IJCRR - 5(2), January, 2013
Pages: 94-100
Date of Publication: 26-Jan-2013
Print Article
Download XML Download PDF
ACCURACY OF ULTRASOUND GUIDED FINE NEEDLE ASPIRATION CYTOLOGY IN THE EVALUATION OF THYROID NODULES
Author: Senthil Panneerselvam, Rajan K. Vaithianathan, Ramachandran Santhanam
Category: Healthcare
Abstract:Background: Thyroid nodules are a common problem which requires an accurate cytological diagnosis for proper management. An essential investigation modality is fine needle aspiration cytology (FNAC) with a sensitivity ranging between 80-90%. Recommendations vary regarding the use of ultrasound in improving the accuracy of free hand fine needle aspiration biopsy. Objective: The aim of our study was to investigate the role and accuracy of ultrasound guided fine needle aspiration cytology in the evaluation of patients with thyroid nodules. Methods: Forty four patients with nodular thyroid disease who were assessed by ultrasound guided fine needle aspiration cytology (US-FNAC) followed by thyroidectomy were identified. Retrospective analysis of data on the cytology specimens and histological results was carried out. Results: The sensitivity and specificity of US-FNAC for diagnosing thyroid neoplasms were 91.7% and 93.3% respectively. The diagnostic accuracy was 92.8%, with the rate of inadequate smears as 4.6%. Conclusions: Ultrasound guided fine needle cytology of thyroid nodules yields more accurate results, with a decrease in the number of inadequate sample category. Precise targeting of lesions in both palpable and non palpable thyroid nodules by the FNA needle under ultrasound guidance will increase the diagnostic accuracy, thereby avoiding or reducing the number of unnecessary thyroid surgeries.
Keywords: thyroid nodule, ultrasound guided, FNAC, neoplasm
Full Text:
INTRODUCTION
Nodular thyroid disease is found in approximately 5% of the population at palpation screening. Routine ultrasound screening of thyroid in clinically normal individuals suggests a prevalence rate of 50% for thyroid nodules 1, 2 . Fine needle aspiration cytology (FNAC) of the thyroid gland is over 50 years old and is the single most important method of establishing a diagnosis in both adults and children. Recent guidelines published by the British Thyroid Association/Royal College of Physicians and the American Association of Clinical Endocrinologists (AACE)/Association Medici Endocrinologi(AME) emphasize that FNAC should be considered as the early investigation of choice for thyroid nodules and specifically for thyroid cancer 4,5 FNAC requires careful aspiration technique and meticulous interpretation of the findings by a skilled cytologist. Studies have suggested a sensitivity and specificity for predicting thyroid malignancies averaging 83% and 92% respectively 5, 6 . Unfortunately, FNAC can miss malignancies with a false negative rate of approximately 5% . Current guidelines recommend the usage of ultrasound guided FNAC (US FNAC) to reduce this error 1,5 .Studies have shown that US FNAC significantly reduces the number of inadequate fine needle aspirates and improves the diagnostic yield for malignancies 1,10 US FNAC also improves the yield of cancer found at surgery 11 The aim of our study was to investigate the role and accuracy of ultrasound guided fine needle aspiration cytology in the management of patients with thyroid nodules.
PATIENTS AND METHODS
Two hundred and eighty two FNACs of thyroid nodules were carried out at Mahatma Gandhi Medical College and Research Institute and the results reviewed. Out of this, 44 patients had US FNAC for assessment of thyroid nodules followed by thyroidectomy. A retrospective analysis of the data was carried out that included patient demographics, US FNAC results and the final histopathological reports. All patients had baseline thyroid function tests followed by ultrasound examination and guided FNAC of the thyroid nodules. A high resolution 7.5 MHz probe was used to guide a 23/25 gauge needle attached to a syringe to obtain cellular aspirates from the lesions. Cytological diagnosis was correlated with histopathology and the accuracy of ultrasound guided FNAC
Study parameters:
- Demographic data
- Sensitivity, specificity
- Positive and negative predictive values
- Diagnostic accuracy rate
- Inadequate sample category
RESULTS
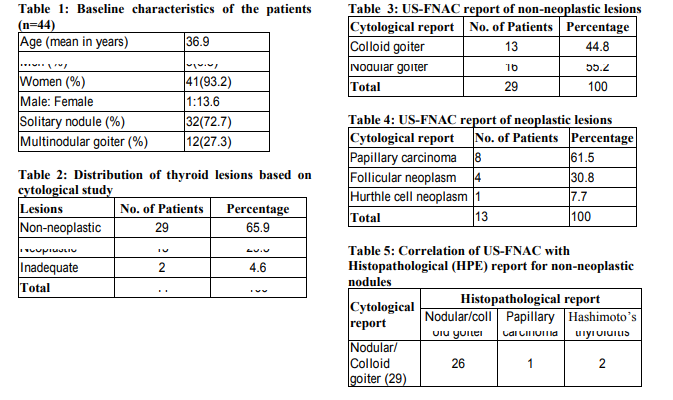
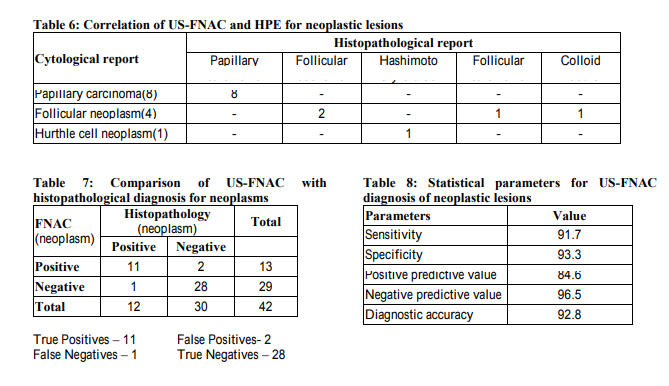
Data regarding 44 patients who had undergone US FNAC of the thyroid nodules followed by thyroidectomy was retrospectively analyzed. There were 3 men and 41 women in the study group, with age ranging from 18 to 51 years. The mean age was 39.6 years with male to female ratio of 1:13.7(Table 1). 29(63.6%) patients had non neoplastic lesions (nodular/colloid goiter, thyroiditis) and 14(31.8%) had neoplastic lesions on cytological examination. Overall, US FNAC yielded satisfactory cell samples in 42(95.4%) patients and inadequate material in 2(4.6%) patients (Table 2). An aspirate was considered adequate by the presence of 5 to 6 clusters of cells with each cluster containing 10 or more cells. Nodular goiter constituted the majority (55.2%) in the non neoplastic category and papillary carcinoma was the commonest (61.5%) cytological diagnosis in the neoplastic group as shown in Tables 3 and 4. On comparing the US FNAC reports of the 29 non neoplastic nodules with the final histological diagnosis, it was observed that 26 patients had same cytological diagnosis, 1 had papillary carcinoma (false negative) and 2 had Hashimoto’s thyroiditis (Table 5). The US FNAC results for the 13 neoplastic lesions were compared with the corresponding histological diagnoses. 8 patients had papillary carcinoma confirmed by histological study and out of 4 cases of follicular neoplasm, 2 were confirmed as follicular adenoma and 1 each of colloid goiter (false positive) and follicular carcinoma. One patient diagnosed as Hurthle cell neoplasm by US FNAC turned out to be Hashimoto’s thyroiditis on final histological study (false positive), Table 6. The sensitivity and specificity of US FNAC for diagnosing neoplastic lesions were 91.7% and 93.3% respectively. The diagnostic accuracy was 92.8%, positive predictive value (PPV) was 86.5% and negative predictive value (NPV) 96.5% (Table 7 and Table 8).
DISCUSSION
FNAC is considered as the gold standard in the evaluation of thyroid nodules. Major problems associated with free hand FNAC are significant false negatives (missed neoplasms) and difficulties in accurate identification of follicular lesions leading to wrong FNAC diagnoses 12 . Possible reasons cited for this include the technique of aspiration, smear preparation and experience of the cytopathologist. The AACE/AME has suggested that ultrasound should be employed routinely to detect features suspicious of malignancy in thyroid nodules and to identify lesions that would be suitable for FNAC . Ultrasound (US) is useful to guide the needle for fine needle aspiration of a thyroid nodule; it improves the quality of diagnosis in pre operative assessment of thyroid nodules and to appropriately select patients for thyroidectomy. Ultrasound guidance allows continuous visualization of the needle during insertion and sampling, which results in pinpoint accuracy with a high evel of safety. Some of the potential advantages of US FNAC in the evaluation of nodular thyroid disease are selecting the suspicious nodule for biopsy in a multinodular goiter and guiding the needle to take samples from nonpalpable nodules. A recent review of studies that evaluated the role of US FNAC in the detection of thyroid cancer revealed a sensitivity of 76%–98%, specificity of 71%–100%, false negative rate of 0%–5%, false positive rate of 0–5.7%, and overall accuracy of 69%–97% 13 23 . Another report based on a systematic review of 12 studies had shown a median sensitivity and specificity of 88% and 90.5% 24 . A large prospective cohort study had reported a marked increase in the diagnostic accuracy of FNAC from 85% to 95% when FNAC was combined with US guidance 25 . Our results have shown a sensitivity and specificity of US FNAC for diagnosing neoplastic lesions as 91.7% and 93.3% respectively. The false negative rate was 2.3%, PPV 86.5%, NPV 96.5% and the diagnostic accuracy was 92.8%. The accuracy of FNAC depends crucially on the technique, operator performing the aspiration and the cytopathologist analyzing it. Even under optimal conditions, the false negative rate for thyroid neoplasms can vary from 1% to 6% due to wrong diagnosis or sampling errors . Danese et al in their study have observed the false negative rate much lower for US FNAC when compared with free hand FNAC 27 . In our analysis, there was one patient who had cytological picture of nodular goiter whereas the histological study showed a small focus of papillary carcinoma in a background of multinodular goiter(false negative 2.3%). The majority of thyroid FNAC is now performed under US guidance and this has become mandatory at some of the centers. The major benefit of this technique is accurate sampling of small or multiple nodules 28 30 . Certain sonologic features of thyroid lesions are predictive of malignancy and hence such lesions can be accurately biopsied 31 . Another crucial benefit of using US FNAC is significant reduction in the number of inadequate aspirates 32 . Case series have reported rates of inadequate samples in the order of 15 30% for free hand FNAC. Many published studies have shown US FNAC to decrease the rate of inadequate samples from 15% to 3% when compared to free hand FNAC 17,33,34 . In a recent study, the authors have noted a prevalence rate of 8.5% for thyroid cancer in patients with inadequate samples and they recommended repeat aspirations by US FNAC technique 35 . It is possible that reduced number of inadequate aspirates may potentially lead to increase in the yield of cancer and the diagnostic accuracy of FNAC. The rate of inadequate specimens in our retrospective study was 4.5 % (2 out of 44 samples), which is comparable to the above quoted studies.
CONCLUSION
In conclusion, US FNAC greatly facilitates the precise and adequate sampling of tissues from thyroid lesions thus enabling the cytopathologist to make an accurate diagnosis. This may lead to the elimination of the cost and potential morbidity of unnecessary thyroidectomy.
Ultrasound guidance helps in the selection of the most suspicious focus within the nodule especially with a background of multinodularity. It is therefore desirable that practice guidelines recommend universal use of ultrasound guided FNAC for all nodular thyroid lesions, especially for inadequate smears from free hand FNAC, for small or nonpalpable nodules and multinodular goiters. US FNAC is the most accurate and cost effective method for diagnostic evaluation of thyroid nodules.
ACKNOWLEDGEMENTS
Authors acknowledge the immense help received from the scholars whose articles are citied and included in references of this manuscript. The authors are also grateful to authors/ editors/publishers of all those articles, journals and books from where the literature for this article has been review and discussed. Authors are grateful to IJCRR editorial board members and IJCRR team of reviewers who have helped to bring quality to this manuscript. The authors also thank all the residents and staff in the Department of Surgery, Departments of Pathology and Radiology, Dean and Vice Chancellor of Mahatma Gandhi Medical College & Research Institute for their support.
References:
1. Cramer H. Fine needle aspiration cytology of the thyroid: an appraisal. Cancer Cytopathol 2000; 90:325–
2. American Association of Clinical Endocrinologists and Asso ciazione Medici Endocrinologi medical guidelines for clinical practice for the diagnosis and management of thyroid nodules. Endocr Pract 2006; 12:63 102
3. Soderstrom N. Puncture of goiters for aspiration biopsy. Acta Med Scand 1952; 144:237–44
4. Perros P. Report of the Thyroid Cancer Guidelines Update Group.2nd ed. London: Royal College of Physicians; 2007. British Thyroid Association, Royal College of Physicians. Guidelines for the management of thyroid cancer.
5. Cobin RH, Gharib H, Bergman DA, Clark OH, Cooper DS, Daniels GH, et al. AACE/AAES medical/surgical guidelines for clinical practice: management of thyroid carcinoma. American Association of Clinical Endocrinologists. American College of Endocrinology. Endocr Pract. 2001; 7:202– 20.
6. Gharib H. Fine needle aspiration biopsy of thyroid nodules: Advantages, limitations, and effect. Mayo Clin Proc. 1994; 69:44–9.
7. Castro MR, Gharib H. Thyroid fine needle aspiration biopsy: Progress, practice, and pitfalls. Endocr Pract. 2003; 9:128–36.
8. Gharib H, Goellner JR. Fine needle aspiration biopsy of thyroid nodules. Endocr Pract. 1995;1:410–17.
9. Jeffrey PB, Miller TR. Fine needle aspiration cytology of the thyroid. Pathology (Phila) 1996;4:319–35.
10. Ahmet Selcuk Can and Kamil Peker. Comparison of palpation versus ultrasound guided fine needle aspiration biopsies in the evaluation of thyroid nodules. BMC Research Notes 2008; 1:12
11. Dilip K Sankhala, Samir S Hussein, Haddia Bererhi, Omeima El Shafie, Nicholas J Woodhouse, V Nirmala. Are scintigraphy and Ultrasonography necessary before fine needle aspiration cytology for thyroid nodules? Squ journal for scientific research Medical sciences 2001; 1: 29 33.
12. Kopald KH, Layfield LJ, Mohrmann R, Foshaq LJ, Giuliano AE. Clarifying the role of fine needle aspiration cytologic evaluation and frozen section examination in the operative management of thyroid cancer. Arch Surg 1989;124:1201–5.
13. Wu HH, Jones JN, Osman J. Fine needle aspiration cytology of the thyroid: ten years experience in a community teaching hospital. Diagn Cytopathol 2006;34:93–96.
14. Serna de la Saravia C, Cuellar F, Saravio Day E, Harach HR. Accuracy of aspiration cytology in thyroid cancer: a study in 1 institution. Acta Cytol 2006;50:384–387.
15. Sangalli G, Serio G, Zampatti C, Bellotti M, Lomuscio G. Fine needle aspiration cytology of the thyroid: a comparison of 5469 cytological and final histological diagnoses. Cytopathology 2006;17: 245–250.
16. Sahin M, Sengul A, Berki Z, Tutuncu NB, uvener ND. Ultrasound guided fine needle aspiration biopsy and ultrasonographic features of infracenti metric nodules in patients with nodular goiter: correlation with pathological findings. Endocr Pathol 2006;17:67–74.
17. Cai XJ, Valiyaparambath N, Nixon P, Waghorn A, Giles T, Helliwell T. Ultrasound guided fine needle aspiration cytology in the diagnosis and manage ment of thyroid nodules. Cytopathology 2006;17: 251–256.
18. Zagorianakou P, Malamou Mitsi V, Zagorianakou N, Stefanou D, Tsatsoulis A, Agnantis NJ. The role of fine needle aspiration biopsy in the management of patients with thyroid nodules. In Vivo 2005;19: 605–609.
19. Sclabas GM, Staerkel GA, Shapiro SE, et al. Fine needle aspiration of the thyroid and correlation with histopathology in a contemporary series of 240 patients. Am J Surg 2003;186:702–709; dis cussion 709– 710.
20. Ogawa Y, Kato Y, Ikeda K, et al. The value of ultrasound guided fine needle aspiration cytology for thyroid nodules: an assessment of its diagnostic potential and pitfalls. Surg Today 2001;31:97–101.
21. Mittendorf EA, Tamarkin SW, McHenry CR. The results of ultrasound guided fine needle aspiration biopsy for evaluation of nodular thyroid disease. Surgery 2002;132:648–653; discussion 653–654.
22. Kessler A, Gavriel H, Zahav S, et al. Accuracy and consistency of fine needle aspiration biopsy in the diagnosis and management of solitary thyroid nod ules. Isr Med Assoc J 2005;7:371–373.
23. Blanco Carrera C, Garcia Diaz JD, Maqueda Villaizan E, Martinez Onsurbe P, Pelaez Torres N, Saavedra Vallejo P. Diagnostic efficacy of fine needle aspiration biopsy in patients with thyroid nodular disease: analysis of 510 cases [in Spanish]. Rev Clin Esp 2005; 205:374–378.
24. Belfiore A, La Rosa GL. Fine needle aspiration biopsy of the thyroid. Endocrinol Metab Clin North Am 2001;30:361–400.
25. Koike E, Yamashita H, Noguchi S, Murakami T, Ohshima A, Maruta J, et al. Effect of combining ultrasonography and ultrasound guided fine needle aspiration biopsy findings for the diagnosis of thyroid nodules. Eur J Surg2001;167:656 1.
26. Mazzaferri EL. Management of a solitary thyroid nodule. N Engl J Med 1993;328:553 9.
27. Danese D, Sciacchitano S, Farsetti A, Andreoli M, Pontecorvi A. Diagnostic accuracy of conventional versus sonography guided fine needle aspiration biopsy of thyroid nodules. Thyroid 1998;8:15–21.
28. Cai XJ, Valiyaparambath N, Nixon Pet al. Ultrasound guided fine needle aspiration cytology in the diagnosis and management of thyroid nodules. Cytopathology 2006;17:251–6.
29. Robinson IA, Cozens NJA. Does a joint ultrasound guided cytology clinic optimize the cytological evaluation of head and neck masses?. Clin Radiol 1999;54:312–6.
30. Kojic Katovic S, Halbauer M, Tomic Brzac H. Importance of FNAC in the detection of tumours within multinodular goiter of the thyroid. Cytopathology 2004;15:206–11.
31. Kovacevic O, Skurla MS. Sonographic diagnosis of thyroid nodules: correlation with the results of sonographically guided fine needle aspiration biopsy. J Clin Ultrasound 2007;35:63–7.
32. Cesur M, Corapcioglu D, Bulut S, et al. Comparison of palpation guided fine needle aspiration biopsy to ultrasound guided fine needle aspiration biopsy in the evaluation of thyroid nodules. Thyroid 2006; 16:555–61.
33. Baskin HJ. Ultrasound guided fine needle aspiration biopsy of thyroid nodules and multinodular goiters. Endocr Pract 2004; 10:242 5.
34. Izquierdo R, Arekat MR, Knudson PE, Kartun KF, Khurana K, Kort K, Numann PJ: Comparison of palpation guided versus ultra sound guided fine needle aspiration biopsies of thyroid nodules in an outpatient endocrinology practice. Endocr Pract 2006; 12:609 14.
35. Orija IB, Pineyro M, Biscotti C, Reddy SS, Hamrahian AH: Value of repeating a non diagnostic thyroid fine needle aspiration biopsy. Endocr Pract 2007; 13:735 42.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





