IJCRR - 5(2), January, 2013
Pages: 83-93
Date of Publication: 26-Jan-2013
Print Article
Download XML Download PDF
RISK FACTORS FOR BREAST CARCINOMA: A CASE CONTROL STUDY, CENTRAL INDIA
Author: Namrata Thakur, Arun Humne
Category: Healthcare
Abstract:Background: The upward trend in breast cancer globally and in India has become a matter of great concern. Breast cancer is the most common site-specific cancer in women. Geographical variations in incidence and mortality rates of breast cancer suggest the known risk factors for breast cancer may vary in different parts of the world and that environmental factors are of greater importance than genetic factors. It is important to identify these factors in order to bring down the incidence, morbidity and mortality due to this disease. Aim: To study some risk factors associated with breast carcinoma and to assess their strength of association. Setting, Design and Period: This was a case control study carried out in Government Medical College, Nagpur from August 2010 to February 2011. Material and Methods: we have studied 240 women which included 120 histopathologically confirmed cases of breast carcinoma and 120 age (?5 years) and residence (rural / urban) matched controls. The risk factors studied were religion, education, socioeconomic status, diet, marital status, age at marriage, age at menarche, parity, age at first childbirth, duration of breastfeeding, use of oral contraceptive pills, age at menopause, duration of reproductive life, hormone replacement therapy, exposure to radiation, previous benign breast condition, family history and time since initiation of breastfeeding after delivery. Results and conclusion: After adjusting with known risk factors, the strongest risk was observed in women having past H/O breast condition followed by Bouddha religion, age at menarche < 14 years, cumulative duration of breastfeeding ? 36 months, upper socioeconomic status and duration of reproductive life > 30 years.
Keywords: breast carcinoma, risk factors, case control, India.
Full Text:
INTRODUCTION
Urbanization, industrialization, changes in life style, population growth and ageing all have contributed for epidemiological transition in the country. The absolute number of new cancer cases is increasing rapidly, due to growth in the size of the population and increase in the proportion of elderly persons because of improved life expectancy following control of communicable diseases.2 Breast cancer is the most common site-specific cancer, and is the leading cause of death from cancer in women.3 Breast cancer incidence has been increasing in the general population all over the world and particularly in areas of low incidence such as Asia.4Breast cancer is second to cancer of the cervix among women in India. Cancer of the breast has replaced cancer of the cervix as the leading site of cancer in all urban PBCRs, except Chennai.5 The incidence of cancer varies substantially according to age, sex, socioeconomic status (SES), race or ethnicity, geographic location, and time period. These variations have provided strong evidence that much of cancer is caused by environmental factors and is potentially avoidable.6 Another well established risk factor is a family history of breast cancer. Ovarian hormones, particularly estrogens, play a major role in breast cancer development. Many of the other established risk factors are surrogate measures of a woman’s cumulative exposure to estrogen and possibly, progesterone. These include early age at menarche, late age at menopause, nulliparity or late age at first birth, lack of or short-term breast-feeding, alcohol intake of at least one drink per day, obesity after menopause, and long-term use of hormone replacement therapy (HRT) 7 . The effects of diet on breast cancer risk still are being debated.8 It is important to identify these factors to bring down the incidence, morbidity and mortality due to this disease. Only few epidemiological studies have been conducted to determine the risk factors of breast cancer in Indian women. In central India they are even less. Hence, this study was undertaken to review the breast cancer patients at a tertiary care center with respect to their sociodemographic characteristics and risk factors that contributed to develop the disease.
METHODOLOGY
A retrospective case-control study was conducted to assess the relationships between some clinicosocial variables and breast cancer risk in central India. Cases comprised of 120 histologically confirmed female breast cancer patients who presented in the inpatients and outpatients departments of Oncology from August 2010 to February 2011. Control subjects were matched one for one with age (? 5 years) and place of residence (rural or urban). They were selected from the community. The controls for urban cases were selected from field practice area of urban health training centre of study institution. For rural cases, to get controls the nearest Taluka was selected purposively. There are 4 PHCs in the selected Taluka. Out of that one PHC was selected by simple random sampling by lottery method. In the selected PHC, there are 7 subcentres. Out of that, one subcentre was selected by simple random sampling by lottery method. The eligible women were then examined clinically in their home ensuring privacy and those without lump in breast were selected as controls. Those with a palpable lump were referred to our tertiary care centre for further investigation and management. Exclusion criteria for controls were those with known malignant diseases, those who are pregnant or who are lactating their offsprings. A structured questionnaire was prepared in English and in-person interviews were conducted for both cases and controls. Written informed consent was taken from every patient. The questionnaires were divided into several sections comprising socio-demography, reproductive history and established and potential risk factors for breast cancer. Age at menarche was defined as the chronological age when the woman first had her menses. Menopausal status was defined when there have been no menses for a year (natural menopause) 9 or those undergone hysterectomy. Age at first full-term pregnancy was defined as the age of the woman at the last date of her first pregnancy that extended into completed 28 weeks, regardless of the outcome of the pregnancy. Socioeconomic status for urban and rural study subjects was assessed by modified Kuppuswamy’s classification and B G Prasad’s classification respectively. For purpose of analysis, socioeconomic status I was labeled for study subjects belonging to Class I of Prasad’s Classification and Upper Class of Kuppuswamy classification; socioeconomic status II was labeled for study subjects belonging to Class II of Prasad’s Classification and Upper Middle Class of Kuppuswamy classification; and so on. The sample size was based on OR for age at first full term birth ? 25 years of 2.59 with case: control = 1:1. A sample size of 232 was calculated including 116 subjects in each group with 80% precision and 95% confidence. The actual sample studied was 240 (120 per each group).10 All data entry and analyses were conducted using STATA 10.1, 2009. Means and standard deviations (SD) for continuous variables and frequencies and percentages for categorical variables were calculated. Differences of proportions between cases and controls for categorical variables were analysed by simple conditional logistic regression.Crude odds ratios (OR) for variables in the model were drawn from simple conditional logistic regression. The level of significance was set at p < 0.05 for all hypotheses tests in this study. Significant predictors for breast cancer were determined using multiple conditional logistic regression analysis in order to control possible confounders. All variables found significant at alpha=0.02 were included in the saturated model of multivariate analysis. All possible risk factors were independent variables and cases and controls were the dichotomous binary outcomes. The analysis was started by removing the largest p-value one at a time. The adjusted odds ratios were estimated with 95% confidence intervals (CI).
OBSERVATIONS
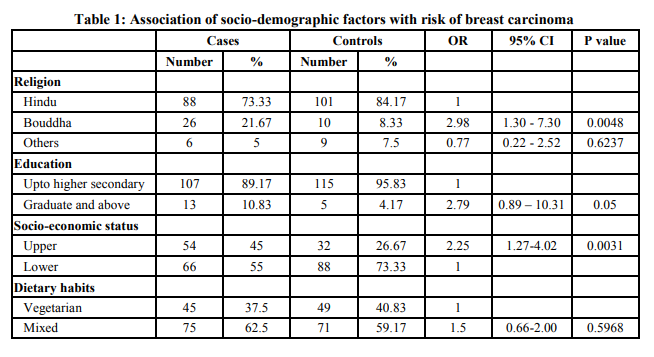
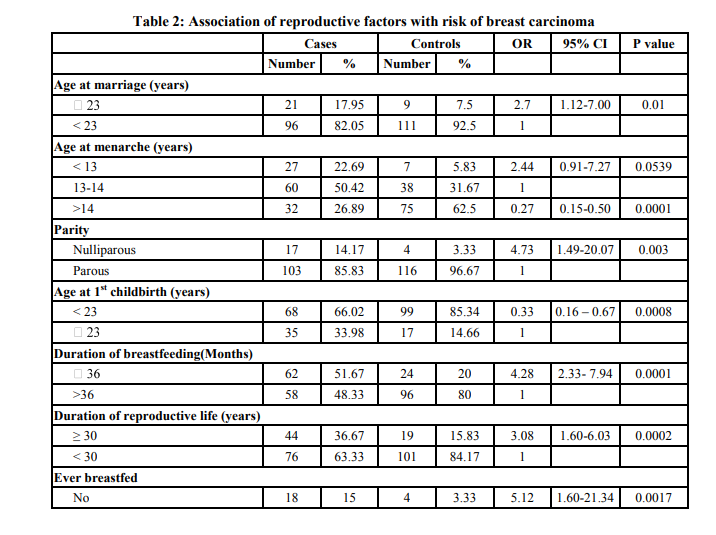
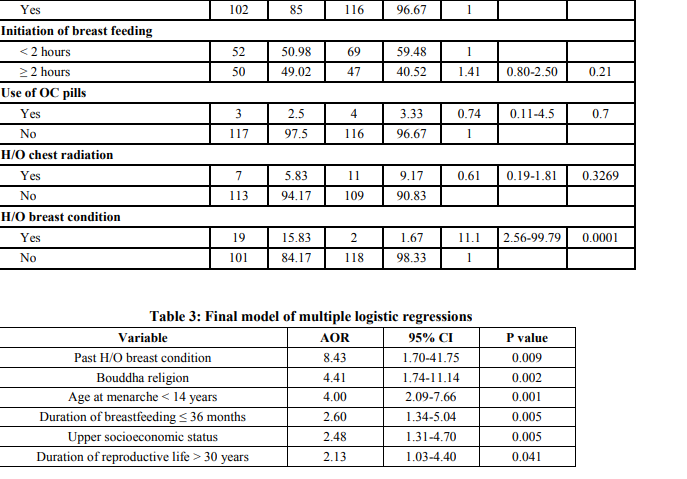
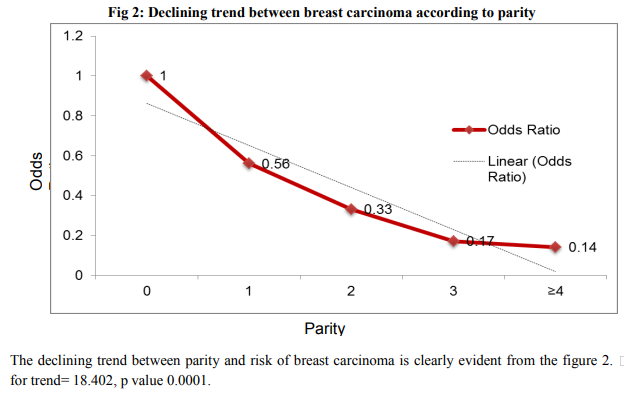
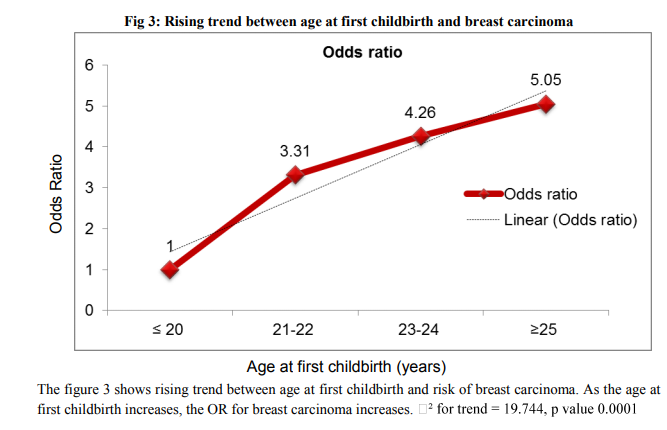
Table I shows the socio-demographical characteristics of the subjects. There were no significant differences in education level and dietary habits between cases and controls. Buddhist women and those with higher education were at risk of breast carcinoma than others. Table II shows the reproductive characteristics of the subjects. Age at marriage, age at menarche, parity, age at 1st childbirth, duration of breastfeeding, duration of reproductive life were found to be significant. From the figure 1 it is clearly evident that as age at menarche increased, risk of developing breast carcinoma decreased. Thus a declining trend between age at menarche and risk of breast carcinoma was observed, value 0.0001 The declining trend between parity and risk of breast carcinoma is clearly evident from the figure 2. The figure 3 shows rising trend between age at first childbirth and risk of breast carcinoma. As the age at first childbirth increases, the OR for breast carcinoma increases. 19.744, p value 0.0001 Table III shows the results of multiple conditional logistic regression analysis of risk factors of female breast cancer. After adjusting with known risk factors, the strongest risk was observed in women having past H/O breast condition, AOR = 8.43 (1.70-41.75); followed by Bouddha religion, AOR = 4.41 (1.74-11.14). Next stronger risk factors were age at menarche < 14 years, AOR = 4.00 (2.09 – 7.66); cumulative duration of breastfeeding ≤ 36 months, AOR = 2.60 (1.34 – 5.04); upper socioeconomic status, AOR = 2.48 (1.31-4.70) and duration of reproductive life > 30 years, AOR = 2.13 (1.03 – 4.40). Thus all the above mentioned factors had independent risk of their own in development of breast carcinoma and the AOR indicated the respective strength of the risk. Only one case has received hormone replacement therapy. Also only 4 cases and 1 control had family history of breast cancer, hence their association with breast carcinoma could not be assessed.
DISCUSSION
Much of the increase of breast cancer in India has been associated with greater urbanization and changing life styles. The rural: urban case ratio in present study reaffirms the fact that this disease is no longer confined to an urban setting. Amongst the well established risk factors for breast carcinoma, only past H/O breast condition, early menarche, no or less duration of breastfeeding, upper socioeconomic status and longer duration of reproductive life were significantly associated with higher risks of breast cancer in this study. Although several variables, such as age at marriage, parous after 23 years old, were significant in univariate analyses, they were not found significant in multivariate analysis. Traditionally, women in India would marry in their mid-teens; bear children at earlier ages and breastfeed their children for long periods, which were protective lifestyles against breast cancer. There is an increasing trend to abandon these traditional habits of reproduction. There are increasing occupational and tertiary educational opportunities for women that influence their marital status and childbearing. Many have postponed marriages or having children and some may not be able to get partners at all and remained childless. The number of children the women had and the age they had their first child were related closely to each other. Those who had their first child at earlier ages tend to have more children than those who had their first child at later ages. The marrying age of women has an influence on their fertility, namely the number of children and age at first birth of these women. If this pattern of reproductive behavior is not monitored, there will be an increasing proportion of women with reproductive risk factors of breast cancer that will lead to a higher incidence of breast cancer. Buddhist women were at a greater risk of developing breast carcinoma than Hindu women. While Muslim and other religion were not having any significant risk. However as in this study cases were taken from hospital; a community based study is further needed to generalize the finding. It is a known fact that the disease risk is high among Parsi women mainly due to certain favorable risk factors such as late age at marriages, lack of breastfeeding and nulliparity or low parity.11 Only one case was Parsi in the present study this may be because, Parsis usually belong to higher socioeconomic group and hence they may not be attending government hospitals. In our study, it was observed the risk of developing breast carcinoma did not vary significantly as far as the level of education is concerned. Similar findings were noted by Montazeri A et al 12, Norsa’adah B et al 13 , Ebrahimi M et al .14 Although few authers1,15,16 have found that higher education was a significant risk factor for breast carcinoma. Delayed marriage and tendency to have small family in high educated women might explain the risk in high educated women. In the present study it was noted that women belonging to upper socioeconomic status were at a risk of developing breast carcinoma than women in lower socioeconomic status. Findings are consistent with other studies 15,17 . The risk level for non-vegetarians was higher than for vegetarians, but the difference was not statistically significant. Vegetarians who totally avoid animal meat, fish and poultry products generally consume less fat than non-vegetarians. In this context, the odds ratio was expected to be higher among the non-vegetarian group than among the vegetarian group since a diet with a high animal fat intake has been shown to increase the risk of breast cancer. Further studies are required to identify the association of dietary factors in breast cancer. When the group of married women was compared against others, no significant association was found between marital status and risk of breast carcinoma. The findings are consistent with other authors 2,12,13,14,20 . Jussawala D J et al 11 had noticed higher risk of breast cancer in unmarried women. Although association of breast cancer with unmarried state is well known, the finding in present study may be due to fact that, the number of unmarried women in the present study was less. In the present study, the mean age at marriage of cases (19.83 yrs) was found to be significantly higher than the mean age at marriage of controls (18.72 yrs). In the present study, out of 117 married cases, 48 (41.03%) were married on or before 18 yrs and 64 (53.33%) controls were married on or before 18 yrs. Women married at or after 23 yrs were at highly significant risk of developing breast carcinoma than those married before that. Similarly Meshram II et al 2 found that 82.18% cases and 90.38% controls were married at or before 20 years old. The risk was found to be 2.04 times higher in women married after 20 yrs of age than those before. Also, the findings are consistent with Rao D N et al 20 , Gajlakshmi C K et al 21 . In the present study, Women who attained menarche at > 14 yrs were at significant decreased risk of breast carcinoma as compared with those attaining it between 13 -14 yrs. Also a linear decreasing trend was observed between the age of attaining menarche and the risk of developing breast carcinoma. Meshram II et al 2 , Hadjisavvas A et al 22 also had similar findings. However few authors 18,12,14,21 did not find any association between age at menarche and risk of breast cancer. It has been estimated that during most of the 20th century age at menarche has been falling by about 3 months per decade.23 This may contribute to future burden of disease. Nulliparas were at of risk of breast carcinoma compared to parous women,. As the parity increased, risk of breast carcinoma decreased. Meshram II et al 1 and Gajalakshmi V et al 15 had also observed decreasing trend with parity and risk of breast carcinoma. Norsa’adah B et al 13 , Ebrahimi M et al 14 also found protective effect of parity for breast carcinoma. The women who had age at first childbirth < 23 yrs were having significant protection against breast carcinoma. Also there is a rising trend between age at first childbirth and risk of breast carcinoma. Meshram II et al2 Harrison AP et al19 , Gajalakshami V et al15 also had similar findings. However Hadjisavvas A et al22 , Pakseresht S et al18, Montazeri A et al12 had not got such association. The most well established and documented data about endocrinological factors that decrease breast cancer risk are ever having breast fed and longer durations of breast feeding (2, 22, 18, 15) . Many studies showing a longer duration of breast feeding decreases breast cancer risk; findings from present study are consistent with them. The explanation given by Byers T et al26 for protective effect of breastfeeding on breast cancer that process of lactation per se could be seen as somewhat beneficial. This effect could be either direct causing changes within the breast which protect against cancer or indirect via modulation of pituitary and/or ovarian activity and alternatively successful lactation could be seen as an indicator of normally balanced endocrine system and unsuccessful lactation as a correlate of underlying normal imbalance which might cause increased risk of breast cancer. No association was found between initiation of breastfeeding after delivery and breast carcinoma. The milk from the unsuckled breasts had a slightly higher pH27..It has been suggested that an alkaline milieu surrounding epithelial cells plays an important role in carcinogenesis of epithelial surfaces28.An alkaline milieu surrounding epithelial cells causes hyperplasia, cell atypia and a marked increase in mitotic activity, changes which are a prelude to neoplasia. No association was found between H/O oral contraceptive pill use and risk of breast cancer was found in present study. Some Indian 2, 18 and foreign 12, 14 studies also have noted similar findings. However studies by Yavari P et al29 , Daud N A 17 have found increased risk of breast cancer in OC pill users. In the present study, the no significant risk was observed; this may be due to small sample in both cases and controls.
The mean age at menopause was comparable in cases and controls. The findings are consistent with previous authers.18,12,14 However few studies2,21 have got such association. The duration of reproductive life in majority of the study subjects; 65 (54.17%) cases and 83 (69.17%) controls; was 21 – 30 yrs. The women who had the duration of reproductive life ? 30 yrs were at a risk of breast carcinoma than those having it < 30 yrs. The findings of current study are consistent with others2,30 . However Yavari P et al29 have not found such association. No association was found between exposure to chest radiation and risk of breast carcinoma in present study. Although Yavari P et al29 had found such association, it could not be seen in present study because of fewer samples in case and control groups. Women who had history of breast diseases in past were at a significant greater risk for breast carcinoma than those who had not. Our findings are consistent with findings of other authors 2,31 However Daud N A17, Yavari P et al29 have not found such association. No significant association was found between family history of breast cancer and risk of breast carcinoma in present study. Pakseresht S et al18 . Montazeri A et al12, Daud N A17 found that family history of breast cancer was not associated with risk of breast cancer. Many authors 22,12,29,14 had found association between family history of breast cancer and risk of breast cancer. The association may not be evident in present study due to less number of subjects with positive family history. In the present study only one case had ever received hormone replacement therapy. So the association between exogenous estrogen and risk of breast carcinoma could not be assessed. However Daud N A17 has not got such type of association. The major drawback of this study was the reliance on recall and self-reported information. Recall bias was unavoidable, especially for elderly women recalling past events such as age at menarche. However, recall bias of reproductive history was less likely, since factors such as breastfeeding and taking OC were related closely to major events in a woman’s life. Women tended to remember accurately pregnancy-related events and were unlikely to under-report such occasions. As this study was a hospital-based study, there was selection bias in hospital utilisation and the intake of cases, which might not be representative of all women with breast cancer. There is an increased probability of hospitalisation among severe and advanced cases, compared to those with fewer complications and those at an early stage of breast cancer. This might be the reason that majority of cases in this study were at advanced stages. Hospital-based cases represent a selective population because going to a hospital is culturally influenced and dependent upon perception of hospital facilities, reputation, policies and staff competency. Cases and controls were from the same source of population that may have the same probability of exposure, thus improving comparability. Careful criteria were applied to eliminate patients with conditions that shared the same known or potential exposure for breast cancer.
CONCLUSIONS
Factors related to reproductive life like early menarche, late marriage, late childbirth, nulliparity and longer duration of reproductive life are found to be significant risk factors for development of breast carcinoma. Longer duration of breastfeeding is a protective factor for development of breast carcinoma. Women having past history of breast condition are at significant risk of developing breast carcinoma. Bouddha religion and higher socioeconomic status are significantly associated with risk of development of breast carcinoma.
RECOMMENDATIONS
Increasing duration of breastfeeding was found to be protective factor for development of breast carcinoma; hence breastfeeding for a longer duration should be promoted. As women with past H/O breast condition were found to be at greater risk of development of breast carcinoma and the time lag between detection of lump by women and presentation to hospital was high; there is need for health education on self breast examination and early presentation to health facility for better management. Also periodic checkups are recommended for those women with past H/O breast condition
References:
1. Datta K, Biswas J. Influence of Dietary Habits, Physical Activity and Affluence Factors on Breast Cancer in East India - A Case-control Study. Asian Pacific J Cancer Prev,2009; 10:219-222
2. Meshram II, Hiwarkar PA, Kulkarni PN. Reproductive Risk Factors for Breast Cancer: A Case Control Study, Online J Health Allied Scs. 2009;8(3):5
3. Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics,2002. CA Cancer J Clin 2005, 55:74-108.
4. Ahmad M. Risk factors for breast cancer among women attending breast clinic in University Malaya Medical Centre Kuala Lumpur. NCD Malaysia, 2003; 2(4): 23-31. 5
. Development of an atlas of cancer in India, First All India Report. 2001-2002
6. Doll R., and Peto R. The causes of cancer: quantitative estimates of avoidable risks of cancer in the United States J Natl Cancer Inst, 1981; 66:1191 – 308
7. Henderson BE, Ross RK, Bernstein L. Estrogens as a cause of human cancer: the Richard and Hinda Rosenthal Foundation Award Lecture. Cancer Res. 1988;48:246– 253. Smith RA, Caleffi M, Albert US, et al. Breast cancer in limited-resource countries: early detection and access to care. Breast J, 2006; 12 (Suppl 1):S16-26.
8. Friedenreich C, Bryant HE, Courneya KS. Case-control study of lifetime physical activity and breast cancer risk. Am JEpidemiol. 2001;154:336–347.
9. Padubidri V G, Daftary S N. Hawkins and Bourne Shaw’s Textbook of Gynaecology, Elsevier Publication, 13th edition, 2002:56.
10. Lwanga S K and Lameshaw S Sample size determination in health studies: A practical manual, Geneva: World Health Organization, 1991
11. Jussawala D J, Yeole B B, Natekar M V. Histological and epidemiological feature of breast cancer in different religion groups in Greater Bombay. J of Surgical Oncology 1981;18: 269 – 79.
12. Montazeri A, Sadighi J, Farzadi F, Maftoon F, Vahdaninia M, Ansari M et al. Weight, height, body mass index and risk of breast cancer in postmenopausal women: a casecontrol study. BMC Cancer 2008, 8:278
13. Norsa’adah B, Rusli B N, Imran A K, Naing I, Winn T. Risk factors of breast cancer in women in Kelantan, Malaysia. Singapore Med J 2005; 46(12) : 698
14. Ebrahimi M, Vahdaninia M and Montazeri A. Risk factors for breast cancer in Iran: a case–control study. Breast Cancer Res 2002, 4:R10
15. Gajalakshmi V, Mathew A, Brennan P, Rajan B, Kanimozhi V C, Mathews A, et al Breastfeeding and breast cancer risk in India: A multicenter case-control study. Int. J. Cancer, 2009;125:662–665
16. Bala DV, Patel DD, Duffy SW, Cherman S, Patel PS, Trivedi J, et al. Role of dietary intake and biomarkers in risk of breast cancer: a case control study. Asian Pac J Cancer Prev 2001;2:123-30.
17. Daud N A. A study of risk factors of breast cancer among registered female patient in Kuala lumpur hospital between July 2001 to September 2001. NCD Malaysia 2004; 3:29- 34.
18. Pakseresht S, Ingle G K, Bahadur A K,Ramteke V K, Singh M M, Garg S et al. Risk factors with breast cancer among women in Delhi. Indian J Cancer 2009,46(2):132-138
19. Harrison AP, Srinivasan K, Binu VS, Vidyasagar MS, Nair S. Risk factors for breast cancer among women attending a tertiary care hospital in southern India International Journal of Collaborative Research on Internal Medicine and Public Health, 2010,2(4):109-116
20. Rao D N, Ganesh B and Desai P B. Role of reproductive factors in breast cancer in a lowrisk area: a case -control study. Br. J. Cancer, 1994; 70:129 132
21. Gajalakshami C K, Shanta V. Risk factors for female breast cancer a hospital-based casecontrol study in Madras, India.Acta Oncologica , 1991;30(5):569 - 574
22. Hadjisavvas A, Loizidou M A, Middleton N, Michael T, Papachristoforou R, Kakouri E et al. An investigation of breast cancer risk factors in Cyprus: a case control study. BMC Cancer 2010, 10:447
23. Karapanou O, Papadimitriou A. Determinants of menarche. Reproductive Biology and Endocrinology 2010, 8:115
24. McCormack VA, Mangtani P, Bhakta D, McMichael A J and I dos Santos Silva. Heterogeneity of breast cancer risk within the South Asian female population in England: a population-based case–control study of firstgeneration migrants.British Journal of Cancer,2004; 90:160 – 166
25. Michels K B, Willett W C, Rosner B A, Manson J E, Hunter D J, Colditz G A, et al. Prospective assessment of breast-feeding and breast cancer incidence among 89,887 women. Lancet 1996;347:431-6
26. Byers T, Graham S, Rzepka T, Marshall J. Lactation and breast cancer. Evidence for a negative association in premenopausal women. Am J Epidemiol 1985;12:664-74
27. Malhotra S L. Effect of non-suckling on the pH of breast milk and its possible relationship with breast cancer Postgraduate Medical Journal (December 1982) 58, 749- 752
28. Malhotra, S L (1977a) A study of cancer of breast with special reference to its causation and prevention. Medical Hypotheses, 3(1), 21.
29. Yavari P , Mosavizadeh M, Sadrol-Hefazi B, Mehrabi Y,et al. Reproductive Characteristics and the Risk of Breast Cancer – A Casecontrol Study in Iran. Asian Pacific J Cancer Prev,2005,6, 370-375
30. Sharpio S, Straux P, Venet L, Fink R : The search for risk factors in breasr cancer. AJPH 1968;58: 820 – 835;
31. Yang P S, Yang T L, Liu C L, Wu C W and Shen C Y. A case-control study of breast cancer in Taiwan - a low-incidence area. British Journal of Cancer, 1997;75(5):752- 756.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





