IJCRR - 4(24), December, 2012
Pages: 43-51
Print Article
Download XML Download PDF
A CROSS-SECTIONAL STUDY OF MORBIDITY PATTERN OF RURAL AGRICULTURAL WORKERS IN SOUTH INDIA
Author: Kulkarni Rajesh R., Shivaswamy M.S., Mallapur M.D.
Category: Healthcare
Abstract:Background and aims: 72% of Indian population lives in rural area, where their main occupation is agriculture. Agriculture workers do not have trade unions and have no access to occupational health services. The present study was aimed to know the morbidities of agricultural workers. Methods and Material: This cross-sectional study was done from January 2009 to December 2009 among 400 agricultural workers of age 16 to 60 years residing at a sub-centre area of the PHC administrated by Medical College in South India, using predesigned and pretested questionnaire. Statistical analysis was done by using percentages and chi square test. Results: Among the study participants 55.75% were men and 44.25% were women, with male to female ratio of 1.25:1. Most of the agricultural workers (89.5%) were Hindus and 47% were illiterates; of the 400 study participants, 295 (73.75%) belonged to Class V socio-economic status. Majority (62%) of agricultural workers suffered from morbidities associated with oral cavity, followed by morbidities associated with musculoskeletal system (21.7%) and respiratory system (19%). Increasing age, gender and poor educational status were significantly associated with morbidities of oral cavity, musculoskeletal system, respiratory system, anaemia and animal bites. Conclusion: The present study suggests that, agricultural workers had a multitude of health problems. In order to overcome the situation, information, education and communication (IEC) activities needs to be strengthened and special health check-up camps to be conducted with emphasis on improvement of health.
Keywords: Agricultural workers; Morbidity pattern; Occupational health
Full Text:
INTRODUCTION
The literature linking health to labour productivity is built on the concepts of household production theory developed by Becker (1965). In Becker’s framework, households are treated also as producers of “commodities” instead of solely consumers of goods and services. This framework was extended by Grossman (1972, 1999) to analyze the demand for health. In Grossman’s model, health is viewed as a durable capital stock that yields an output of healthy time. [1] India lives in its 600,000 villages. Nearly 72% of Indian community lives in rural area, where their main occupation is agriculture. Indian agriculture accounts for 25% of total gross domestic product (GDP) on which 75% of country’s population depends on. Agricultural workers do not have trade unions and have no access to occupational health services. [2] Occupational health in the agricultural sector is a new concept. These agricultural workers have a multitude of health problems, a fact which is often forgotten because of misconception that occupational health is mainly concerned with industry and industrialized countries. These health problems of workers in agriculture may be accidents (machine injuries, snake and insect bites), toxic hazards (chemical exposures and insecticide poisoning), physical hazards (extreme conditions, solar radiation), respiratory problems (farmer’s lung, occupational asthma). [3] A study of women farmers in mixed cropping systems found that the vast majority suffered from intense muscular fatigue, heat exhaustion, and skin disorders, forcing them to take days off from attending to crops.[4] Poor health will result in a loss of days worked or in reduced worker capacity, which, when family and hired labour are not perfect substitutes or when there are liquidity constraints, is likely to reduce output.[5] For example, prolonged exposure to pesticides could cause cardiopulmonary problems, neurological and hematological symptoms, and adverse dermal effects, which could significantly hamper farmers’ work capacity in the field and reduce their management and supervision abilities.[6] As pointed by the World Bank (2007), illness and death from HIV/AIDS, malaria, tuberculosis and other diseases reduce agricultural productivity through the loss of labour, knowledge of productive adults and assets to cope with illness. [7] Morbidity has been defined by World Health Organization (WHO) as any departure, subjective or objective, from a state of physiological well being. The term is used equivalent to such terms as sickness, illness, disability etc. The WHO Expert Committee on Health Statistics noted in its sixth report that morbidity could be measured in terms of three units that is persons who were ill, illness (period or spell of illness) that these persons experienced and duration (days, weeks etc) of these illnesses. [8] The lack of coordination of policy making between agriculture and health undermines efforts to overcome ill health among the rural poor and gives short shrift to agriculture’s role in alleviating many of the world’s most serious health problems. [9] .
AIMS AND OBJECTIVES
To assess the morbidity pattern of agricultural workers residing in rural field practice area of Medical College in South India
MATERIALS AND METHODS
Study design, period and area This community based cross-sectional study was conducted from January 2009 to December 2009 in the rural field practice area of Primary Health Center (PHC) attached to Medical College in South India. The PHC has five sub-centers catering 18 villages having total population of 31,510. One sub-centre was selected among the five sub-centres using sample random sampling technique. Sample size and technique Since no previous studies had been recorded on agricultural workers morbidity in this area, the prevalence was considered to be 50% and the sample size was calculated as 400. All agricultural workers residing in six villages coming under selected sub-centre were listed. By four digit random number table method, 400 participants were selected. Selection criteria Agricultural workers residing in the study area for at least one year preceding the date of survey aged between 16 years to 60 years were included in the study. Recent migrants, pregnant and lactating women working as agricultural workers were excluded from the study. Procedure The study was approved from Institutional Ethics Committee of the Medical College. The study participants were interviewed in their households/fields. Based on the selection criteria, the study participants were selected and written informed consent was obtained from all the participants. The data was collected using predesigned and pretested proforma. Data regarding demographic variable like place of residence, age, sex, education status, marital status, socio-economic status and type of family were recorded. The personal history was taken for diet, sleep pattern, appetite and personal habits. Study variables Self reported illness symptoms experienced by the subjects (one month preceding the survey) were enquired and noted. History of trauma, animal bite, allergy, zoonotic diseases, and poison consumption one month preceding the survey were enquired and noted. A thorough general physical examination and systemic examination was conducted by the investigator to know the morbidities. Two more subsequent visits were made to collect data from those who were absent during first visit. Statistical analysis The data was tabulated using MS Excel sheet and analysis was done using percentages, rates and ratios. Chi square test was used to find the association between attributes.
RESULTS
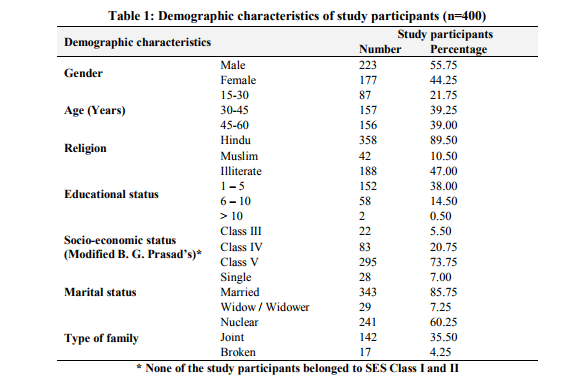
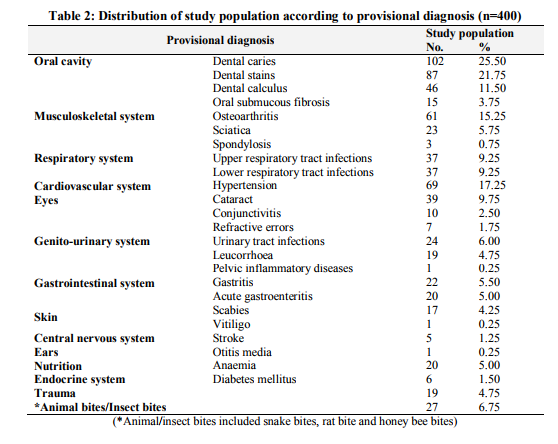
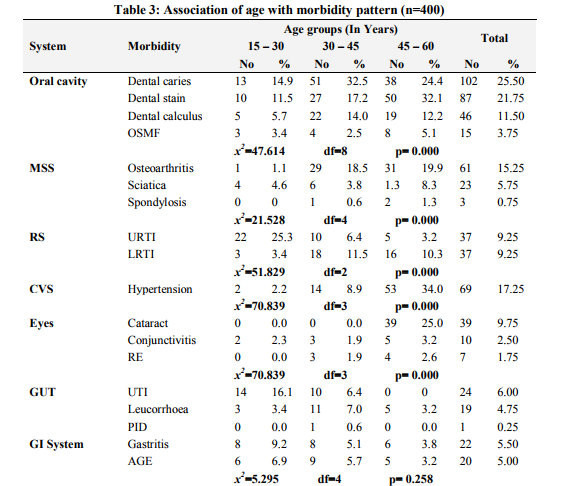
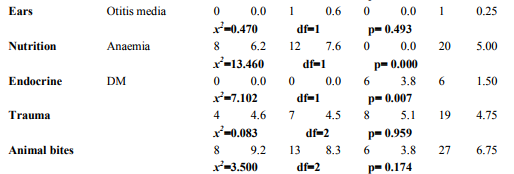
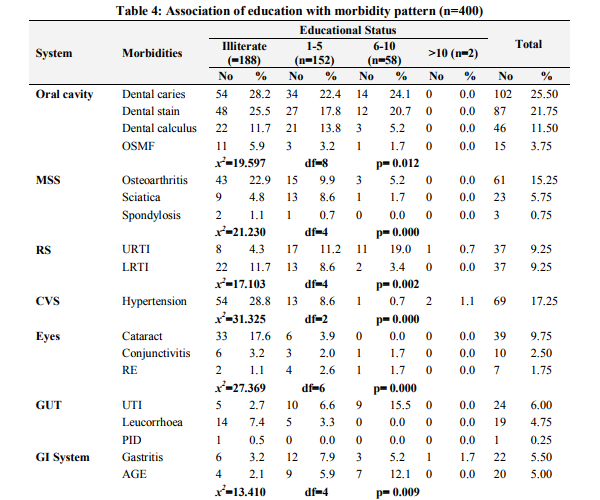
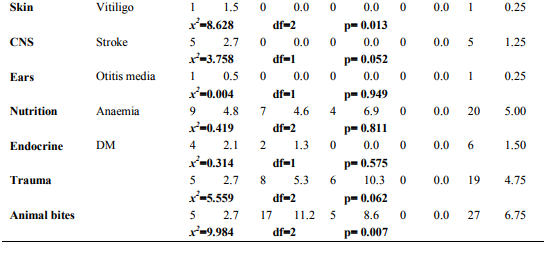
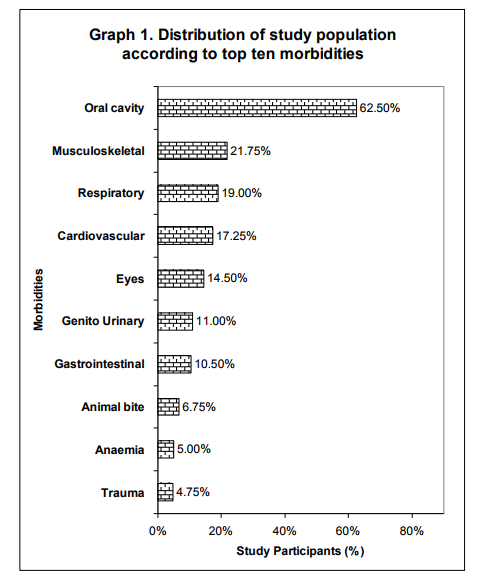
Among the study participants 55.75% were males and 44.25% were females with male to female ratio of 1.25:1. Equal distribution (39%) was seen in the age group of 30 to 45 years and 45 to 60 years. There were 87 (21.75%) people with age between 15 to 30 years. Majority of the people were (89.5%) Hindus and 10.5% were to Muslims. The other demographic features are as shown in Table 1. Morbidity Pattern The general physical examination revealed majority (31%) had pallor, followed by fever (10.75%), skin abnormalities (4.5%), icterus (0.5%) and kyphosis (0.25%). The tachycardia and tachypnoea were noted in 20.25% and 9.75% respectively. The blood pressure measurement findings showed 17.25% of subjects had hypertension. Provisional diagnosis among the study participants showed, majority (62%) suffered from morbidity associated with oral cavity like dental caries (25.50%), dental stains (21.75%), dental calculus (11.50%) and oral submucous fibrosis (3.75%). The other morbidities seen were as mentioned in Table 2. Among the top ten morbidities, majority (62.5%) of the study participants had morbidities associated with oral cavity followed by musculoskeletal system (21.75%) and respiratory system (19%) (Graph 1). The present study showed significant association between morbidities of oral cavity, musculoskeletal system, respiratory system, cardiovascular system, eyes, central nervous system, anaemia and endocrine system with increasing age (Table 3). Also significant association was found between morbidities of oral cavity, musculoskeletal system, respiratory system, cardiovascular system, eye, gastrointestinal system, skin and animal bites with educational status (Table 4). However no significant association was found between socioeconomic status with morbidity pattern.
DISCUSSION
India, a land of agriculture, has formed the scaffolding for many agro-based industries. Morbidity is more common among these industrial workers; being a developing nation, India is faced with traditional public health problems like communicable diseases, malnutrition, poor environmental sanitation and inadequate medical care.[10] However, globalization and rapid industrial growth in the last few years has resulted in emergence of occupational health related issues. Agriculture is the main occupation in India giving employment to about 58% of the people. This is in contrast to the industrialized nations, like USA and Western Europe, where the employment in the agricultural sector is between 4 - 12%. [11]
Agriculture being the principle occupation in the country exposes a considerable proportion of population to this occupational related hazard. The major occupational diseases/morbidity of concern in India are silicosis, musculo-skeletal injuries, coal workers’ pneumoconiosis, chronic obstructive lung diseases, asbestosis, byssinosis, pesticide poisoning and noise induced hearing loss. [11] India is a developing nation and presents the demographic features similar to the other developing nations of the world. Emerging occupational health problems are to be tackled along with the existing traditional public health problems like communicable diseases, malnutrition, poor environmental sanitation and inadequate medical care. [11] Hence the present study was undertaken to assess the morbidity pattern of agricultural workers. In the present study among the study participants majority (62%) suffered form morbidity associated with oral cavity like dental caries (25.50%), dental stains (21.75%), dental calculus (11.50%) and oral sub-mucous fibrosis (3.75%), followed by musculoskeletal system (21.75%) and respiratory system (19%). The statistics for the over [11] A study estimated an annual incidence of occupational disease between 924,700 and 1,902,300 and 121,000 deaths in India. [12] Based on the survey of agriculture injury incidence study in Northern India, they estimated annual incidence of 17 million injuries per year, (two million moderate to serious) and 53,000 deaths per year in agriculture alone. [13] A study in 2006 showed that women farmers in mixed cropping systems found that the vast majority suffered from intense muscular fatigue heat exhaustion and skin disorders .[4] According to ILO, the agricultural sector is one of most hazardous health world wide. Agricultural work possesses several characteristics that are risky for health; exposure to wealth, close contact with animals and plant, extensive use of chemicals and biological products, difficult working posture and lengthy house and use of hazardous agricultural tools and machinery. [14] In the present study significant association was found between morbidities of oral cavity like dental caries, dental stain, dental calculus, Oral submucous fibrosis, musculoskeletal system, morbidity like osteoarthritis, sciatica, spondylosis, respiratory system, morbidities like upper respiratory tract infection, lower respiratory tract infection, hypertension, eye morbidities, stroke, anaemia, diabetes mellitus with increasing age. Also morbidities of oral cavity, musculoskeletal system, respiratory system, cardiovascular system, eyes, gastrointestinal system, skin trauma and animal bites were significantly associated with educational status of study participants. However, this study finding were limited to the self reported symptoms and signs elicited only and laboratory investigations could not be done in all cases due to time restraint.
CONCLUSION AND RECOMMENDATIONS
Agricultural workers had a multitude of health problems associated with oral cavity, musculoskeletal and respiratory system. Creating awareness about benefits of toilets and harms of open air defecation may help to reduce the morbidities to a greater extent. Further strengthening the information, education and communication (IEC) activities and special health check-up camps with emphasis on improvement of health and awareness could help to combat the situation. CONFLICT OF INTEREST: None
ACKNOWLEDGEMENTS
Dr. V. D. Patil, Principal Jawaharlal Nehru Medical College, Belgaum for the permission to conduct this study; Staff of Primary Health Centre, Vantmuri and Sub centre of Bhutaramanahatti, Belgaum and all study subjects who participated in the study for their cooperation in data collection.
References:
1. Ulimwengu J. Farmers’ health and agricultural productivity in rural Ethiopia. AFJARE 2009; 3(2): 83-100.
2. Lal S, Adarsh, Pankaj. Text book of Community Medicine – Preventive and Social Medicine. 2nd ed., New Delhi: CBS Publishers; 2009.
3. Park K. Park’s Textbook of Preventive and Social Medicine. 20th Ed., Jabalpur, India: Banarasidas Bhanot; 2009.
4. Cole D. Understanding the Links between Agriculture and Health for Food, Agriculture, and the Environment. Washington, DC; International Food Policy Research Institute (IFPRI): 2006.
5. Antle JM, Pingali PL. Pesticides, productivity, and farmer health: A Philippine case study. American J of Agricultural Economics 1994; 76(3): 418–30.
6. Spear R. Handbook of Pesticide Toxicology: General Principles. New York: Academic Press; 1991.
7. World Bank. World Development Report: Agriculture for development. Washington, DC: The World Bank; 2007.
8. WHO Expert Committee on Health Statistics. Sixth Report. WHO Technical Report Series, No. 164. Geneva: World Health Organization: 1959.
9. Lipton M, De Kadt E. Agriculture: Health linkages. Geneva: World Health Organization; 1988.
10. Prakash S, Manjunatha S, Shashikala C. Morbidity patterns among rice mill workers: A cross sectional study. Ind J Occup Environ Med 2010; 14(3): 91-3.
11. Saiyed HN, Tiwari RR. Occupational Health Research in India. Industrial Health 2004; 42: 141–8.
12. Leigh J, Macaskill P, Kuosma E, Mandryk J. Global burden of disease and injuries due to occupational factors. Epidemiol 1999; 10: 626-31.
13. Mohan D, Patel R. Design of safer agricultural equipment: Application of ergonomics and epidemiology. Int J Ind Ergonomics 1992; 10: 301-9.
14. Duggal R, Amin S. Cost of health care: A household level survey in an Indian district. Bombay: Foundation for Research in Community Health; 1989.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





