IJCRR - 5(5), March, 2013
Pages: 135-139
Date of Publication: 22-Mar-2013
Print Article
Download XML Download PDF
PREVALENCE OF DENTAL CARIES AT DIFFERENT LEVELS OF FLUORIDE ION CONCENTRATIONS AMONG THE SCHOOL CHILDREN IN NALGONDA DISTRICT
Author: Vikas C. Desai, Manjula M., Rajendra Reddy E., Hussain Saheb Shaik
Category: Healthcare
Abstract:Dental caries is the most common oral disease seen in children and adolescents. This study was conducted to assess prevalence of dental caries at different water fluoride levels in Nalgonda district of Andhra Pradesh. A total of 1800 school children aged 12-15 years were selected by stratified cluster sampling from three areas with different levels of natural fluoride concentrations in drinking water. Water samples were collected and analyzed for fluoride concentration. Dental caries was recorded using Dentition Status and Treatment Need index. The overall prevalence of dental caries in the study population was 35.2% and the remaining 64.8% of the children were caries free. The prevalence of caries in below optimal was the highest (57%) followed by above optimal fluoride areas (33.3%). The lowest prevalence of caries was found in the optimal fluoride areas (17.2%). The difference in the prevalence of dental caries between different fluoride areas was statistically significant. The prevalence of dental caries was more in below optimal fluoride area followed by areas where fluoride concentration was 5ppm and above. The lowest caries prevalence was found in optimal fluoride areas. There was a positive correlation between severity of dental fluorosis and prevalence of dental caries. There was a negative correlation between fluoride concentration and dental caries. The prevalence of dental caries decreased with increasing concentration of fluoride in the drinking water up to 5 ppm.
Keywords: Dental caries, Fluoride ion, Drinking Water.
Full Text:
INTRODUCTION
The prevalence of dental caries has decreased in the past two decades in developed countries. Contributing factors for this decline are water fluoridation, dentifrices, improved oral hygiene, changes in diet and awareness. However dental caries still exists as a smouldering disease in developing and under developed countries where there are inadequate resources of dental treatment, lack of public awareness and motivation1. The prevalence and severity of dental fluorosis varies from place to place depending mainly upon the fluoride concentration of the local drinking water. Dental fluorosis is a disorder effecting the mineralization of teeth as a result of exposure to excess amount of fluoride during tooth development. Although fluorosis is much more prevalent in high fluoride areas there is no evidence of an overall detrimental effect on caries susceptibility. According to the survey conducted by Rajiv Gandhi National Drinking Water Mission, fluorosis was prevalent in almost all districts of Andhra Pradesh, where Nalgonda district tops the list of fluorosis affected districts2 . Nalgonda district is one such endemic fluorosis area of Andhra Pradesh, where 1122 out of the 3321 habitations have fluoride levels of above 1 ppm in the drinking water. There are reports of not only dental fluorosis, but also crippling skeletal fluorosis from this region. Similar geographic and climatic conditions have been existing in this place but people are exposed to drinking water with different concentrations of fluoride, ranging from as low as 0.2 ppm to as high as 12 ppm3 . The correlation between dental caries and fluorosis has not been documented in this place so far. This makes Nalgonda an ideal place for the present study, to assess the prevalence of dental caries and dental fluorosis and their correlation at different concentrations of fluoride in drinking water. The aim of the study is to assess the relationship between drinking water fluoride levels and dental caries among 12 to 15 year old school children of Nalgonda district, Andhra Pradesh.
MATERIALS AND METHODS
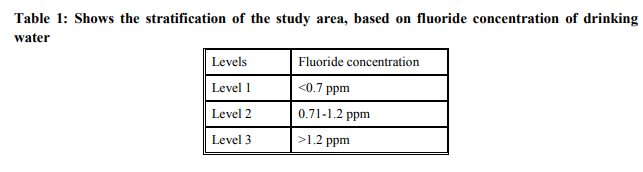
Source of Data: Total study population was 1800 school going children. Data was collected from 12-15year old school going children of Nalgonda district, who lived in the same place since their birth and who consumed drinking water from a single source, at least in the initial 12 years of their life. Study Design: This was a cross sectional Analytical study. Data was collected by means of structured questionnaires, intra oral examinations; and collection and analysis of drinking water samples (ground water) for fluoride concentrations. The questionnaire was used to collect information about their residential status, demographic details, eating, oral hygiene practices and exposure to fluoride. Clinical and visual examination was conducted to detect dental caries. A stratified random sampling technique was used. The entire geographical area of Nalgonda district was divided into 3 strata based on the concentrations of naturally occurring fluoride in drinking water. Sample size was equally divided among the three strata. Schools were selected randomly from each stratum. From each selected school, all the children who satisfied the inclusion criteria were considered, till the required numbers of children were selected. Information on drinking water fluoride levels was obtained from the documented records of the office of the Chief Engineer, Department of Rural Water Supply (RWS), Nalgonda. Criteria followed for diagnosis of dental caries and dental fluorosis: The criteria suggested by World Health Organization (WHO) in 1997 were followed to diagnose the carious lesions. Dental caries was recorded using “Dentition status and treatment need index”4 . The information collected from questionnaires, clinical examinations and Fluoride analysis was computerized and analyzed using the Statistical Package for Social Sciences (SPSS version 16.0).
RESULTS
This cross sectional study was conducted on a total of 1800 school children in the age group of 12 – 15 years. The number of children in 12 years, 13 years, 14years and 15 years was 444, 446, 425 and 485 respectively. The study had 1102 male and 698 female children. There was no statistically significant difference in the age distribution of the study population across the gender groups. Among 1800 school children, 560 were from below optimal fluoride areas. The corresponding number of children from optimal and above optimal fluoride areas was 612 and 628 respectively. There was no statistically significant difference in the distribution of children in different fluoride areas. Prevalence of Dental caries: The overall prevalence of dental caries in the study population was 35.2% and the remaining 64.8% of the children were caries free. The prevalence of caries in below optimal was the highest (57%) followed by above optimal fluoride areas (33.3%). The lowest prevalence of caries was found in the optimal fluoride areas (17.2%). The difference in the prevalence of dental caries between different fluoride areas was statistically significant (p=0.000). Prevalence of dental caries between males and females: The prevalence of dental caries among males in the study was 34.85% and among females it was 35.67%. There was no statistically significant difference in the distribution of dental caries between male and female children in the present study (p=0.720). Prevalence of dental caries in different age groups: The prevalence of dental caries among 12 years group was 35.36%. The corresponding values among 13, 14, and 15 years groups were 35.65%, 35.06%, and 34.64% respectively. There was no statistically significant difference in the distribution of dental caries in different age groups (p=0.990). Distribution of DMF component among the study population in different fluoride areas: The mean DMFT in the study population was 0.59 with a standard deviation of 1.01. The mean DMFT score was highest in the below optimal fluoride area (1.17±1.42) followed by above optimal fluoride area (0.43±0.67) and optimal fluoride area (0.21±0.50) in the descending order. The difference in the mean DMFT score among the study population in different fluoride areas was statistically significant (p=0.000). The finding was true even when the comparison was made among different age groups in different fluoride areas.
DISCUSSION
The effect of drinking water fluoride concentration on human health, particularly dental health has been a matter of debate since the works of McKay and Dean. Dean’s landmark epidemiologic studies had conceptualized that 1 ppm of fluoride in drinking is ‘optimum’ for dental health, which offers maximum protection against dental caries, with minimal or no dental fluorosis5 . Galagon designed a formula (E= - 0.038+0.0062 X temperature in F0 . where E is estimated water intake) for optimal concentration of fluoride in drinking water, based on mean annual temperature of the area6,7 . Nalgonda district is a known endemic area for fluorosis, with a wide spectrum of severity, ranging from mild dental fluorosis to crippling skeletal fluorosis8 . The study was intended to find the prevalence of dental caries and dental fluorosis in relation to fluoride ion concentration in drinking water. Commonly, all the deciduous teeth are exfoliated and all the permanent teeth, except third molars are erupted by 12 years of age9,10. The study population contained about 61.2% of boys and 38.8% of girls. Socio-economic status of the individuals is known to influence dental caries11 . Sample size was 1800 and the samples were almost equally selected from the three areas with different water fluoride levels. To record dental caries, Dentition status and Treatment Need Index5 was used. Caries diagnosis was based on the guidelines given by WHO in 1997 for assessment of dental caries. The average prevalence of dental caries in the present study was 35.2%, lower than average Andhra Pradesh caries prevalence of 41.5% for 15 year age group, as reported by National Oral Health Survey and Fluoride Mapping- 2002- 200312. In the present study 67.06% of the children had dental fluorosis. National oral health survey and fluoride mapping by Dental council of India (2002 -03) found the prevalence of dental fluorosis in the state of Andhra Pradesh to be around 5% which was significantly less12 . The least prevalence of dental caries was found in level 2 (0.71 –1.2 ppm). Many studies concluded that dental caries and fluorosis are minimum at about 1ppm water fluoride concentration13,14. . Menon A, Indushekar. K. R (1999)15 in their study among 6-16 year old school children in Gadag and Dharwad district of Karnataka, India and reported the prevalence of dental caries to be 33% and the DMFT to be 0.65 in low fluoride area (below optimal fluoride area with a fluoride concentration of 0.5 ppm) and the prevalence of caries in high fluoride area (optimal fluoride area with a fluoride concentration of 1.2 ppm) was 16% and the mean DMFT was 0.39. The caries experience was more in below optimal fluoride area than in optimal fluoride area. The results of the present study were consistent with the findings of this study. V.V.Subba Reddy & A.Tiwari (1992)16 in their study among 1750 school children in the age group 12 – 17 years, on the prevalence of dental caries in relation to fluoride levels of drinking water, in Punjab, India found the prevalence to be lowest in areas where the fluoride concentration was 1.1 ppm (dental caries prevalence was 61.24%) and 2 ppm (dental caries prevalence was 54.72%). The dental caries prevalence was relatively high in areas where the fluoride concentration was 0.3 ppm (89.03%), 3.4 ppm (72.77%), 5.4 ppm (73.61%) and 10.4 ppm (85.47%). The caries experience was more in below optimal and above optimal fluoride areas than compared to optimal fluoride areas. The results of the present study were in harmony with the conclusions of this study. A 1995 investigation by The National Committee on Oral Health of China (NCOH)17 showed the relationship between average number of decayed, missing and filled teeth (DMFT) of urban residents and fluoride concentration in drinking water to be negatively correlated but not forming a good linear relationship. A study conducted in China (2005)18 reported that there was a statistically significant reduction in dental caries as the fluoride content of the drinking water increased from 0.4 to 5.6 ppm. The present study is in accordance with the above study in concluding that there was significant reduction in caries prevalence from 0.7 – 5.3ppm. In the present study the prevalence of dental caries (57%) and mean DMFT (1.17± 1.42) was found to be the highest in below optimal fluoride area and least in optimal fluoride area (17.2% and 0.21± 0.50). The caries experience in the above optimal fluoride area was intermediate (33.3% and 0.43±0.67). The present study found an overall weak negative correlation between concentration of fluoride in drinking water and caries experience.
CONCLUSION
There was a strong positive relationship between fluoride concentration in drinking water and the prevalence and severity of dental fluorosis. The prevalence of dental caries was more in below optimal fluoride area followed by areas where fluoride concentration was 5ppm and above. The lowest caries prevalence was found in optimal fluoride areas. There was a negative correlation between fluoride concentration and dental caries. The prevalence of dental caries decreased with increasing concentration of fluoride in the drinking water up to 5 ppm.
References:
1. Kulkarni S.S, Deshpande S.D. Caries prevalence and treatment needs in 11-15 year old children of Belgaum city. J Indian Soc Pedo Prev Dent 2002; 20(1):12-5.
2. Prevention and control of fluorosis. Health aspects volume I. Rajiv Gandhi National Drinking water Mission. New Delhi, 1993.
3. http://nalgonda.ap.nic.in/climate_rainfall.htm .01/12/2012.
4. World Health Organization. Oral health surveys, Basic methods, 4th edition. Geneva: WHO, 1997.
5. Dean HT. Endemic fluorosis and its relation to dental caries. Public Health Rep 1938;53:1443 52.
6. E. S. Budipramana, A. Hapsoro, E. S. Irmavati, S. Kuntari. Dental fluorosis and caries prevalence in the fluorosis endemic area of Assemblages, Indonesia. International Journal of Paediatric Dentistry 2002; 12:415- 22.
7. A.K. Susheela. Epidemiology and control of fluorosis in India, J of Nutrition foundation of India, April 1984.
8. KM Sudhir, GM Prashant, VV Subba Reddy, U Mohandas, GN Chandu Prevalence and severity of dental fluorosis among 13- to 15- year-old school children of an area known for endemic fluorosis: Nalgonda district of Andhra Pradesh. J Indian Soc Pedo Prev Dent 2009:27(4):190-196.
9. Ralph E. McDonald. Dentistry for child and adolescent, 8th edition, Mosby publications, 2004.
10. Sathananthan K, Vos T, Bango G. Dental caries, fluoride levels and oral hygiene practices of school children in Matebeleland South, Zimbabwe. Community Dent Oral Epidemiol 1996; 24:21-4.
11. Akpata ES, Akinremisi EO. Anti bacterial activity of extracts from some African chewing sticks. Oral Surg 1977; 44:717-22.
12. National oral health survey and fluoride mapping 2002-2003, India. Dental Council of India, New Delhi, 2004.
13. Manji F. Gingivitis, dental fluorosis and dental caries in primary school children in Nairobi, Kanya; E.Afr Med. J 1984;61:524- 32.
14. Grobler SR, Louw AJ, van Kotze TJ. Dental fluorosis and caries experience in relation to three different drinking water fluoride levels in South Africa. Int J Paediatric Dent 2001; 11:372 9.
15. Menon A, Indushekar K.R. Prevalence of dental caries and co-relation with fluorosis in low and high fluoride areas. J Indian Soc Pedo Prev Dent Mar 1999.
16. V V Subba Reddy and A. Tewari. Prevalence of dental caries to different levels of fluoride in drinking water. JIDA 1992;63(11):455-9.
17. Wang B, Zheng B, Zhai C, Yu G, Liu X. Relationship between fluorine in drinking water and dental health of residents in some large cities in China. Environ Int. 2004; 30(8):1067-73.
18. Jian-Ping Ruan, Zhuang-Qun Yang, Zhi-Lun Wang, Anne Nordrehaug Astrom, Asgeir Bardsen and Kjell Bjorvatn. Dental fluorosis and dental caries in permanent teeth: rural school children in high fluoride areas in the shaanxi province, China. Acta Odontologica Scandanavica 2005;63(5):258-65.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





