IJCRR - 5(1), January, 2013
Pages: 54-57
Print Article
Download XML Download PDF
UTILITY OF ULTRASOUND GUIDED FINE NEEDLE ASPIRATION CYTOLOGY IN ASSESSING AXILLARY LYMPH NODE STATUS IN CARCINOMA BREAST
Author: Sandhyalakshmi B.N., Poornima Naregal , Rajeev Gothe, M.H. Kulkarni
Category: Healthcare
Abstract:Assessment of lymphnode status in carcinoma breast is an important factor in staging. Lymphnode status can be evaluated by different methods such as physical examination and sentinel node biopsy. Ultra sonography features such as round, hypo echoic, with loss of central hilum, eccentric cortical hypertrophy of lymphnode indicate the malignant involvement of lymph nodes. This study was conducted to evaluate the ultra sonography features of metastatically involved axillary lymphnodes. Ultrasound guided fine needle aspiration of involved axillary lymph nodes was done to confirm the findings. Ultrasonography of axillary lymphnodes will detect the small lymphnodes which can be missed on physical examination. Ultrasound guided fine needle aspiration will help in removal of metastatically involved lymphnodes in axillary clearance in a single surgery.
Keywords: Ultrasound, FNAC, Axillary lymphnode, Carcinoma breast.
Full Text:
INTRODUCTION
Axillary lymph node status is the most important prognostic factor in breast cancer. The presence of nodal metastases decreases 5-year survival by approximately 40% compared to node-negative patients. Noninvasive imaging techniques have been used to predict the preoperative axillary lymph node status. Ultra Sonography has higher diagnostic accuracy than mammography, computed tomography, magnetic resonance imaging, and positron emission tomography for diagnosing axillary node metastasis1,3.However axillary sonography has been shown to be moderately sensitive (48.8%–87.1%). UltraSonography is reported to be more sensitive in the detection of metastatic axillary lymph nodes than palpation or mammography2, 6 . Fine needle aspiration cytology (FNAC) of radiologically abnormal axillary lymph nodes in patients with breast cancer can identify patients suitable for primary axillary clearance rather than sentinel node biopsy, enabling surgical axillary staging by a single operation 4 .
MATERIALS AND METHODS This study was carried out in Karnataka institute of medical sciences, Hubli, Karnataka a tertiary care centre for one year (2006-2007). Thirty cases of carcinoma breast diagnosed on fine needle aspiration cytology were selected for detection of axillary lymphnode status. Axillary lymphnodes were palpated to know the presence in these 30 cases. Verbal consent was taken by the patients after explaining the procedure. They were subjected to conventional fine needle aspiration cytology first and US guided fine needle aspiration cytology later.
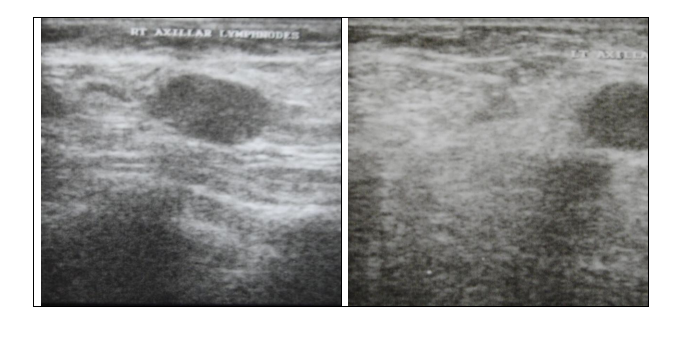
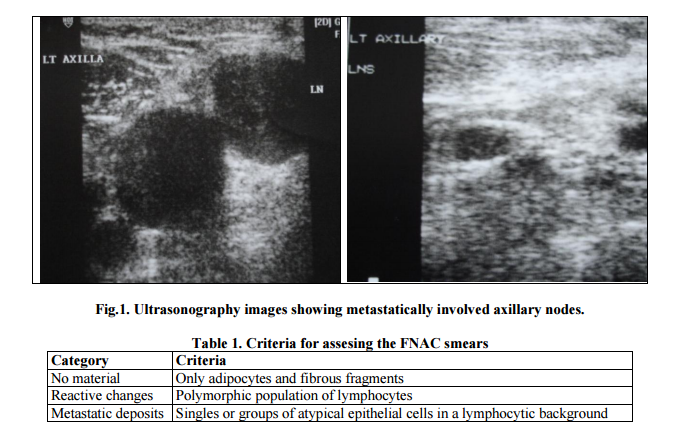
Philips HDI Ultrasonography machine along with hand held probe was used to determine the status of axillary lymphnodes. Ultrasonographically axillary nodes that are round, hypo echoic, with loss of central hilum, eccentric cortical hypertrophy were considered malignant and others were reactive. Lymphnodes either positive or negative on sonography basis were selected for fine needle aspiration cytology. Fine needle aspiration cytology was done using 5ml syringe with 20-22 gauge needle. Smears stained with H&E stain and Wright’s stain were examined. They were categorised as no material, reactive changes and metastatic deposits as depicted in Table 1 and Fig.1.
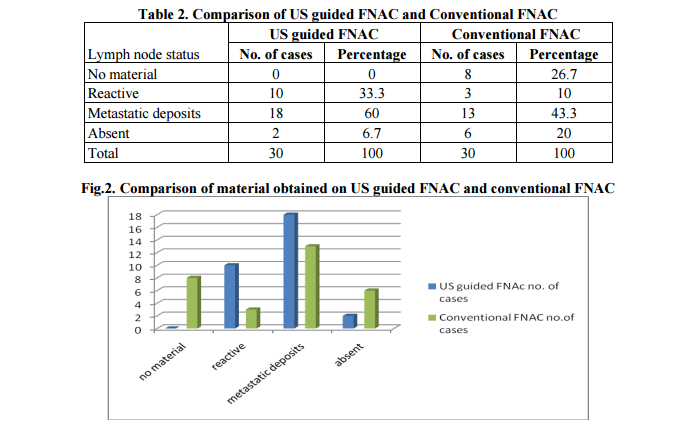
RESULTS In the present study, 2 cases did not have any axillary lymphnodes while on physical examination 6 were negative. Ultrasonography assesment of lymphnodes whether they were reactive or metastatically involved were complimented by FNAC. None of the cases on US guided FNAC showed no material while 8 cases yielded no material on conventional FNAC. Reactive features were seen in 10 cases on US guided FNAC and 3 cases on conventional FNAC. Metastatic deposits was seen in 18 cases on US guided FNAC and 13 on conventional FNAC. Physical examination did yield positive results only when the lymphnodes were of sufficient size (>2cms) but not for the lymphnodes which were smaller. Ultrasonography showed the lymphnodes immaterial of the size (smaller being 0.5cms) along with additional information of metastatic deposits as depicted in Table 2 and Figure 2.
DISCUSSION Breast cancer is the second most common malignancy in India after carcinoma of cervix 7 . The incidence of breast carcinoma is increasing among the young females. Early diagnosis of carcinoma will have better prognosis and has varied modalities of treatment. Initial assesment of a lump in a breast can be done with mammography, ultrasonography, fine needle aspiration cytology, core biopsy and excision biopsy. Once the lump has been diagnosed as carcinoma staging becomes the important prognostic factor. Assesment of axillary lymphnode status is an important factor in staging of breast cancer. Many of the times axillary lymphnodes are missed on physical examination of axilla owing to smaller size or deeper location and it will affect the staging. Traditional use of axillary sentinel node biopsy raised issue of false negative results 8 . These false negative cases may be because of massive metastasis in a single lymphnode in the draining area3 .The use of ultrasonography in detecting axillary lymphnode status has limited application because of low sensitivity (48.8%– 87.1%) 2 .
However use of sonography to detect metastically involved lymphnodes will reduce the sentinel lymphnode biopsies. It will also help in diagnosing metastatically involved lymphnodes which might have been missed on physical examination. Ultrasonography is much more cost effective , can be used in centres where the facility for CT and MRI are not available. US guided FNAC will compliment the diagnostic findings of sonography. With precise assesment of lymphnode status staging can be more accurate. Axillary clearence incase of involved nodes can be done with primary removal of breast tumor in a single operation. Hence it will reduce the two stage surgery or surgery at a later date.
CONCLUSION Ultra sonography of axillary lymphnodes will help in identifying the enlarged axillary lymphnodes which can be missed by physical examination. The charachteristic features of metastatically involved lymphnodes will help in proper staging of carcinoma breast. Ultra sonography guided fine needle aspiration cytology will compliment the findings and help in removal of metastatically involved lymphnodes in a single surgery.
ACKNOWLEDGEMENTS: To all the patients who were part of this study for their co-operation. To the editorial committee for accepting and publishing this artcle.
References:
1. Jae Jeong Choi, Bong Joo Kang, Sung Hun Kim, Ji Hye Lee, Seung Hee Jeong, Hyun Woo Yim et al. Role of Sonographic Elastography in the Differential Diagnosis of Axillary Lymph Nodes in Breast Cancer. J Ultrasound Med 2011; 30:429–436.
2. Isil Gunhan-Bilgen, Esin Emin Ustun, Aysenur Memis. Inflammatory Breast Carcinoma: Mammographic, Ultrasonographic, Clinical and Pathologic Findings in 142 cases. Radiology 2002; 223:829–838.
3. Soledad Alvarez, Enrique Añorbe, Pilar Alcorta, Fernando López, Ignacio Alonso, Julia Cortés. Role of Sonography in the Diagnosis of Axillary Lymph Node Metastases in Breast Cancer: A Systematic Review. AJR 2006; 186:1342–1348.
4. Brian D Hayes, Linda Feeley, Cecily M Quinn, M M Kennedy, Ann O'Doherty, Fidelma Flanagan et al. Axillary fine needle aspiration cytology for pre-operative staging of patients with screen-detected invasive breast carcinoma. J Clin Pathol 2011;64: 338-342.
5. J N Bruneton, E Caramella, M Héry, D Aubanel, J J Manzino and J L Picard. Axillary lymph node metastases in breast cancer: preoperative detection with US. Radiology, 158, February 1986; 325- 326.
6. Valerie P.Jackson. The role of US in breast imaging. Radiology1990; 177:305-311.
7. Patra AK, Malik RN, Dash S. Fine needle aspiration as a primary diagnostic procedure of breast lumps. Indian J Pathol Microbiol 1991; 34(4):259-64.
8. Fraile M, Rull M, Julian FJ, et al. Sentinel node biopsy as a practical alternative to axillary lymphnode dissection in breast cancer patients: an approach to its validity. Ann Oncol 2000; 11:701–705.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





