IJCRR - 5(5), March, 2013
Pages: 162-165
Date of Publication: 22-Mar-2013
Print Article
Download XML Download PDF
ACUTE MYELOID LEUKEMIA PRESENTING AS PLEURAL EFFUSION: A UNIQUE EVENT
Author: Deepak Nayak M., Sushma V. Belurkar, Rachana Garg, Gauri A. Salgaonkar
Category: Healthcare
Abstract:Pleural involvement as one of first manifestations of a hematolymphoid malignancy is conventionally associated with solid tumors such as carcinomas of the breast, lung, gastrointestinal tract and lymphomas. A leukemic involvement of pleural effusion has seldom been described. We report a case of a 68 year old male who presented with a pleural leukemic infiltration. The patient complained of progressive exertional dyspnea for two weeks with cough and hemoptysis. The chest radiograph showed a bilateral pleural effusion. Diagnostic thoracocentesis suggested an exudate; with cytology remarkable for leukemic blasts comprising a total of 56%. The subsequent peripheral smear and bone marrow examination confirmed an acute myeloid leukemia (AML-M4). Chemotherapy was initiated but the patient succumbed shortly. This case is unique as it highlights the unusual presentation of the disease and also demonstrates the importance of analysis of material obtained in the body fluid.
Keywords: pleural effusion, acute myeloid leukemia, blasts.
Full Text:
INTRODUCTION
Acute Myeloid Leukemia (AML) is a group of hematogenous neoplasms characterized by a clonal proliferation of myeloid precursors with a reduced capacity to differentiate into more mature cellular elements.1 As a result, there is an accumulation of leukemic blasts or immature forms in the bone marrow with a spillover into the peripheral blood, and occasionally to other tissues. This is invariably associated with a variable reduction in the production of normal red blood cells, platelets and mature granulocytes. The increased production of malignant cells, along with a reduction in these mature elements, result in a variety of systemic consequences including anemia, bleeding, and an increased risk of infection.1,2 While the peripheral blood and bone marrow findings well elaborated in the literature, less than 1 percent of patients present with prominent extramedullary disease.1 These extramedullary manifestations can manifest simultaneously with, or precede the bone marrow involvement. Sites of isolated expression include bone, soft tissues, and lymph nodes, and less commonly the orbit, intestine, mediastinum, epidural region, uterus, and ovary.3 To the best of our knowledge, this is one of the few reported cases of pleural effusion as the initial manifestation of AML.
CASE REPORT
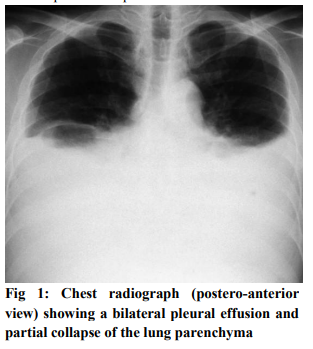
A 68 year old man was admitted to emergency unit of the hospital with a two-week history of progressive exertional dyspnea which had an acute exacerbation. He also had low grade fever, productive cough with hemoptysis and easy fatiguability. There was history of loss of appetite without any significant weight loss. Review of other systems was normal. On physical examination, the patient was alert but tachypneic even at rest. The cardiac examination was normal; pulmonary examination revealed diffusely decreased breathing sounds, inspiratory crackles and dullness to percussion with decreased vocal fremitus. There was no use of accessory muscles. The oxygen saturation was 84%. The systemic examination did not reveal lymphadenopathy. The ultrasound scan showed mild hepatomegaly. The chest radiograph showed a bilateral pleural effusion (figure 1). There was blunting of the costo- phrenic angle (CP).The lung parenchyma showed partial collapse.
A diagnostic and therapeutic thoracocentesis was performed which yielded approximately 1 litre of fluid. The respiratory symptoms resolved to a marginal extent and the fluid was sent to the laboratory for hematological and biochemical analysis. The thoracocentesis showed the following features (table 1).
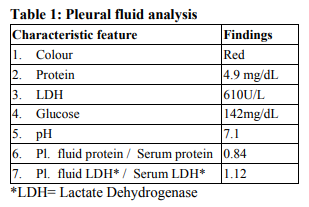
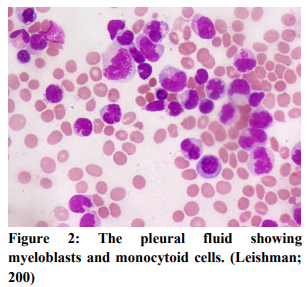
The pleural fluid analysis established that it was an exudative effusion. Ratio of the pleural fluid lactate dehydrogenase and protein to serum lactate dehydrogenase and protein (Light’s criteria) met the requisites for an exudative etiology.4 The total leucocyte count of the pleural fluid was 3200/ cu.mm. The differential count revealed 45% blast-like cells and 16% monocytoid cells (figure 2). The morphology of these cells revealed large sized monomorphic cells with round to slightly indented nuclei, fine chromatin, single conspicuous to multiple nucleoli and moderate amount of lightly basophilic cytoplasm The rest of the differential count was made up by lymphocytes and neutrophils. The background showed reactive mesothelial cells and hemorrhage. A provisional diagnosis of a lymphoma was considered. However, a correlation with the peripheral blood findings was awaited.
The hemogram showed an anemic profile (Hb: 7.2gm %) with mild leucocytosis (21,500 /mm3 ) and thrombocytopenia (platelets: 84,000 /mm3 ). The peripheral smear showed myeloblasts and monoblasts comprising a total of 57% of the differential leucocyte count. A diagnosis of acute leukemia was made and a bone marrow study was requested for subtyping of the neoplasia. The bone marrow established a diagnosis of acute myeloid leukaemia (AML M4- FAB classification). The cause of the pleural effusion was thus established. Induction chemotherapy was started, but the patient expired on the seventh day of treatment.
DISCUSSION
The diagnostic utility of pleural effusions are seldom reported or entertained. Rarely, can an effusion lead to the discovery of an underlying hematologic malignancy.1 Acute myeloid leukaemia (AML) generally presents with symptoms related to complications of leucocytosis or even pancytopenia. Most patients have more subtle evidence of bone marrow involvement for weeks, or perhaps months, before the diagnosis can be made.2 It is unusual for leukemias, either acute or chronic, manifest with malignant pleural effusions as the initial presentation.5-7 A malignant involvement of the body cavity leading to a fluid collection is a complication more commonly associated with solid tumors and lymphomas.7 Our patient presented with AML and pulmonary involvement with signs and symptoms secondary to the manifestations of pleural effusion itself. The classical appearance of the acute myeloid leukemia such as an association with organomegaly, or the complications such as bleeding and recurrent infections was overshadowed by the initial respiratory symptoms and signs. This mode of presentation also serves to demonstrate the importance of the hematological and biochemical analysis of the specimens obtained in pleural fluid since an early detection of any particular hematologic disease or malignancies specifically in this context, could guide effective therapy. Pleural effusions may be only initial presentation of a haematological malignancy or they may develop during the course of the disease. Besides the direct infiltration of leukaemic cells into the pleura, the pleural effusions can be secondarily caused by drug toxicity, underlying infections or by metastatic or rarely autoimmune causes in haematological malignancies.8 In most of the cases, the pleural fluid responds to the treatment of the primary disease, whereas the resistant or the relapsing cases may necessitate a pleurodesis.9 The other important aspect of diagnosing a malignant pleural effusion is that an extramedullary relapse is considered as recurrence of the leukaemia in sites other than the bone marrow.8 It is also known to recur ‘isolated’ without any recurrence in the bone marrow.7
CONCLUSION
Acute myeloid leukemia presenting as a pleural effusions are a rare occurrence. It indicates an advanced disease and a poor prognosis for the patient. The presence of abnormal cells in the effusion can simulate other common neoplasms such as a lymphoma or carcinoma. Cytologic examination continues to be an effective method to diagnose these. Ancillary techniques, when available, also help in this regard.
References:
1. ES, Harris NL, Stein H, Vardiman JW. World Health Organization of Tumors: Pathology and Genetics of Tumors of Hematopoietic and Lymphoid Tissues, Lyon 2001, France: IARC Press.
2. José Nieves-Nieves, et al. Pleural effusion as the initial extramedullary manifestation of acute myeloid leukemia. F1000 Research 2012; 1:39:1-6.
3. Dores GM, et al. Acute leukemia incidence and patient survival among children and adults in the United States. Blood 2012; 119(1): 34.
4. Light RW, et al. Pleural effusions: the diagnostic separation of transudates and exudates. Annals of Internal Medicine 1972: vol.77(4):507–513.
5. Byrd JC, et al. Extramedullary myeloid cell tumors in acute non-lymphocytic leukemia: a clinical review. J Clin Oncol.1995;13(7): 1800.
6. Ohe K, Okamura T, Arima F, et al. CD7+ Acute Myelogenous Leukemia exhibiting pleural involvement as an initial manifestation. Rinsho Ketsueki 1994; 35: 552–556.
7. Alexandrakis MG, Passam FH, Kyriakou DS, Bouros D. Pleural effusions in hematologic malignancies. Chest 2004; 125:1546-55.
8. Agrawal R. Acute myeloid leukaemia (AML) presenting as a bilateral pleural effusion. (Letter to the editor). JCDR 2013; Vol7(1):187.
9. Raina S, Kaul R, Mahesh DM, Kaushal SS, Gupta D, Sharma J. Pleural effusions in acute myeloid leukaemia. JAPI 2008; 56: 194.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





