IJCRR - 5(6), March, 2013
Pages: 114-118
Date of Publication: 30-Mar-2013
Print Article
Download XML Download PDF
EFFICACY OF FINE NEEDLE ASPIRATION CYTOLOGY IN EVALUATION OF BREAST LUMPS: A ONE YEAR STUDY
Author: Sumit Giri
Category: Healthcare
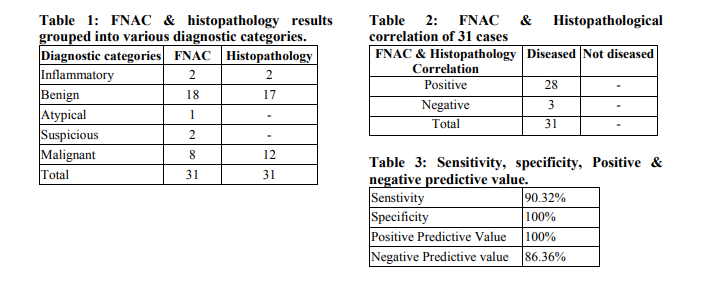
Abstract:Background: Lumps in breast have always commanded a great deal of attention because of fear of their being cancerous. Preoperative diagnosis helps in planning the correct surgical and therapeutic treatment. Aim: This study was aimed to assess the efficacy of Fine Needle Aspiration Cytology (FNAC) in breast lump evaluation with regards to sensitivity, specificity, positive predictive value and negative predictive value. Materials and Methods: This study was carried out on 277 breast lump cases at the Department of pathology, Dr. Hedgewar Arogya Sansthan Hospital from July 2009 to July 2010. FNAC was performed by cytopathologist with a 21 or 22G needle that was attached to a 10cc syringe. Two slides were stained with May Gr\?nwald-Giemsa (MGG) and 2 with Papanicolaou (Pap) stain. FNAC results were compared with final histopathological diagnosis. Taking histopathology as gold standard criteria, sensitivity, specificity, positive predictive value and negative predictive value of FNAC for detection of various lesions were calculated. Results: A total of 277 cases of FNAC of breast Lumps were obtained, out of which histopathological correlation was available in only 31 (11.19%) cases. Out of 12 histopathologically confirmed malignant cases, 8 cases were diagnosed as malignant on FNAC, two cases as suspicious for malignancy, one case as atypical hyperplasia and one as benign mammary lesion. There was not even a single case which was diagnosed as malignant on FNAC and later turned out to be benign on histopathology. Out of 31 cases where histopathology was available, in 28 cases the FNAC diagnoses correlated well with the final histopathological diagnosis. In the remaining 3 cases, one was diagnosed as benign mammary lesion and others as atypical hyperplasia on FNAC. On histopathological examination all 3 showed infiltrating ductal carcinoma. The Sensitivity, Specificity, Positive predictive value and Negative predictive value of FNAC were found to be 90.32%, 100%, 100% and 86.36% respectively. Conclusion: FNAC is a quick, inexpensive, simple, safe and readily acceptable procedure to patient and can be performed in Out Patient Department. It helps in providing a speedy and accurate diagnosis of not only breast cancers but also the majority of benign lesions mimicking malignancy.
Keywords: Breast lump, FNAC, sensitivity, specificity.
Full Text:
INTRODUCTION
Breast lumps in women encompasses a spectrum of benign and malignant disorders. Benign proliferative breast disease is an extremely complex and interrelated group of proliferative disorder of the breast parenchyma, most of which are not true neoplasm but are hormonally induced hyperplastic processes. Breast cancer is the most common type of cancer in women, in the age group of 40 – 50 years. It is the second leading cause of cancer deaths i.e about 250,000 women die of this disease every year [1]. Increase in cases of breast cancers are related to late marriage, birth of child in the later age, shorter period of breast feeding and nulliparity or low parity. Though histopathological diagnosis is a universally accepted confirmatory mode of diagnosis & follow up, fine needle aspiration cytology (FNAC) of breast lumps is an important part of triple assessment (clinical examination, imaging, and FNAC) of palpable breast lumps. Fine needle aspiration cytology (FNAC) is a relevant and important diagnostic method in the management of breast cancer. It has high sensitivity and specificity in determining the pathology of breast lumps [2,3,4,5, 6]. This study was aimed to assess the efficacy of FNAC in breast lump evaluation with regards to sensitivity, specificity, positive predictive value and negative predictive value.
MATERIALS AND METHODS
This retrospective study was carried out at the Department of pathology, Dr. Hedgewar Arogya Sansthan Hospital from July 2009 to July 2010. FNAC was performed on 277 cases by cytopathologist with a 21 or 22G needle that was attached to a 10cc syringe. The skin over the lump was completely cleaned with antiseptic solution. The palpable lesion was immobilized and the needle inserted into the lesion. Multidirectional sampling was done by to and fro movement of the needle. Negative pressure was applied during this time and released prior to removing the needle. At least 3 passes were made. The needle was taken out as some fluid /blood appeared in the hub. The sample obtained was pushed onto a glass slide and smeared. At least 4 slides were prepared. 2 slides were airdried and 2 were fixed with 95% alcohol. These air-dried slides were stained with May GrünwaldGiemsa stain, while the alcohol-fixed slides were stained with Papanicolaou stain in the cytopathology laboratory. Unsatisfactory slides were excluded from the study. Except for mild pain reported by some patients, no other complications were recorded. Pre-operative FNAC results were compared with final histopathological diagnosis in 31 patients. Taking histopathology as gold standard criteria, sensitivity, specificity, positive predictive value and negative predictive value of FNAC for detection of various lesions were calculated. The sensitivity of a test is the ability of a test to identify correctly all those who have the disease (True positive/True positive + False negative). The specificity of a test is the ability of the study to identify correctly the candidates who do not have the disease. (True negative /True negative +False positive). The positive predictive value of a test indicates the probability that the patient with a positive test has, in fact, the disease in question (True Positive / True Positive + False Positive). The negative predictive value of a test indicates the probability of a patient with a negative test not having the disease in question (True negative / True negative + False negative ). Formula used for detection of sensitivity, specificity, positive predictive value and negative predictive value was as follows: Sensitivity = (True positive / True positive + False negative) x100 Specificity = (True negative / True negative + False positive) x100 Positive predictive value = (True Positive / True Positive + False Positive) x100 Negative predictive value= (True negative / True negative + False negative) x100
RESULTS
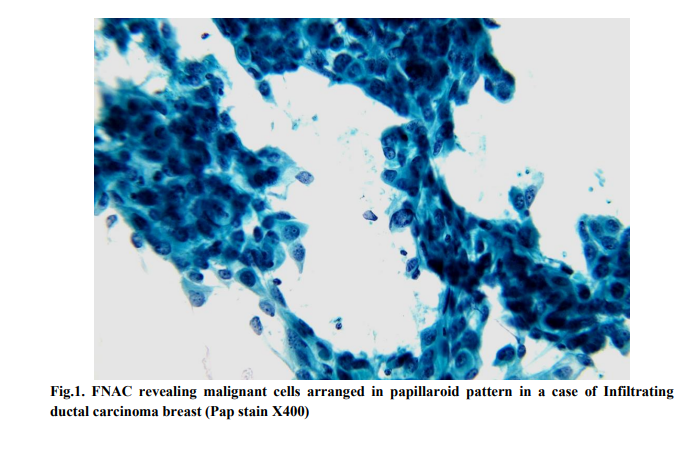
A total of 277 cases of FNAC of breast Lumps were obtained, out of which histopathological correlation was available in only 31 (11.19%) cases. FNAC and histopathology results were grouped into five diagnostic categories (Table 1). Out of 12 histopathologically confirmed malignant cases, 8 cases were diagnosed as malignant on FNAC, two cases as suspicious for malignancy, one case as atypical hyperplasia and one as benign mammary lesion. There was not even a single case which was diagnosed as malignant on FNAC and later turned out to be benign on histopathology. Out of 31 cases where histopathology was available, in 28 cases the FNAC diagnoses correlated well with the final histopathological diagnosis (Table 2). In the remaining 3 cases, one was diagnosed as benign mammary lesion and others as atypical hyperplasia on FNAC. On histopathological examination all 3 showed infiltrating ductal carcinoma (Fig.1). In our study 28 cases were true positive, 3 were false negative and no false positive. Since female without any breast lump was not included in this study, we had no true negatives or female with normal breasts. So we calculated 19 cases (17 benign and 2 inflammatory on histopathology) as true negatives which were also diagnosed as benign and inflammatory lesions on FNAC. The Sensitivity, Specificity, Positive predictive value and Negative predictive value of FNAC is shown in Table 3.
DISCUSSION
Breast lump have always commanded a great deal of attention because of fear of their being cancerous. Most of breast disease takes the form of palpable lump, sometimes painful and most of these conditions have possible confusion clinically with cancer [7]. Women breast lump are in a state of anxiety. Hence a quick diagnosis of lump in the breast is essential. FNAC of breast lump is an accepted and established method to determine the nature of breast lump with high degree of accuracy [8,9,10,11]. This study was aimed to assess the efficacy of FNAC in breast lump evaluation with regards to sensitivity, specificity, positive predictive value and negative predictive value. Our study revealed the sensitivity of 90.32% and specificity of 100% which were in accordance to sensitivity of 77- 99% and specificity of 92-100% reported in various studies[12-18]. In the present study, cases suspicious for malignancy and with atypical hyperplasia were found to be infiltrating ductal carcinoma following biopsy. This emphasizes need for further evaluation of such lesions, which often prove to be malignant [17]. This study also documented the fact that the benign lesions of breast are the most common lesions. This increased case of benign lesions indicates increase in awareness of patients. In such lesions the reassurance is the main line of treatment though close follow up is mandatory.
CONCLUSION
It is concluded that FNAC is an ideal adjunct tool in cancer program and management of patients presenting with breast lump as it helps in early diagnosis. It is a rapid, relatively atraumatic and accurate method for the diagnosis of breast lumps. It is highly accurate and has low false positive and false negative diagnosis. It can be carried out safely as a preoperative diagnostic method in patients with breast lump, mostly in outpatient department. Mastectomies can be prevented by early diagnosis and open biopsies need can be reduced. So it is recommended that FNAC should be used as a routine diagnostic method to maximise availability of health care to patients with breast lesions.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Fatima S, Faridi N, Gill S. Breast Cancer: Steroid Re-ceptors Prognostic and other Prognostic Indicators. JCPSP 2005; 15 (4): 230 – 233.
2. Furnival CM, Hocking MA, Hughes HE, Reid MM, Blumgart LH (1975). Aspiration cytology in breast cancer. Its relevance to diagnosis. Lancet, 2, 446-9.
3. Nicosia SV, Williams JA, Horowitz SA, et al (1993). Fine needle aspiration biopsy of palpable breast lesions. Review and statistical analysis of 1875 cases. Surg Oncol, 2, 145- 60.
4. Ballo MS, Sneige N (1996). Can core needle biopsy replace fine-needle aspiration cytology in the diagnosis of palpable breast carcinoma. A comparative study of 124 women.Cancer, 78, 773-7.
5. Yeoh GP, Chan KW (1998). Fine needle aspiration of breast masses: an analysis of 1,533 cases in private practice. Hong Kong Med J, 4, 283-8.
6. Chaiwun B, Settakorn J, Ya-In C, et al (2002). Effectiveness of fine-needle aspiration cytology of breast: analysis of 2,375 cases from northern Thailand. Diagn Cytopathol, 26, 201-5.
7. Mushtaque S, Memon N, Karamat KA. Breast cancer in Pakistani women. Pak JPathol 1998; 9 (2); 1-3.
8. Purasiri P, Abdalla M, Heys SD, Ah-See AK, McKean ME, Gilbert FJ, Needham G, Deans HEand Eremin O. A novel diagnostic index for use in the breast clinic. J R Coll Surg Edinb 1996; 41: 30-4.
9. Kaufman Z, Shpitz B, Shapiro M, Rona R, Lew S, Dinbar A. Triple approach in the diagnosis of dominant breast masses: combined physical examination, mammography and fine-needle aspiration. J Surg Oncol 1994; 56: 254-7.
10. Dehn TCB, Clarke J, Dixon JM, Crucioli V, Greenall MJ, Lee ECG. Fine needle aspiration cytology, with immediate reporting in the outpatient diagnosis of breast disease. Ann R Coll Surg Engl 1987; 69: 280-2.
11. Dixon MJ, Anderson TJ, Lamb J, Forest AMP. Fine needle aspiration cytology, in relationships to clinical examination and mammography in the diagnosis of a solid breast mass. Br J Surg 1984; 71: 593-6.
12. Hussain MT. Comparison of fine needle aspiration cytology with excision biopsy of breast lump. J Coll Physicians Surg Pak 2005; 15(4): 211-214.
13. Jayaram G, Alhady SF, Yip CH. Cytological analysis of breast lesions: A review of 780 cases. Malaysian Journal of Pathology 1996; 18: 81-87.
14. Muhamed AZ, Edino ST, Ochicha O, Alhasan Su. The Value of Fine-needle aspiration biopsy in preoperative diagnosis of palpable breast lumps in resource-poor countries: a Nigerian experience. Annals of African Medicine 2005; 4: 19-22.
15. Rubin J, Horiuchi K, Joy N, Haun W, Read R, Ratzer E, Fenoglio M. Use of FNAC for solid breast lesions is accurate and cost effective. Am J Surg 1997; 174: 694-6.
16. Ishikawa T, Hamaguchi Y, Tanabe M, Momiyama N, Chishima J, Nakatini Y, Nozawa A, Sasaki T, Kltamura H, Shimada H. False positive and false negative cases of fine needle aspiration cytology for breast lesions. Breast Carcinoma 2007; 14: 388-92.
17. Argia R, Bloom K, Reddy VB, Klusens L, Francescotti D, Dowlat K, Sizipikou P, Gattuso P. Fine Needle Aspiration of clinically suspicious palpable breast masses with histopathological correlation. Am J Surg 2002; 184: 410-413.
18. Choi YD, Choi YH, Lee JH, Nam JH, Juhng SW, Choi C, Acta Cytol. 2004; 48: 801-806.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





