IJCRR - 5(5), March, 2013
Pages: 150-153
Date of Publication: 22-Mar-2013
Print Article
Download XML Download PDF
SEROPREVALENCE OF HBs ANTIGEN AMONG CONTRACTUAL WORKMEN IN A SMALL-SCALE FACOR ALLOY FACTORY
Author: Supriya Panda, R. Sarath Babu, T.V. Ramani, K. Bhaskar Rao
Category: Healthcare
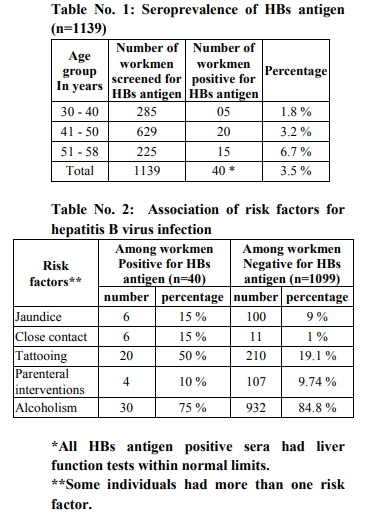
Abstract:Aim: To know the seroprevalence of HBs antigen among the contractual workers engaged in small-scale Facor Alloy Factory located in rural area. Materials and methods: Blood samples collected from 1139 contractual workmen were screened for HBs antigen by using two rapid tests in tandem. They were asked about the risk factors associated with hepatitis B virus infection. Results: Forty workmen (3.5%) were positive for HBs antigen. The prevalence rate was highest in 51-58 years of age (6.7%). Fifty percent of HBs antigen positive individuals gave past history of tattooing compared to 19.1 % of those negative for HBs antigen. Fifteen percent of HBs antigen positive individuals had close household contact with a patient suffering from jaundice compared to 1 % in HBs antigen negative individuals. Conclusion: Overall seroprevalence rate of HBs antigen in the study group was less compared to other studies from rural areas. Tattooing and close household contact were the most common risk factors for acquiring hepatitis B virus infection in the present study.
Keywords: Seroprevalence, HBs antigen, Rural area.
Full Text:
INTRODUCTION
Hepatitis B Virus infection is a global issue with more than 2 billion infected individuals throughout the world which includes more than 3 million chronically infected carriers (1). The prevalence of carrier rate varies in different countries in relation to their loving standard and life style. India belongs to intermediate endemic zone with carrier rate between 2-7%, with higher carrier rate in the southern part and lower rate in the northern part of the country (2). The prevalence of HBs Antigen in India varies from 1-13%, with an average of 4.7% (3-8). There are studies from India regarding its prevalence among blood donors (9), children (8) and in different tribal population (10-14). There are only few studies available based on its prevalence in rural population (15-16) and poor urban slums (17). Hence, the present study was undertaken to know the seroprevalence of HBs antigen among the contractual workers engaged in small-scale Facor Alloy Factory located in rural area.
MATERIAL AND METHODS
Study group: A total of 1,139 contract workmen of Facor Alloy Factory, located in Sriramnagar village of Garividi Mandal, 20 km away from MIMS, between 30 to 58 years old and not suffering from any acute illness were included in the study. They belong to low income group with low literacy rate. They were asked about previous episodes of jaundice and potential risk factors for acquiring hepatitis B virus infection, such as close house hold contact with a patient suffering from jaundice, tattooing, parenteral interventions like intravenous fluid, blood transfusion and intramuscular injection; and alcoholism. None of them had received hepatitis B virus vaccine. Duration of study: From October 2009 to December 2009.
Setting: The tests were carried out in the Dept. of Microbiology and Biochemistry, MIMS, after an approval taken from the head of the institution and owner of the factory. Written consent was taken from each individual included in the study to undergo the required tests. 5 ml venous blood was collected from each subject at the factory site and subjected to the tests on the same day in MIMS taking precaution to avoid cross contamination. Serology: Screening for HBs antigen was done by the test based on immunochromatography method (Hepacard, J.Mitra and Co Pvt. Ltd). Samples tested positive in first test were subjected to second test based on two-site sandwich immunoassay (Acon HBs Ag, Acon Biotech Co Ltd, China) (18). All the tests were performed in accordance with the manufacturers’ instructions with adequate controls. The specimens reactive for HBs antigen were subjected to liver function tests (LFTs) in the Dept. of Biochemistry. Workmen reactive for HBs antigen were counseled to consult an expert once in six months and health education was given to prevent its transmission.
RESULTS
Overall seroprevalence of HBs antigen among the study population was 3.5 %. The seroprevalence rate increased from third to sixth decades of life. Fifty percent of HBs antigen positive individuals gave past history of tattooing compared to 19.1 % of those negative for HBs antigen. Fifteen percent of HBs antigen positive individuals had close household contact with a patient suffering from jaundice compared to 1 % in HBs antigen negative individuals.
DISCUSSION
This is a cross-sectional study reporting seroprevalence of HBs antigen among contractual factory workmen of rural area with low literacy rate. Different studies from India and abroad reported a higher hepatitis B virus carrier rate among rural population with low income which varied from 12 % among rural Kenyans (19) to 5.3 % among rural West Bengal population (15). The overall seroprevalence of HBs antigen among South Indian population was reported to be 5.7 % (20). But in the present study, overall seroprevalence of HBs antigen was found to be 3.5 % which is low in comparison to other studies from India. In our study group, there is four folds increase in its prevalence from third to sixth decades of life. This suggests that although most of India’s hepatitis B virus carrier pool is established during early childhood as major spread of this infection in the community occurs at this age through vertical transmission and close contact with a patient or a carrier, other routes of transmission may also be important in its spread. Practices like use of shared razors, tattooing and ear piercing using unsterile instruments are more common in rural area and have been reported to transmit hepatitis B virus infection (21, 22, 23). In the present study tattooing and close household contact with hepatitis B virus were the most common risk factors for acquiring this infection. A study from South India also reported family contact with hepatitis B virus as the most significant risk factor (20).
CONCLUSION
The overall seroprevalence of HBs antigen among the study population was low with a four folds increase in its prevalence from third to sixth decade of life. Tattooing and close household contact were the most common risk factors.
ACKNOWLEDGEMENT
We acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors /editors /publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. WHO global health situation projection and estimates.1992; WHO Geneva.
2. R Ananthanrayana and CKJ Paniker. Text Book of Microbiology by R Ananthanrayana and CKJ Paniker.8th Edition, 2009.
3. Thyagarajan SP, Jayaram S, Mohanavalli B. Prevalence of HBV in general population of India. In: Sarin SK, Singhal AK, editors. Hepatitis B in India: Problems and prevention. New Delhi: CBS; 1996 p.5-16.
4. Jain RC, Bhatt SD, Sangle S. Prevalence of hepatitis surface antigen among rural population of Loni area in Ahmednagar district of Western Maharashtra. J Assoc. Physicians India 1992; 40:390-1.
5. Pal SR, Chitkara NL, Choudhury S, Dutta DV, Deodhar SD,Chhuttani PN. Hepatitis B virus infection in northern India. Prevalence, subtype and seasonal variation. Bull World Health Organ 1974; 51: 13-7.
6. Mital VN, Gupta OP, Nigam DK, Saxena PC,Kumar S. Pattern of hepatitis B antigencontact and carrier state in Northern India. J Indian Med Assoc 1980; 74:105-7.
7. Sobeslavsky O. Prevalence of markers of hepatitis B virus infection in various countries: aWHO collaborative study. Bull World Health Organ 1980; 58: 621-8.
8. Tandon BN, Irshad M, Raju M, Mathur GP, Rao MN. Prevalence of HBs Ag and antiHBs Ag in children and strategy suggested for immunisation in India. Indian J Med Res 1991; 93: 337-9.
9. S P Gulia, S Panda, E Sitaramam, K P Reddy. Seroprevalence of hepatitis B virus infection among blood donors in lacal population. The Internet J of Pathology. 2011; volume 12 Number 1.
10. Prasad SR, Rodrigues FM, Dhorje SP, Ramamoorthy CL. Prevalence and subtype of hepatitis B surface antigen in the tribal population of Arunachal Pradesh, India. Indian J Med Res 1983; 78: 300-6.
11. Dutta RN, Sen S. A study of Australia antigen, cold antibodies and ABO blood group frequencies in Ladakhies. Indian J Med Res 1975; 63: 1635-40.
12. Joshi SH, Gorakshakar AC, Mukherjee M, Rao VR, Sathe MS, Anabbaane SM. et al. Prevalence of HBs Ag carriers among some tribes of Madhya Pradesh.Indian J Med Res 1990; 91: 340-3.
13. Jain RC. Prevalence of HBs Ag among tribal population of Udaipur district in southern Rajasthan. Indian J Med Microbiol 1992; 10: 257-9.
14. Murhekar MV, Murhekar KM, Das D, Arankalle VA, Sehgal SC. Prevalence of hepatitis B infection among the primitive tribes of Andaman and Nicobar Islands. Indian J Med Res 2000; 111: 199-203.
15. Chowdhury A, Santra A, Chaudhuri S, Ghosh A,Banerjee P,Mazumder DN.Prevalence of hepatitis B infection in the general population: a rural community based study. Trop Gastroenterol 1999; 20: 75-7.
16. Singh H, Aggarwal R, Singh RL, Naik SR, Naik S. Frequency of infection by hepatitis B virus and its surface mutants in a northern Indian population. Indian J Gastroenterol 2003; 22: 132-7.
17. BN Tandon, Sk Acharya, A Tandon. Epidemiology of hepatitis B virus infection in India. Gut 1996; 38 (sppl 2): S56-S59.
18. Hepatitis B surface antigen assay: Operational characteristics (Phase 1). Report 2. Dept of Essential health technologies, WHO. Available at www.who.int/diagnostics_laboratory investgations.
19. Kew MC. Progress towards the comprehensive control of hepatitis B in Africa: a view from South Africa. Gut 1996; 38 (Suppl 2):S31-S36.
20. T Kurien, SP Thyagarajan, L Jeyaseelan, A Peedicayil, P Rajendran et al. Community prevalence of hepatitis B infection and modes of transmission in Tamil Nadu, India. Indian J Med Res 121, May 2005:670-675.
21. Limentani AE, Elliott LM, Noah ND, Lamborn JK. An outbreak of hepatitis B from tattooing. Lancet 1979; 2:86-8.
22. Johnson CJ, Anderson H, Spearman J, Madson J. Ear piercing and hepatitis. Non sterile instrument for ear piercing and subsequent onset of viral hepatitis. JAMA 1974; 227:1165.
23. Abdool Karim SS, Coovadia HM, Windsor IM, Thejpal R, van den Ende J, Fouche A. The prevalence and transmission of hepatitis B virus infection in urban, rural and institutionalized black children of Natal/KwaZulu, South Africa. Int J Epidemiol 1988; 17:168-73.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





