parotid, lymph node, breast, thyroid, testis, soft tissue, bone and abdominal viscera. On the basis of his experience in about 2500 tumors, he observed no untoward complication, encouraging results and established diagnosis. The method is applicable to lesions that are easily palpable; for example superficial growth of the skin, subcutis and soft tissues and organs such as the thyroid, breast, salivary glands and superficial lymph nodes. Modern imaging techniques, mainly ultra-sonography (US) and computed tomography (CT), applied to organ and lesions in site not easily accessible to surgical biopsy offer vast opportunities for per-cutaneous, trans thoracic and trans peritoneal fine needle biopsy of deeper structure. In the practice of fine needle aspiration, there are clear advantage to patient and doctors. The technique is relatively painless, produces a speedy result and is inexpensive (2). Its accuracy when applied by experienced and well trained practitioners can approach unequivocal diagnosis. Although FNAB can be applied to practically every organ and tissue of the body, certain limitation does exist. The four fundamental requirements on which the success of FNAB depends are representativeness, adequacy of the sample and high quality of preparation with relevant and correct clinical / radiological information. These four prerequisites will always remain sine qua non, no matter how sophisticated the supplementary technique (3). The proximity of tissues of various types and the wide range of primary and metastatic neoplasms are responsible for head and neck region being among the most interesting and challenging in FNAC diagnosis. Where incisional biopsies may lead troubles in some sensitive sites, in such circumstances FNAC is a suitable choice, being a minimally invasive technique. A preoperative cytological, diagnosis of a primary neoplasm may permit more appropriate surgery. The majority of head and neck mass are usually superficial and easily accessible to needle biopsy. There is no doubt that as Koss 1980(4) has said “Thin needle aspiration biopsy is a procedure whose time has come” and the pathologists not already versed in the technique will come under increasing and compelling pressure to provide it.
MATERIAL AND METHODS
The present study was carried out in the Department of Pathology, Dr. Sampurananad Medical College and Associate groups of Hospitals, Jodhpur. The material consists of 125 cases of palpable lesions of head and neck region- including lesions of thyroid, salivary gland, lymph nodes and few miscellaneous lesions. The FNA diagnosis was correlated with available subsequent histopathological diagnosis. The patients were selected without any consideration of age, sex.
Following cases were excluded from the study:
- Cases presenting with uncorrectable coagulopathies.
- Where there is lack of safe biopsy route.
- Uncooperative patient
A careful thorough history and clinical examination was done in each case. Routine and specific biochemical investigations were carried out as per individual requirements. FNAC was done without any aids of C.T. or ultrasonic guidance.
Procedure of aspiration
The FNAC was done under full aseptic precautions. Proper preparation and draping of the part was done. Aspiration needle was mounted on syringe and all air from the syringe was expelled. The swelling was identified and fixed by left hand in between thumb and the finger so that skin was stretched and mounted needle was inserted in the central part of swelling by sharp and quick jerk. Its entry into the tumor was felt by change in the resistance to the needle. The negative pressure was created by withdrawing the piston. Usually 2-3 ml of air will create an adequate vacuum.
Statistical analysis
A true positive (TP) FNA is defined as malignant cytological diagnosis from a lesion determined to be malignant after surgical biopsy A false positive (FP) is defined as a malignant FNA diagnosis found to be benign after surgery. A true negative (TN) FNA is defined as benign cytological results from a lesion proved to be benign after surgery. A false negative (FN) FNA is defined as defined as benign cytological diagnosis turned out to be malignant on histology. The following parameters were analyzed according to standard criteria:- Sensitivity: It is defined as the proportion of patient having malignant lesions and positive cytological diagnosis and calculated by TP/ (TP+FN). Specificity: It is the proportion of the patients with nonmalignant lesion and negative cytological finding and calculated by TN / (TN+FP). Positive predictive value: It is the probability of having malignant lesion with positive cytological finding and calculated by TP/ (TP+FP). Negative predictive value: It is the probability that a patient did not have malignant lesion with negative cytological finding and calculated by TN/ (TN+FN). Accuracy: It is the proportion of correct results (true positive and true negative) in relation to all cases studied and calculated by (TP+TN)/ (TP+FP+TN+FN).
RESULTS
The present study was conducted at Pathology Department of Dr. S.N. Medical College, Jodhpur, a total 125 cases of palpable lesion of head and neck region were studied. These patients were assessed clinically and FNAC was performed. The accuracy of FNAC was verified by histological examination in 71 cases. Majority of cases of Fine Needle Aspiration Biopsy performed in the age group of 21-30 yrs. (29.6%) followed by 11-20 yrs. (18.4%) and least number of cases were seen in age group of > 70 (4.8%)Out of 125 cases 76 (60.8) % cases were females and 49 (39.2) % cases were males.
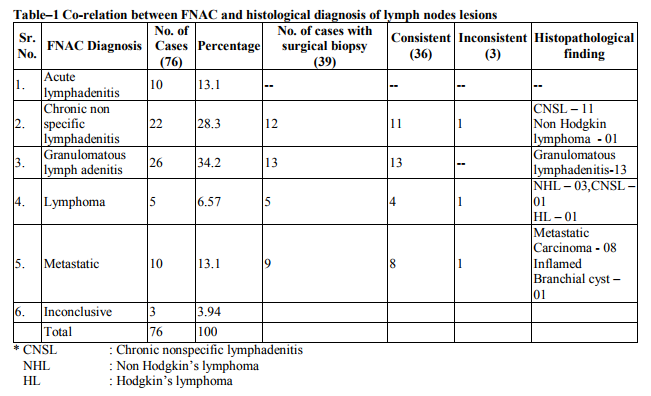
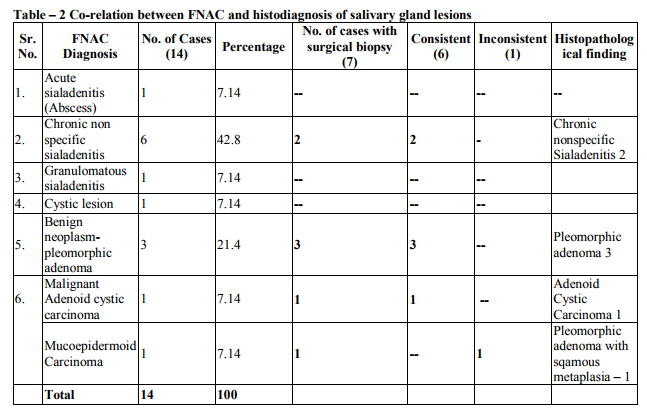
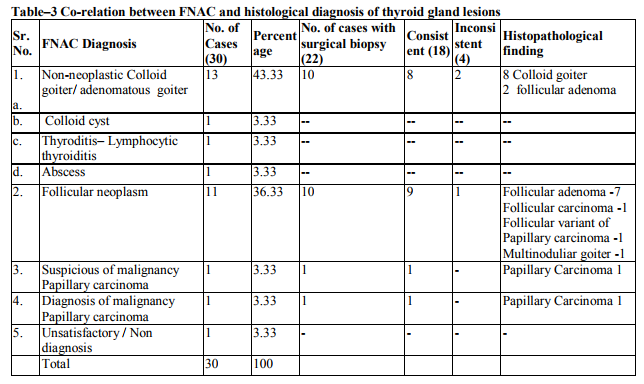
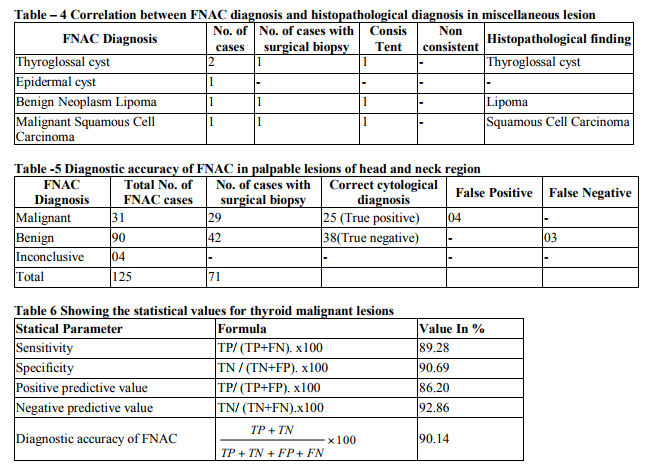
The FNA results of 125 cases were distributed according to site of lesion – thyroid gland 30 case (24%), lymph node 76 cases (60.8%), salivary gland 14 cases (11.2%) and other case of neck (excluding lymph nodes and thyroid) 5 cases (4.0%). Lesions of all site were categorized into group of benign (inflammatory and benign neoplasm) and malignant (primary and secondary) and nondiagnostic (unsatisfactory), on the basis of known criteria. In the lymph node cytologically diagnosed benign lesions were (Granulomatous lymph adenitis 26 cases (34.2%), chronic non specific lymphadenitis 22 cases (28.3%) and acute lymphadenitis 10 cases (13.1%). In Malignant group cytological diagnosis were metastatic carcinoma in 10 cases (13.1%) and lymphoma in 5 cases (6.57%). Histopathological study of 39 cases, confirmed the diagnosis in 36 cases with two false positive and one false negative case. In the salivary gland cytologically diagnosed benign lesions were chronic non specific sialadenitis 6 cases (42.8%), benign neoplasm – plemorphic adenoma 3 cases (21.4%). In Malignant group 1 case was adenoid cystic carcinoma (7.14%) and 1 Mucoepidermoid carcinoma (7.14%). Histopathological study of 7 cases, confirmed the diagnosis in 6 cases with one false positive case, which was cytologically diagnosed as, mucoepidermoid carcinoma, turned out to be pleomorphic adenoma with squamous metaplasia. FNAC of thyroid gland reveled non-neoplastic 16 cases (53.32%), follicular neoplasm 11 cases (36.33%), malignant 2 cases (6.66%), unsatisfactory 1 case (3.33%).
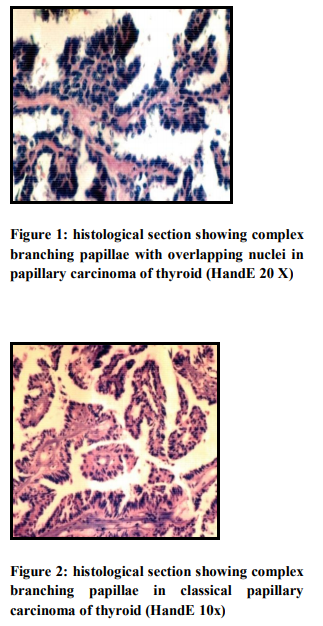
Histopathological correlation in 22 cases, reveled consistent result in 18 cases while one case was found false negative which was cytologically diagnosed as follicular neoplasm turned out to be follicular variant of papillary carcinoma on histology. FNAC of neck site (excluding lymph node and thyroid) benign diagnosis was offered in 4 cases and malignant diagnosis in 1 case. Histological correlation was available in 3 cases and found consistent 100%. The overall accuracy in the 71 cases evaluated was 90.14% with sensitivity of 89.28% and specificity of 90.69%. Positive predictive value and negative predictive value found 86.20% and 92.86% respectively.
DISCUSSION
The present study was conducted in the Department of Pathology, Dr. Sampurnanad Medical College and Associate groups of Hospitals, Jodhpur. The results of 125 cases of aspirates were weighing against with surgically excised specimens obtained in 71 cases which were characteristically processed and stained with Haematoxylin and Eosin stain. In present study, most of the cases on which FNAC was performed were in the age group of 21-30 yrs. There were 37 cases in this age group (29.6%) followed by 11-20 yrs. – 23 cases (18.4%), 0-10 yrs. – 17 cases (13.6%) and minimum number of cases were in age group of >70 years (4.8%) Among the 125 patients, 49 (39.2%) were males and 76 (60.8%) were females and ratio was found to be M: F: 1: 1.5. Tilak et al (2002) performed FNAC in 154 cases of head and neck region and 55 cases were available for surgical biopsy among 55, 16 were male and 39 were female. Ratio was found M: F = 16: 39 = 1: 2.4. (5) In present study, maximum number of fine needle aspiration biopsies were performed from lymph nodes (60.8%) followed by thyroid gland (24%), salivary glands (11.2%) and other sites (neck excluding lymph node and thyroid) 4%.Agarwal et al (2004) performed FNAC in 400 cases of the palpable lesions of head and neck region and incidence was found in lymph nodes (40.5%) thyroid gland (43.5%), salivary gland 7.5% miscellaneous lesion (8%).(6) Peter et al (1989) analyzed 253 cases of FNAC of the palpable lesions of head and neck region. They found incidence in cervical lymph node (61%), thyroid nodules (21%), salivary gland (16%) and miscellaneous (3.2%). (7) In present study incidence was found similar to the Peter et al. In this study, FNAC of the lymph nodes had shown that commonest lesions encountered was granulomatous lymphadenitis (tubercular lymphadenitis) 26 cases (34.2%), 22 cases (28.3%) were of chronic non specific lymphadenitis, 10 cases (13.1%) were diagnosed as acute lymphadenitis.Cytological malignant diagnosis were offered in 15 cases, 10 cases (13.1%) were diagnosed as metastatic carcinoma, and 5 cases (6.57%) were as lymphoma. (Table No. 1) Tilak et al (2002) (5) studied 154 cases of FNAC in the head and neck region and among 18 cases of lymphadenopathy 7 cases (38.8%) were reported as tubercular lymphadenitis. In present study the also most common lesion encountered was tubercular lymphadenitis and our findings are also comparable to study of Tilak et al (2002) (5). FNAC findings of lymph nodes were correlated with histopathological diagnosis in 39 cases (Table No. 1). Histological findings are found to be consistent in 36 cases and in tubercular lymphadenitis correlation was found 100%. Shyamala bhaskaran et al (1990) (8) also reported 100% correlation of cytological diagnosis of tubercular lymphadenitis with histological diagnosis.
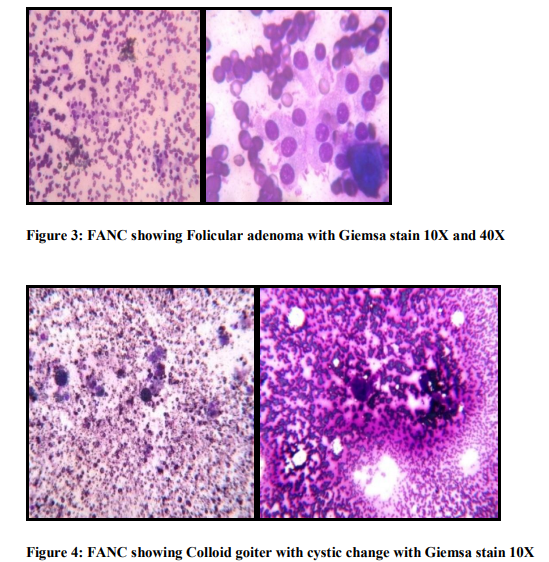
It was concluded that FNAC having high diagnostic accuracy rate for the tubercular lesion on the basis of present study and other workers. In this study, one case was turned out to be Non Hodgkin lymphoma which was cytologically diagnosed as chronic non specific lymphadenitis (i.e. false negative) and one case was turned out to be reactive follicular hyperplasia which were cytologically diagnosed as Non Hodgkin lymphoma (i.e. false positive cases) one case which was cytologically diagnosed as Hodgkin lymphoma very well correlated histolgically. Such false negative/ false positive results are also present in review. According to Frable et al (1988) (9) and, Hehn et al (2004) (10) FNAC is used primarily for documentation of residual recurrent lymphoma or to assess the stage of the disease. (9, 10) The use of FNA to render a primary diagnosis of lymphoma remains controversial. The differential diagnosis between prominent follicular hyperplasia and follicular lymphoma grade 1-2 (Centroblastic / Centracytic) can be very difficult in FNAB smears. The difficulty in distinguishing the two conditions is largely due to the fact that dendritic reticulum cells associated with centroblasts and centrocytes are seen in both conditions, and that interfollicular areas in follicular lymphoma may contain large number of lymphocyte. Borges et al (1991) study and present study revealed that primary diagnosis of lymphoma and its classification must be made on an adequate tissue biopsy. (11) In this study, one case was turned out to be inflamed branchial cyst which was cytologically diagnosed as Metastatic carcinoma (i.e. False positive). The distinction between an inflamed branchial cyst and a node metastasis of well-differentiated squamous cell carcinoma with liquifactive necrosis is a particular problem (12). Both false negative and false positive diagnosis have been reported. Given the prevalence of both these conditions, this is one of the most important causes of misdiagnosis in the head and neck. Tilak et al (2002) was also showed one false positive case in their study. They stated that it was due to poorly fixed smear. So this highlights the necessity of making a cytological diagnosis in a known clinical context and the importance of adequate fixation of smears.(5) In present study total 30 cases (24%) were aspirated from thyroid gland cytological diagnosis was classified in five groups, based on standard criteria reported in the literature Mcnicol et al (2004)(13). Maximum cases (13 cases 43.33%) were cytologically diagnosed as colloid goiter followed by follicular neoplasm 11 cases (36.66%). Cytological suspicion of papillary carcinoma was offered in one case and definite diagnosis of malignancy (typing papillary carcinoma) was given in one case. Cytological material was found inadequate for giving definite opinion in one case (Table No. 3). 22 cases were correlated with histological diagnosis. (Table No. 9). Histological findings were found to be consistent in 18 cases. Two cytologically diagnosed case of adenomatous goiter were turned out to be follicular adenoma in histology. The cytological appearances in colloid goiter form a continuum which merge with those of follicular adenoma, and in this grey area, cytological criteria alone cannot reliably distinguish between the two. (14) If a micro follicular focus in a nodular goiter is selectively sampled, the smear shows a repetitive pattern of microfollicles or rosettes with no colloid and the distinction from follicular neoplasm may be impossible. Mehdi et al (2003) (15) studied FNAC of 100 cases of thyroid swelling and surgical biopsy available in 34 cases. They also observed in their study that histological examination results were consistent with cytological findings except in two cases, where one case of colloid cyst and another of colloid goiter turned out to be follicular adenoma. In present study, one cytologically diagnosed case of follicular neoplasm turned out to be follicular carcinoma on histopathology and 7 follicular neoplasm were benign follicular adenoma. The cytological findings in follicular adenoma and follicular carcinoma are similar. Lowhagen advocated that a cytological report should only state that a follicular neoplasm is present with no implication of its benign or malignant nature (Lowhagen et al 1974) (16). In present study 81% results are found to be consistent in thyroid FNAC and 18.18% were not consistent and 3.33% were inadequate. One cytologically diagnosed case of follicular neoplasm was turned out to be follicular variant of papillary carcinoma (False Negative) and one case turned out multinodular goiter in histology. The follicular variant of papillary carcinoma may have well-formed follicles containing colloid, and cystic papillary tumors often contain abundant colloid. This can cause diagnostic difficulties if smears are poor in cells. Gagneten (1987) stressed the importance of doing multiple aspirations in a thyroid swelling in order to obtain representative material from different area.(17) In this study two cases of papillary carcinoma were diagnosed cytologically and very well confirmed histologically. Kumar et al (1999) analyzed cytological findings in 15 cases of follicular variant of papillary thyroid carcinoma (histologically proven). (18)They considered that Adenomatous colloid goiter and follicular adenoma are differential diagnosis of follicular variant of papillary carcinoma due to presence of microfollicles but the presence of numerous colloid balls with multilayered microfollicles (rosettes) are cytological finding of follicular variant of papillary thyroid carcinoma. In present study FNAC were done from salivary gland in 14 cases out of which 7 cases were correlated with histological findings (Table No.2). Maximum cases (6 cases 42.8%) were cytologically diagnosed as chronic non specific sialadenitis. Surgical biopsies available in two cases were found to be consistent. In this study 3 cases (21.4%) were diagnosed as pleomorphic adenoma and all were confirmed histologically. Tilak et al (2002) also reported 100% accuracy of FNAC for diagnosis of pleomorphic adenoma. In present study diagnostic accuracy of the FNAC for pleomorphic adenoma was found comparable to the other workers i.e. 100 %.( 5) In this study one case which was diagnosed mucoepidermoid carcinoma cytologically turned out to be pleomorphic adenoma with extensive squamous metaplasia on histologically. According to Klijanlenko et al (1997), aspiration of mucoid fluid may suggest low grade mucoepidermoid carcinoma. Multiple sampling is important to overcome the problems due to selective sampling. Epithelial metaplasia, mainly squamous and oncocytic, is often seen in plemorphic adenoma. Goblet cells are some time present and squamous metaplasia can be a prominent feature. (19) If a squamous component is selectively sampled by FNB and if the metaplastic cells appear atypical, the possibility of low grade mucoepidermoid tumor may be considered but the presence of groups of bland myoepithelial cells typical of plemorphic adenoma and a few fragments of myxoid stroma suggest the correct diagnosis. In present study one case was cytologically diagnosed as adenoid cystic carcinoma and confirmed histologically. Parijatham et al (2003) studied 40 cases of FNAC from salivary gland. Their study showed 100% accuracy rate for adenoid cystic carcinoma and chronic non specific sialadenitis, 90% for pleomorphic adenoma. Results obtained in our study, were very comparable to the study of Parijatham et al. (20)
Among the five cases of the neck lesions excluding lymph nodes and thyroid gland. 3 cases were correlated histologically (Table No.4).In one case a cytologic diagnosis of lipoma was suggested, which was confirmed histologically. A cytological suspicion of malignancy was considered in one case which was subsequently proved to be infiltrating squamous cell carcinoma. In this study out of 125 cases, 71 cases of FNA were correlated with histopathology. The overall accuracy rate of FNA cytology was 90.14% with the sensitivity 89.28% and specificity 90.69%.Positive predictive value and negative predictive value found 85% and 96.07% respectively. However, the results of present study correlated well with those of Tilak et al (2002) studied FNAC 154 cases of the palpable region of the head and neck region, 55 cases were available for histopathological correlation. Overall diagnostic accuracy was found 92.73% with sensitivity 90.91% and specificity 93.18 %.( 5) It can be said that results of this study compare favorably with those in published literature and are fairly accurate.
CONCLUSION
FNAC is an excellent first line method for investigating the nature of palpable lesions in the head and neck region. It can obviate the need for surgery if the lesions are shown to be nonneoplastic or can provide most useful information to the surgeon to determine the further mode of management. FNAC is having high accuracy rate to differentiate benign and malignant nature of the lesions. To obtain maximum diagnostic accuracy from the FNAC, close cooperation between a committed and trained cytopathologist and an experienced clinician is essential.FNAB is a simple, quick, economical and non traumatic procedure can easily be carried out in outpatient department or bed sides.
References:
1. Martin HE, Ellis EB, Aspiration biopsy. Surg. Gynecol obstet 59, 578-589, 1934.
2. Frable WJ. Thin-needle aspiration biopsy. Philadelphia : Saunders ; 1983
3. Orell SR : Fine needle aspiration cytology, 2005.
4. Koss LG : Thin needle aspiration biopsy (editorial). Acta Cytol 24 : 1-3, 1980.
5. Vijay Tilak. A.V. Dhaded, Ragini Jain et al : Fine needle aspiration cytology of Head and Neck masses. Indian J. Pathol. Microbiol 45(1) 23-30, 2002.
6. Agarwal S. Khan MA et al : FNAC as a diagnostic tool in head and neck lesions on their histopatholgical correlations. Indian J. Pathol Microbial 47(1) 135-136, 2004.
7. Peters B. Robert et al : Inter observer variability in the interpretation of fine needle aspiration biopsy of head and neck masses. Arch otolaryngol Head Neck Surg., 115, Number 12, 1438-1442, 1989
8. Shyamala Bhaskaran et al : Fine needle aspiration cytology, review of 1731 cases. Indian J. Pathol. Microbiol, 33, 392-395, 1990.
9. Frable WJ, Kardos TF. Fine needle aspiration biopsy : Application in the diagnosis of lymphoproliferative diseases. AM J. Surg Pathol 12: 62-72, 1988
10. Hehn ST, Miller TP. Utility of fine needle aspiration as a diagnostic technique in lymphoma. J Clin oncol 22 : 3046-3052, 2004.
11. Borges Anita: Aspiration cytology in the management of head and neck masses. In Aspiration cytology for clinicians and pathologists eds Kishnamurthy SC, Tata Memorial Centre, Bombay, PP 48-47, 1991.
12. Ustun et al Cystic change in metastatic lymph nodes: a common diagnostic pitfall in fine needle aspiration cytology. Diagn cytopathol 27, 387-392, 2002.
13. Mc Nicol AM : Criteria for diagnosis of follicular thyroid neoplasms and related conditions. Recent Advances in histopathology 20, 1-10, 2004.
14. Orell SR. et al : Fine needle aspiration cytology the thyroid gland 4th edition, 139- 142, 2005.
15. Syed Riaz Mehdi, Shaista M. Vasenwala, Mohd. Shoaib Zaeer : Role of FNAC and antithyroid antibodies in the diagnosis of thyroid disorders. Indian J. Pathol Microbiol 46(2) : 184-190, 2003.
16. Lowhagen T, Sprenger E. Cytologic presentation of thyroid tumors in aspiration biopsy smear. A review of 60 cases. Acta Cytol 18 : 192-194, 1974.
17. Gagneten C.B. Lowenstein A : The role of fine needle aspiration biopsy cytology in the evaluation of the clinically solitary thyroid nodule. Acta Cytol 31 : 595 – 598, 1987.
18. Kumar et al (1999) Follicular variant of papillary carcinoma of the thyroid : A cytologic study of 15 cases. Acta Cytol 43 : 139- 142, 1999.
19. Klijanienko J. Vielh P. Fine needle sample of salivary gland lesions IV. Review of 50 cases of mucoepidermoid carcinoma with histologic correlation. Diagn cytopathol 17 : 92-98 1997b.
20. Parijathan, B. et al : FNAC of salivary gland with hisopathologic correlation. Indian J. Pathol Microbiol Vol. 46 No. 2. Page No. 306, 2003.

|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





