IJCRR - 5(6), March, 2013
Pages: 80-86
Date of Publication: 30-Mar-2013
Print Article
Download XML Download PDF
STERNAL FORAMEN - A CASE REPORT
Author: Parvathi S.
Category: Healthcare
Abstract:The sternum or Breastbone is one of the flat axial bone forming the anterior part of thoracic skeleton. It resembles a short sword. The upper part is the manubrium, middle part is the body The lowest partappears the point of the sword is xiphoid process or xiphisternum. The length of adult sternum in an averagely build individual is about 17.2cm, which is longer in males that females. The foramen was found in one sternum during routine osteological class taken for 1st MBBS students in academic year-2011-12 in anatomy department. Student by name Krupa.K. JJMMC Davangere Karnataka State come and showed this bone. One oval shaped foramen of size 0.5cmX0.7cm was present on lower 1/3 of body of an adult sternum such a foramen of sternum is not common. This has been not only a focus of attention of anatomists but also at interest of Forensic experts, orthopedicians, paediatricians, cardiothoracic surgeons, physicians because it is very close contact with heart and lungs.
Full Text:
INTRODUCTION
The sternum or Breast bone is one of the flat axial bone forming the anterior part of thoracic skeleton. It resembles a short sword. The upper part is the manubrium, middle part is the body The lowest part appears the point of the sword is xiphoid process or xiphisternum. The length of adult sternum in an averagely build individual is about 17.2 cm, which is longer in males that females.
AIM:
Sternal along with ribs, vertebral variations described in the literature. The purpose of this study was to review and discuss and to highlight the importance of early recognition of these defects. These lesions are frequently overlooked at the initial evaluation 5 .
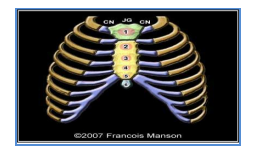
NORMAL ANATOMY OF STERNUM: The STERNUM
(from Greek sternon, "chest"; plural "sternums" or "sterna") or breastbone is a long flat bony plate shaped like a capital "T" located anteriorly to the heart in the center of the anterior wall of the thorax (chest). Thus the sternum plays an important role in protecting helps to protect the lungs, heart and major blood vessels from physical trauma. Its average length in the adult is about 17 cm, and is rather longer in the male than in the female. From the front, the sternum is shaped somewhat like a sword\dagger. From the side, the sternum appears as a long, flat bone with a outward curvature. The sternum consists of 3 parts: listed superior to inferior: the manubrium, the body of sternum or gladiolus, and the xiphoid process. The Manubrium (ma-NOO-bree-um) is the broad superior portion of the sternum, connects to the 1st pair of ribs. The superior end supports the clavicles (collarbones), and its margins articulate with the cartilages of the first seven pairs of ribs forming the front of the rib cage. The Body or Corpus Sterni or Gladiolus is the longest part of the sternum connects with the next 6 pairs of ribs. Together, these 7 pairs of ribs are known as the true ribs. The sternal angle is located at the point where the body joins the manubrium. The sternal angle is a useful landmark when counting ribs because the second rib attaches here. In early life its body is divided in four segments, called sternebrœ (singular: sternebra)
The Xiphoid Process or Processus Xiphoidus or Ensiform Appendix or Xiphoid Appendix --Located at the inferior end of the sternum is the pointed is the smallest of the three pieces. It articulates above with the body and on the front of each superior angle presents a facet for part of the cartilage of the 7th, 8th, 9th and 10th ribs. it gives attachment to the linea alba and, on the posterior surface, to the diaphragm9 .
OBSERVATIONS
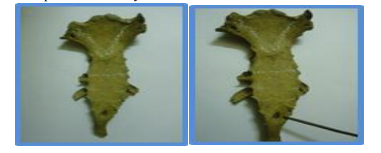
During the examination of the skeleton an oval defect was found through the Xiphoid Process of the sternum. It was located in the center of the midline of the between the attachments of the 6th and 7th costal cartilages and measured of size 0.5cm X 0.7cm. The edges were smooth, well ossified rounded, and covered by cortical bone.
MATERIALS AND METHODS
The foramen was found in one sternum during routine osteological class taken for 1st MBBS students in academic year-2011-12 in anatomy department. Student by name Krupa. K. JJMMC Davangere Karnataka State come and showed this bone. One oval shaped foramen was present on lower 1/3 of body of an adult sternum such an foramen of sternum is not common. This have been not only a focus of attention of anatomists but also at interest of Forensic experts, orthopedicians, paediatricians, cardiothoracic surgeons, physicians because it is very close contact with heart and lungs.
DISCUSSION
In the fetus the sternum originally consists of two cartilaginous bars, one on either side of the midline, which become connected to the cartilages of the upper 9ribs on each side
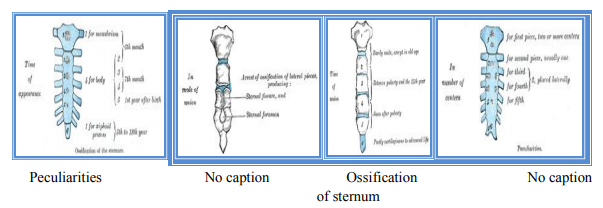
These two bars fuse with each other along the middle line to form the cartilaginous sternum which is ossified from six centers in the following order: one for the manubrium and four for the body first piece of the body, during the sixth month; in the second and third pieces of the body, during the seventh month of fetal life; in its fourth piece, during the first year after birth; and one for the xiphoid process, between the fifth and eighteenth years. one for the manubrium, four for the body, and xiphoid process. During the 8th week of gestation these bars migrate, converge toward the midline, and fuse with each other, beginning cephalically. By the 9 week the union of the plates is established in the midline and fusion is almost completed to form the manubrium and body of the sternum. The xyphoid process is formed by a caudal extension of the sternal plate.These ossification centers appear between the articular depressions for the costal cartilages and divide the sternal plate into 6 transverse pieces. The 3rd, 4th, and 5th pieces are often formed from multicentric ossification centers placed laterally. The 3rd and 4 th appear during the 4th and 5th months of fetal life. The 5th usually appears one year after birth. Incomplete fusion of the sternal bars in this area accompanied by eccentric centers of ossification accounts for the relatively rare occurrence of a perforate sternum (sternal foramen), or of a vertical fissure which intersects this part of the bone and which is referred to as fissura sterni. Ossification of the sixth part in the xyphoid process; does not begin until the 5thto 18th year of life and partial cartilaginization may persist well into adult life. Thus, malformations of the xyphoid process due to abnormal fusion and irregular ossification are much more common. Abnormalities of the manubrium and upper portion of the body of the sternum where fusion and ossification occur early in fetal development are much more rare. The position of these defects, in the center of the lower portion of the body of the sterum between the articular surfaces of the costal cartilages, and their characteristic gross appearance are consistent with sternal foramina. Developmental defects of the sternum are usually not readily detected in vivo or in the intact body during postmortem examination, unless they are associated with severe malformations of the rib cage. Perforations or fissures are obscured on routine chest X-rays by the radio-dense structures of the mediastinum and by the superimposed thoracic vertebral column. Abnormalities can be demonstrated at autopsy by holding the removed breastplate between the prosector and a strong light source. If a defect is detected by transillumination, it can be documented by further dissection and by Xraying the breastplate alone. The differentiation between traumatic and congenital defects of the sternum does not present a difficult problem in bodies that are not decomposed. Associated abnormalities, either old or recent, in the surrounding soft tissues and adjacent structures and organs will indicate a lesion caused by injury. To these may be added the occasional existence of two small episternal centers, which make their appearance one on either side of the jugular notch; they are probably vestiges of the episternal bone of the monotremata and lizards. Occasionally some of the segments are formed from more than one center, the number and position of which vary, More rarely still the upper end of the sternum may be divided by a fissure. Union of the various centers of the body begins about puberty, and proceeds from below upward by the age of twenty-five they are all united. The xiphoid process may become joined to the body before the age of thirty, but this occurs more frequently after forty; on the other hand, it sometimes remains un united in old age. In advanced life the manubrium is occasionally joined to the body by bone. When this takes place, however, the bony tissue is generally only superficial, the central portion of the intervening cartilage remaining un ossified 1 . A sternal foramen, has been incidentally detected at CT in nearly 5% of the population Awareness of the presence of a sternal foramen in a patient who is undergoing acupuncture or sterna bone marrow aspiration is particularly important because of the risk of associated complications (eg, hemorrhage and cardiac tamponade.) A sternal foramen is well demonstrated at CT, with a typical bow-tie appearance on axial images of the sternal body .A vertical sclerotic band superior or inferior to the foramen is a common associated finding on coronal CT images. Rarely, a sternal cleft may be seen adjacent to a sternal foramen 3 6 . Minor sternal clefts (e.g., a notch or foramen in the xiphoid process) are common and are of no clinical concern 8 .It is possible that the formation of the sternum and proliferation of midlineangioblastic tissue may be affected by certain mechanisms during the sixth to ninth gestational weeks 10 . Further, in an asymptomatic patient with sternal cleft, careful investigation is needed to identify possible asymptomatic internal vascular anomalies. More frequently seen abnormalities of the lung and bronchial tree are abnormal divisions of the bronchial tree, sometimes resulting in the presence of supernumerary lobules, as in our two cases. Thesevariations in the bronchial tree are of little functional significance, but may cause unexpected difficulties in bronchoscopy 10 . Few doctors, and possibly fewer acupuncturists, are aware of congenital sternal foramina. Some authors conclude that if sternal acupuncture is planned in the corpus sterni region, radiographs should first be done to rule out this anomaly to avoid such fatal complications as cardiac tamponade following sternal puncture during treatment 10 Finally, 1. Severely macerated specimens should confirm the presence of a sternal foramen. The defect will be located in the midline through the lower half of the body of the sternum. The measurements of the defect will be the same on both the outer and inner surfaces of the bone. No beveling will be present on either surface. The edges with a hand lens will reveal it to be smooth and covered by cortical bone. 2. In specimens which have been exposed to insects, fauna, or marine animals, characteristic erosion, teeth, or claw marks may be present around the foramen, but these should not be mistaken for recent antemortem, traumatic injury. 3. The sternal foramen is a relatively rare congenital anomaly but when encountered by the pathologist in a case that has medicolegal implications, the failure to recognize it as a developmental abnormality can be a serious pitfall and hazard. 4. The misinterpretation of this bony defect by the nature of its location can result in ascribing a wrong cause and manner of death and frustrating, unnecessary expenditure of time and effort in the investigation of a suspected homicide or suicide 1 .
MEDICAL LEGAL IMPORTANCE
1. In badly decomposed bodies or skeletonized human remains a sternal defect may present a problem that can lead to misinterpretation and wrong conclusions which have serious consequences.
2. Postmortem artifacts of advanced putrification can obscure and mask the gross and microscopic changes of associated trauma.
3. In skeletons the character of the edges of the defect may be altered by scavenger animals or, when evaluating human skeletons which have been exposed or buried for longer periods of time, demineralization and erosion of the margins of the defect may have occurred.
4. The possibility of an old or recent gunshot wound or a traumatic penetrating lesion caused by an object other than a missile. X-rays of the body or remaining tissue parts and organs are necessary to rule out the presence of a missile. A separate X-ray of the sternum will disclose small metallic fragments about the defect that would be undetectable by gross examination.
5. Imaging of sternal foramen simulating osteolytic lesion 1, 3 . The defect in the body of sternum leaves only the skin separating the pleura and heart from the surface at the affected site, thus any penetrating injury would easily access the heart and cause more severe damage than would normally be. The longer manubrium is unusual and can be both a clinical, radiological and medico-legal challenge when encountered 7 .
APPLIED ASPECTS
- Clinicians should be aware of this anatomic variation, because needle insertions in this area may lead to fatal complications Knowledge of the existence of such anatomic variants is important to avoid misdiagnosis as an osteolytic process 3 .
- The possibility of a sternal foramen should be mentioned to the clinician because infiltration, biopsy or acupuncture of this area may lead to fatal cardiac complications2 .
- Sternal foramina may pose a great hazard during sternal puncture, due to inadvertent cardiac or great vessel injury. They can also be misinterpreted as osteolytic lesions in crosssectional imaging of the sternum.
- Variant xiphoid morphology such as bifid, duplicated, or trifurcated may be mistaken for fractures during imaging3. These variations may complicate sternal puncture, and due caution is recommended. The variant xiphisternal morphology may raise alarm for xiphoid fractures and may therefore be considered a differential 2 . Also, important in radiological diagnosis, therapeutic procedures, forensic and medical legal pathological identifications. It is essential to students of medicine, radiology, anatomy and forensic pathology just as each variation could have unique features different from others,
CONCLUSIONS
The findings that are recorded is accordance with literatureThis have been not only a focus of attention of anatomists but also at interest of Genetitians, Embryologists, oncologists, paediatric endocrinologists, surgeons, physicians, psychiatrists, Forensic experts because it makes very verysensivitiv issue on the boy, family and society. Variations in numbers of both vertebrae and ribs do occur which can be subnumerary or supernumerary, and are important in radiological diagnosis, the rapeutic procedures, forensic and medical legal pathological identifications. Knowledge of such variation is essential to students of medicine, radiology, anatomy and forensic pathology just as each variation could have unique features different from others, and could be associated with a number of other congenital anomalies. The discovery of the sternum being different from the usual is important additions to the variations that are expected on the thoracic cage hence need to put this finding in serious consideration during our medical training and practice. Clinicians should be aware of the anatomic variation, because needle insertions in this area may lead to fatal complications 3 .
HIGH SIGNIFICANCE
1. Sternal foramina were significantly in blacks and episternal anomaly in whites. Sternal foramina had no sex predilection.
2. Sternal bone with sternal foramen, fracture and osteoporosis, and that bone marrow aspiration from sternal bones might not be as safe as previously thought.
3. In a retrospective review of the bone scan, patients with breast cancer, found to represent metastatic disease. The sternal lesions may with regional lymphatic tumor spread than hematogenous seeding and so local recurrence common. The incidence and significance of isolated sternal metastases undergoing radionucide bone imaging.
4. Many anatomic variants and congenital anomalies may affect the both sternum and sternoclavicular joints involved in pathologic conditions, including degenerative changes, arthritides, trauma, infection, and primary and secondary tumors.
5.Sternal foramen is a congenital oval fusion defect of the sternum occurring in up to 6.7% of autopsy and prevalence of focal bone thinning, fissures and other abnormalities seen in sternum can be detetected with bone scintigraphy, radiography, and CT imaging.
6. Sternal wound complications may result from median sternotomy procedures following cardiothoracic surgery and can represent a significant management problem like infections and can increase hospital stay, morbidity and mortality, but modern techiniques improves the conditions.
7. MDCT exhibits various sternal variations and anomalies. Sternal foramen is a frequent minor anomaly with sternal sclerotic bands. Early manubriosternal and sternoxiphoidal fusions can be seen in early adulthood with out osteo degeneration. Double-ended xiphoid process and single xiphoidal foramen are frequent sternal variations.
8. A bifid sternum is a rare congenital anomaly diagnosed as asymptomatic at birth may with other congenital anomalies or may be diagnosed only in adult life.
9. A complete congenital sternal cleft (absent sternum) with abnormalities of midline fusion may with pericardial defect and \ or with pectus excavatum of incidence is 0.15% of all chest deformities is very rare. In neonates this and the sternal bars can be easily approximated by simple suture, due to the flexibility of the cartilaginous thorax with little danger of cardiac compression when the repair is performed early in life (1stmonth).
10. The imperfect union is known as midlinesternal foramens, an anomalies mistaken for a gunshot wound or by CT, High resolution computed tomography (HRCT) and visual inspection in the lower part of the sternum, even in the manubrium may be with displacement of the heart or other midline abnormalities.
11.Sternal cleft is a midline defect. May be Incomplete (common) or complete (rare) it leads to mediastinal structures ( the heart and great vessels) can easily be injured by external trauma with no familial, teratogenic or nutritional factors have been identified as a potential cause . Failure of fusion of the lateral sternal bands by an early disturbance affecting the midline mesodermal structures between the 6 th and 9 th IUL. Multiplanar and 3D reconstructed multidetector CT (MDCT) images are useful in the evaluation of the human skeleton - the sternum.
12. Misinterpretation of autopsy findings (artifacts) from forensic pathology are major cause of concern to forensic scientists encountered in the medicolegal autopsy of skeletonized human remains.
13. Sternal foramina may leads great hazard during sternal puncture, due to inadvertent cardiac or great vessel injury . May be mistaken as osteolytic lesions in c\s imaging of the sternum. variant xiphoid morphology such as bifid, duplicated, or trifurcated may be mistaken for fractures.
14. Bony union of the segments of the stenum starts in early childhood but is normally not complete before the 15yrs of life (Ashley, 1954). Early fusion or defective segmentation of the sternum with congenital heart disease seen. Currarino et al. (1958) reported; A large septal defect with a wide ductus arteriosus confirmed by autopsy, noticed one radiological evidence of an aberrant right subclavian artery.
15 Episternal bones were commonly on unilateral [left] than bilateral with out any clinical significance, they are of potential forensic value in individual identification.
ACKNOWLEDGEMENTS
Author acknowledges the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. Special thanks and I am grateful to my brother Anil for his moral support and encouragement during preparation of paper.
References:
1. J Forensic Sci, Oct. 1974, Vol. 19, No. 4 H. L. Taylor,1 M.D. The Sternal Foramen: The Possible Forensic Misinterpretation of an Anatomic Abnormality.
2. Sternal foramina and variant xiphoid morphology in a Kenyan population) H. ElBusaid, etal.
3. Sternal Foramen Simulating Osteolytic Lesion on Scintigraphy and SPET Imaging. Philip Pevenage1, Michel De Maeseneer2, Kristoff Muylle1, Michel Osteaux21 Department of Nuclear Medicine; 2Department of Radiology Brussels, Belgium.
4. CASE REPORT-- Bifid sternum Year : 2012, Volume : 29, Issue : 1, Page : 73-75Sibes Kumar Das1, Pulak Kumar Jana2, Tapan Das Bairagya3, Bhaswati Ghoshal .
5. Lane F. Donnelly, MD, Donald P. Frush, MD, Joseph N. Foss, MD2,Sara M. O'Hara, MD and George S. Bisset III, MD- Anterior Chest Wall: Frequency of Anatomic Variations in Children.
6. [Henry Gray (1821–1865). Anatomy of the Human Body. 1918. The Sternum.Ossification of sternum.
7. Sternal Anomalies with Supernumerary and Subnumerary Vertebrae and Ribs – Case Reports East and Central African Journal of Surgery, Vol. 12, No. 1, April, 2006, Vol. 12, Num. 1, 2007, pp. 99-104. Ochieng, J. and Ibingira, C.B.R.Department of Anatomy, faculty of medicine, Makerere University Uganda Email: ochiengjoe@yahoo.com.
8. Skeletal System Development. Development of Human Skeletal System Copyright © 2011 by U. Bala)
9. Sternum -Francois Manson, MD ; Philippe Jeanty, MD, PhD.
10. Anatomic and HRCT Demonstration of Midline Sternal Foramina,Tr. J. of Medical Sciences28 (1998) 511-514.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





