IJCRR - 4(24), December, 2012
Pages: 32-37
Print Article
Download XML Download PDF
MONTEGGIA FRACTURE-DISLOCATION TYPE 3 WITH POSTERIOR INTEROSSEOUS NERVE (PIN) INJURY: A CASE REPORT
Author: Ravish.V.N, Karthik Subramanian, I. Suresh
Category: Healthcare
Abstract:Fracture of proximal two-thirds of ulna and dislocation of the proximal radio-ulna joint in the same upper limb is called Monteggia fracture- dislocation. Four clinical variants of this fracture- dislocation have been described according to Bado's classification depending upon the fracture location and direction of dislocation of the radial head. Monteggia fracture-dislocation type 3 is a rare variety and its association with posterior interosseous nerve injury is not widely documented. We report the case of a 13 year old male who presented with one day old history of painful and swollen left elbow and weakness of his ipsilateral hand, following a self fall. On careful clinical examination and imaging (x-ray), he was diagnosed to have sustained Monteggia type 3 fracture-dislocation with posterior interosseous nerve (PIN) injury. After adequate pre-operative follow-up, the patient was treated by open reduction of the radial head, annular ligament reconstruction and open reduction, internal fixation of the fracture ulna with DCP and screws. The patient was followed up at regular intervals. His recent radiograph of the left forearm and elbow shows satisfactory union at the fracture site with complete recovery of the posterior interosseous nerve injury.
Keywords: Monteggia fracture-dislocation, Bado’s classification, Posterior interosseous nerve injury.
Full Text:
INTRODUCTION
The term Monteggia fracture- dislocation describes fracture of proximal two-thirds of ulna and dislocation of the proximal radio-ulna joint in the same upper limb1 . Four clinical variants of this fracture- dislocation have been described according to Bado’s classification depending upon the fracture location and direction of dislocation of the radial head2 . Monteggia type 3 fracture dislocation consists of fracture of proximal third ulna, just distal to coronoid process with lateral dislocation of the radial head. It is a rare variety of all Monteggia variants3 and its association with posterior interosseous nerve injury is not widely documented. We report the case of a 13 year old male who presented with post-traumatic painful left elbow due to Monteggia type 3 fracture-dislocation with posterior interosseous nerve (PIN) injury.
Case History
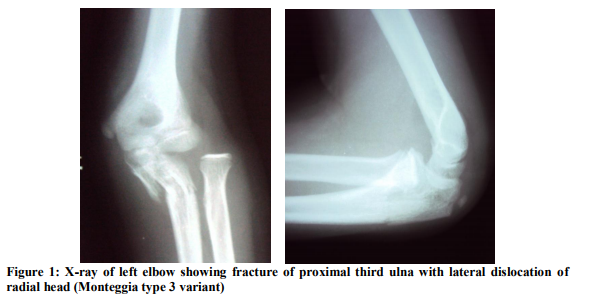
A 13 year old young male presented with complaints of severe pain and swelling in his left elbow following a fall on an out-stretched hand and inability to move his left elbow. The pain was acute in onset following the trauma, aggravated on movements on the affected limb, associated with diffuse swelling and deformity of the left elbow. On physical examination, there was tenderness over the radial head and proximal third of ulna. The radial head was palpable as a bony prominence on the lateral aspect of his elbow, in continuity with the shaft. There was crepitus, abnormal mobility and loss of transmitted movements in the proximal third shaft of left ulna. There was weakness of extensors of the thumb and four fingers of his left hand, but the power of dorsiflexion of his wrist was normal. Radial pulse of the ipsilateral upper limb was well felt. Conventional plain radiographs of his left elbow revealed fracture of the proximal third ulna just distal to the coronoid process and lateral dislocation of the radial head (Figure 1).
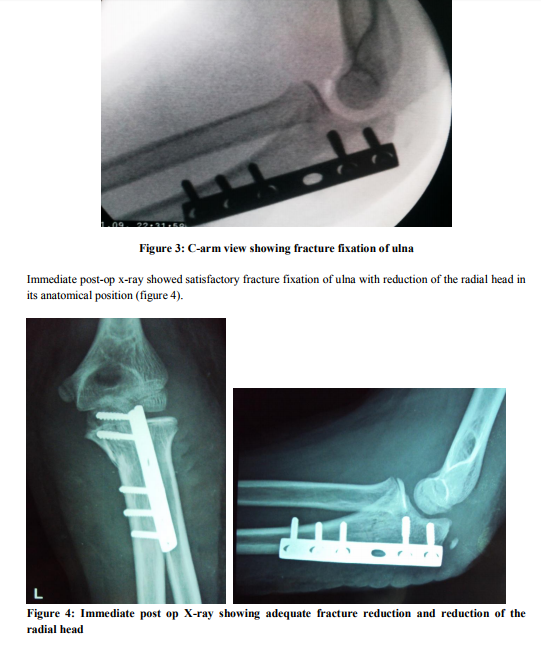
After adequate pre-operative workup, exploration of the left elbow was done using a Boyd’s approach3. The radial head was reduced and the annular ligament reconstructed using triceps tendon. The fracture of proximal third ulnar shaft was reduced and fixation was done with dynamic compression plate (DCP) and screws (figure 2 and figure 3).

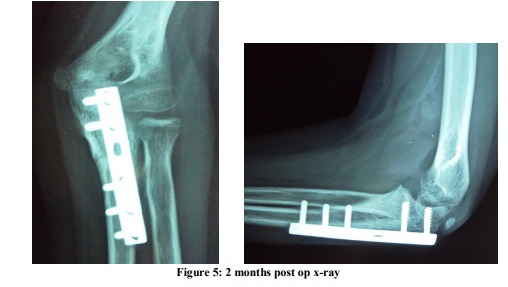
The patient recovered extension of his four fingers and thumb by six weeks after surgery. The movements of his right elbow were normal at a follow-up examination two months after surgery and radiographs showed satisfactory fracture union (figure 5).
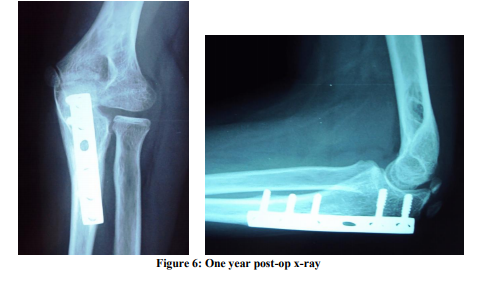
The patient was followed up at regular intervals thereafter. He showed normal range of movements at elbow, not associated with pain at the completion of one year and his recent radiograph showed complete union at the fracture site (Figure 6).
DISCUSSION
Fractures of the proximal two-thirds of ulna combined with dislocation of the proximal radio-ulnar joint were described in 1814 by Monteggia2 . Bado coined the term ‘Monteggia fracture-dislocation’ in 19672 . Numerous classification schemes have been developed, but Bado's classification has been widely accepted worldwide. Bado's classification2 divides Monteggia fracturedislocation into four types: Type 1 consisted of fracture in the proximal two thirds of the ulna with anterior dislocation of the radial head. This is the most common Monteggia injury in children, representing around 70%. Type 2 consisted of fracture in the proximal two thirds of the ulna with posterior dislocation of the radial head. This type is more commonly seen in elderly children and adults. Type 3 consisted of fracture of ulna, just distal to coronoid process at the metaphysis with lateral dislocation of the radial head. This fracture pattern often is associated with radial nerve or PIN injuries and a coexisting intra-articular obstruction to radial head reduction, which requires surgical reduction of the radial head. Type 4 consisted of fracture of the proximal or middle third of the ulna, anterior dislocation of the radial head, and fracture of the proximal third of the radius below the bicipital tuberosity. A hybrid lesion similar to a type III Monteggia lesion has been described in which anterior dislocation of the radial head was associated with a fracture of the metaphyseal region of the ulna that extended into the olecranon2 . Monteggia fracturedislocation type 3 is a rare variety, constituting only about 10-15% of all Monteggia variants3 . Stability of the proximal radioulnar joint is provided by the surrounding ligaments, primarily the annular ligament. The annular ligament maintains the position of the radial head within the radial notch of the ulna through the entire range of rotation, becoming tighter in supination because of the shape of the radial head. The substance of the annular ligament is reinforced by the radial collateral ligament at the elbow joint. Hence, annular ligament reconstruction forms an important step in maintaining the radial head reduction2 . The Monteggia lesion probably can be caused by any of the three proposed mechanisms, but the most common mechanism is a fall on an outstretched hand that forces the elbow into complete extension, locking the olecranon into the humerus2 . The biceps brachii muscle, inserting into the biceps tuberosity on the proximal radius, is a major deforming force. It is active in the pathomechanics of Monteggia fracture-dislocation, violently pulling the proximal radius away from the capitellum as the elbow goes into extension. During treatment, the effect of the biceps must be regulated by elbow flexion to prevent recurrence of the radial head dislocation2 . Nerve injuries in closed forearm fractures are relatively uncommon5 . There is a close relation between the posterior interosseous nerve and the proximal radius6 , with the nerve coursing anterior and anterolateral to the radial head and neck on its path through the supinator muscle. With anterolateral dislocations of the radial head, direct trauma may cause paresis of the nerve. In adults, there is a more discrete organization of the proximal border of the superficial head of the supinator, forming the ‘Arcade of Frohse’. This band is not as well defined in children, which may partially account for the lower incidence of permanent injury to the posterior interosseous nerve in children7 , as well as the high incidence of resolution once reduction of the radius is obtained2 . It is necessary to make an accurate diagnosis and render proper treatment by reduction and annular ligament reconstruction, when a Monteggia fracture-disloaction occurs, to avoid possible posterior interosseous nerve palsy due to excessive pronation and supination even several decades later4,8,9 .Internal fixation with plates allows excellent control of the fracture fragments and therefore permits accurate restoration of the anatomy, which remains the key principle in treating forearm fractures as it preserves maximal forearm function. In this case, immediate restoration of the elbow anatomy was done by reduction of the radial head with annular ligament reconstruction and fixation of fracture ulna with DCP and screws.
CONCLUSION
Fracture of proximal two-thirds of ulna and dislocation of the proximal radio-ulna joint in the same upper limb is called Monteggia fracture- dislocation. Four clinical variants of this fracture- dislocation have been described according to Bado’s classification depending upon the fracture location and direction of dislocation of the radial head. Monteggia fracture-dislocation type 3 is a rare variety, constituting only about 10-15% of all Monteggia variants and its association with posterior interosseous nerve (PIN) injuries is not widely documented. It is necessary to make an accurate diagnosis and render prompt treatment by reduction of the radial head dislocation and fixation of the ulna fracture to avoid PIN palsy. Regular follow-up till the recovery of PIN is essential.
CONSENT
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
COMPETING INTERESTS
The authors declare that they have no competing interests.
References:
1. Abdullahi Agaba-Idu Musa. Monteggia fracture-dislocation: a case report, its’ initial management and review of bado’s classification. Afr Health Sci. 2006; 6(4): 252–254.
2. Beaty JH, Kasser JR, editors. Rockwood and Wilkins Fractures in children. 7th edition. Philadelphia: Wolters Kluwer; 2012: 446- 475.
3. Canale ST, Beaty JH, editors. Campbell’s Operative Orthopaedics. 11th edition. Philadelphia: Mosby Elsevier; 2008; 3420- 24.
4. Cho CH, Lee KJ, Min BW. Tardy posterior interosseous nerve palsy resulting from residual dislocation of the radial head in a Monteggia fracture: a case report. Journal of Medical Case Reports 2009; 3:9300.
5. Spinner M, Freundlich BD, Teicher J. Posterior interosseous nerve palsy as a complication of Monteggia fractures in children. Clin Orthop Relat Res.1968; 58:141-145.
6. Jessing P. Monteggia lesions and their complicating nerve damage. Acta Orthop Scand. 1975; 46:601-609.
7. Stein F, Grabias SL, Deffer PA. Nerve injuries complicating Monteggia lesions. J Bone Joint Surg Am. 1971; 53:1432-1436.
8. Lichter RL, Jacobsen T. Tardy palsy of the posterior interosseous nerve with a Monteggia fracture. J Bone Joint Surg Am. 1975; 57:124-125.
9. Hashizume H, Nishida K, Yamamoto K, Hirooka T, Inoue H. Delayed posterior interosseous nerve palsy. J Hand Surg Br. 1995; 20:655-657.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





