IJCRR - 4(24), December, 2012
Pages: 119-123
Date of Publication: 22-Dec-2012
Print Article
Download XML Download PDF
MANAGEMENT OF ORAL PYOGENIC GRANULOMA - A CASE SERIES
Author: Mythireyi D., K. Vinayagavel
Category: Healthcare
Abstract:Background: Pyogenic granuloma is a reactive tumor like lesion frequently seen in the oral cavity. It occurs in response to various stimuli such as chronic low grade irritation, traumatic injury, hormonal factors etc. It predominantly occurs in second decade of life in young females, possibly because of vascular effects of female hormones. Lesions have a similar frequency throughout the world. No racial predilection is reported. Clinically, pyogenic granuloma is a smooth or lobulated exophytic lesion manifesting as small, red erythematous papules on a pedunculated or sometimes sessile base. Treatment consists of surgical excision along with eradicating the causative agents. Recurrence of the lesion can be prevented by complete excision of the lesion and by following proper oral hygiene measures by the patient. This article describes three cases which have been successfully managed and maintained.
Keywords: pregnancy tumor, pyogenic granuloma, surgical excision
Full Text:
INTRODUCTION
Pyogenic granuloma is one of the most common reactive tumor like lesion seen in the oral cavity. Hullihen’s1 description in 1844 was most likely the first pyogenic granuloma reported in English literature but the term “pyogenic granuloma” or “granuloma pyogenicum” was introduced by Hartzell2 in 1904. Pyogenic granuloma arises in response to various stimuli such as chronic low grade irritation, traumatic injury, hormonal factors or certain kind of drugs. It predominantly occurs in second decade of life in young females, possibly because of vascular effects of female hormones3 . Lesions have a similar frequency throughout the world. No racial predilection is reported. Although it was originally thought to be caused by pyogenic organisms, it is now believed to be unrelated to infection. So the term pyogenic granuloma is a misnomer because the lesion does not contain pus and is not strictly a granuloma. The pyogenic granuloma has been called “pregnancy tumor” and occurs in 1% of pregnant women3,4 . Clinically, pyogenic granuloma is a smooth or lobulated exophytic lesion manifesting as small, red erythematous papules on a pedunculated or sometimes sessile base, which is usually hemorrhagic or compressible and may develop as a dumb bell shaped mass3 . This article describes three cases of pyogenic granuloma that were successfully managed.
CASE REPORT
1 A male patient 26 yrs of age reported to a private clinic with a chief complaint of growth in the inner aspect of gums of upper front teeth since 15 days. The growth which was initially a pin head size slowly increased to its present size and was stable. No relevant medical history. On intra oral examination, a small triangle shaped growth with its base at the incissive papilla on the palatal aspect of upper anterior teeth was seen. The growth was 0.5cm * 0.3cm in size, firm fibrotic with no associated bleeding on probing. The oral hygiene status was poor. Intra oral periapical radiograph revealed no bone loss. Non surgical periodontal treatment was opted. The treatment consisted of oral prophylaxis and oral hygiene motivation. When the patient was recalled for review after one week the lesion had subsided.
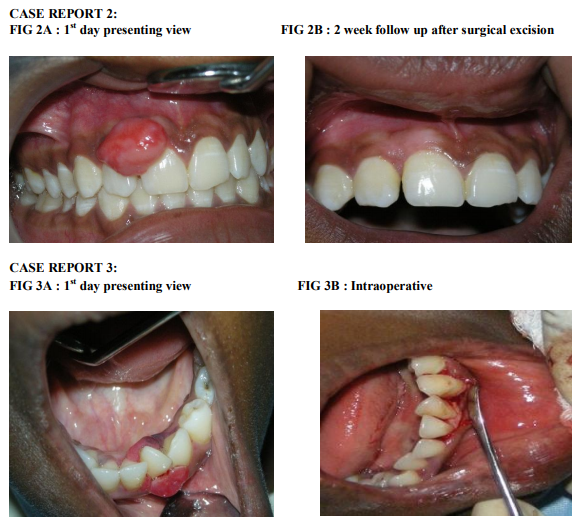
CASE REPORT 2
A 15 yr old female patient reported with a chief complaint of swelling in upper anterior region since 1 month. On intra oral examination there was a single well defined pedunculated swelling 3cm*2cm between right maxillary central and lateral incisor. Lesion was firm, fibrotic and non tender on palpation. The oral hygiene status was fair. The treatment comprised of oral prophylaxis and oral hygiene motivation. After one week , surgical excision of the lesion was done. Histopathological report revealed proliferating stratified squamous epithelium. Underlying connective tissue showed dilated blood vessels and inflammatory cell infiltration. On follow up after one year patient was normal with no symptoms of recurrence.
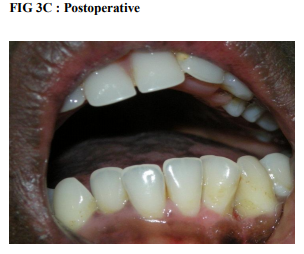
CASE REPORT 3
A 17 yr old female patient reported with a chief complaint of enlargement of gums in relation to lower front tooth region for the past 1 year. On examination there was a dumb bell shaped lesion in relation to 32,33 extending from labial to the lingual aspect in relation to mandibular anterior teeth. On palpation the lesion was soft and vascular with a tendency to bleed. Treatment plan consisted of oral prophylaxis followed by surgical periodontal management. On the first day through oral prophylaxis was done. Patient was recalled after 1 week and was reviewed. Since the lesion was still vascular surgical excision followed by periodontal flap surgery for through debridement was done. Histopathological report showed proliferating parakeratinised epithelium. Underlying connective tissue showed inflammatory cell infiltration and engorged blood vessels. Follow up after six months showed no symptoms of recurrence.
DISCUSSION
Pyogenic granuloma is a non neoplastic growth in the oral cavity. It may vary in size from few millimeters to several centimeters and are often painless. Gingiva is the most common site of occurrence accounting about 75% of all cases5 . According to Vilmann et al6 , majority of pyogenic granulomas are found on the marginal gingiva with only 15% of the tumors on the alveolar part. Other common sites are lips, tongue and buccal mucosa. Since it is a reactive tumor like lesion, chronic low grade irritation, traumatic injury, hormonal factors and certain kind of drugs could be considered as etiologic agents. Poor oral hygiene may be a precipitating factor in many patients3,4,5 . Many treatment techniques have been described for pyogenic granuloma. But before treating any case the etiology must be clearly identified and eradicated. Before attempting surgical excision of the lesion, a thorough oral prophylaxis should be done, because local factors such as plaque and calculus are the most important etiologic factors for pyogenic granuloma. If the lesion is small, painless and free of bleeding, oral prophylaxis, removal of causative irritants (foreign materials, source of trauma) and follow up is advised. The first case was managed successfully with the above mentioned treatment modality. If the lesion is large, a thorough oral prophylaxis followed by surgical excision extending down to the periosteum should be done along with scaling of adjacent teeth to remove the source of continuing irritation. The second and third cases were managed with this treatment plan. Other treatment protocols also have been suggested. Powell et al7 reported the use of Nd: YAG laser for excision of the lesion because of the lower risk of bleeding compared to other surgical techniques. White et al8 proposed that CO2 and Nd:YAG laser irradiation is successful in surgical management. Meffert et al9 used flash lamp pulsed dye laser on a mass of granulation tissue which did not respond to the usual treatment methods and concluded that previously resolute tissue responded well to a series of treatments with the pulsed dye laser. Ishida and Ramos-e-Silva10 believed that cryosurgery is a very useful technique for the treatment of pyogenic granuloma. Moon et al11 reported that sodium tetradecyl sulfate sclerotherapy successfully cleared the lesions in most patients without major complications. Parisi et al12 used a series of intralesional corticosteroid injections for treatment of pyogenic granuloma, particularly highly recurrent lesions. Preventive measures consists of adequate home care measures with regular dental check up and oral prophylaxis especially during pregnancy. Lesions removed during pregnancy may have a higher recurrence rate. After excision recurrence occurs in upto 16% of the lesions. Recurrence is believed to result from incomplete excision, failure to remove etiologic factors or re injury of the area. Some recurrences manifest as multiple deep satellite nodules that surround the site of the original lesion3 . Differential diagnosis of pyogenic granuloma includes peripheral giant cell granuloma, peripheral ossifying fibroma, peripheral odontogenic fibroma, hyperplastic gingival inflammation, Kaposi’s sarcoma, bacillary angiomatosis, angiosarcoma, metastatic cancer and hemangioma13 .
CONCLUSION
Pyogenic granuloma is a relatively common tumor like lesion of oral cavity. Successful management necessitates proper diagnosis and treatment planning. Although excisional surgery is the treatment of choice for pyogenic granuloma, removal of causative agents should be the first line of treatment. After surgical excision patient should follow proper oral hygiene measures to prevent recurrence of the lesion. High recurrence rate of this lesion could be attributed to improper excision of the lesion, or improper surgical debridement or failure of the patient to maintain proper oral hygiene. Importance of strict oral hygiene measures must be stressed to the patient.
ACKNOWLEDGEMENT
Authors acknowledge the great help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors and publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. Authors are grateful to IJCRR editorial board members and IJCRR team of reviewers who have helped to bring quality to this manuscript.
References:
1. Hullihen SP (1844) Case of aneurism by anastomosis of the superior maxillae. Am J Dent Sc 4, 160 -162
2. Hartzell MB (1904) Granuloma pyogenicum J Cuttan Dis Syph 22, 520-525
3. Hamid Jafarzadeh, Majid Sanatkhani et al (2006) oral pyogenic granuloma: a review vol 48 no 4 167 -175
4. Neville BW, Damm ,Allen CM, Bouquot JE (2009) oral and maxillofacial pathology 3rd ed, WB Saunders, Philadelphia, 517-518
5. Regezi JA, Sciubba JJ, Jordan RCK (2003) Oral Pathology : ClinicalPathology Consideration 4th ed , BC Decker, Hamilton 141-142
6. Vilmann A, Vilmann P, Vilmann H (1986) Pyogenic granuloma evaluation of oral conditions. Br J Oral Maxillofac Surg 24, 376 – 382
7. Powell JL, Bailey CL, Coopland AT, Otis CN, Frank JL, Meyer I(1994) Nd:YAG laser excision of a giant gingival pyogenic granuloma of pregnancy. Lasers Surg Med 14, 178-183
8. White , Chaudhry SI, Kuder JJ, Sekandari N, Schloelch ML, Silverman S Jr(1998) Nd:YAG and CO2 laser therapy of oral mucosal lesions. J Clin Laser Med Surg 16, 299 -304
9. Meffert JJ, Cagna DR, Meffert RM (1998) Treatment of oral granulation tissue with the flashlamp plsed dye laser. Dermatol Surg 24, 845 -848
10. Ishida CE, Ramos-e-Silva M (1998) Cryosurgery in oral lesions. Int J Dermatol 37, 283-285
11. Moon SE, Hwang EF, Cho KH ( 2005) Treament of pyogenic granuloma by sodium tetradecyl sulfate sclerotherapy. Arch Dermatol 141, 644-646
12. Parisi E, Glick PH, Glick M (2006) Recurrent intraoral pyogenic granuloma with satellitosis treated with corticosteroids. Oral Dis 12, 70- 72
13. Kamal R, Dahiya P, Puri A. ( 2012 ) Oral pyogenic granuloma: Various concepts of etiopathogenesis. J Oral Maxillofac Pathol ;16:79-82

|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





