IJCRR - 5(2), January, 2013
Pages: 66-70
Date of Publication: 26-Jan-2013
Print Article
Download XML Download PDF
A STUDY OF THE CONDYLAR CANAL AND ITS INCIDENCE, MORPHOLOGY AND CLINICAL SIGNIFICANCE
Author: S. Kavitha, A. Anand
Category: Healthcare
Abstract:The posterior condylar canal is one among the largest and inconstant emissary foramina in the human skull. The canal, if present, may be single or multiple. It transmits the posterior condylar vein and meningeal branch of occipital artery. The present study was conducted to observe the incidence of posterior condylar canal and its morphological variations in dry adult human skulls. The dimensions and shape of the condylar fossa were also studied. In 78.9 % cases, it shows bilateral presentation where as in 21.1 % cases it presents unilaterally. Single canal or multiple smaller canals in clusters were also observed. Knowledge of such anatomical variations is important in case of treatment of dural arterio venous fistula involving the posterior condylar canal.
Keywords: Condylar fossa, canal, foramen
Full Text:
INTRODUCTION
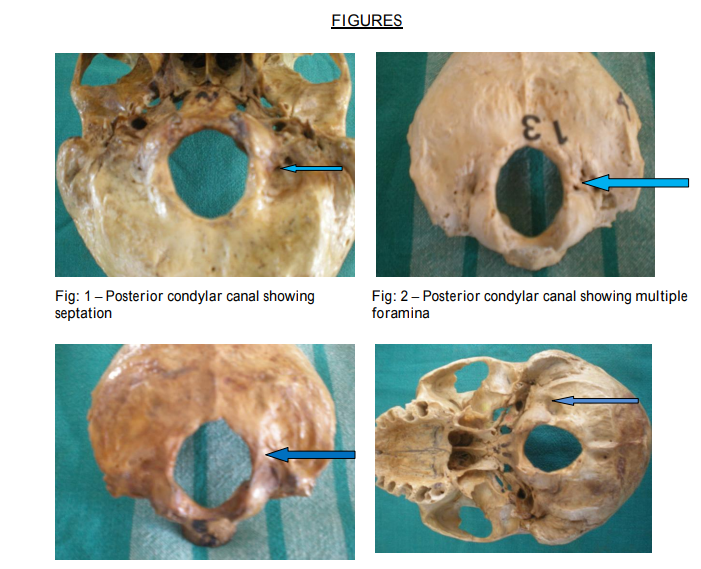
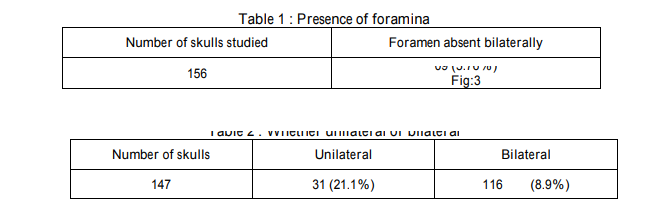
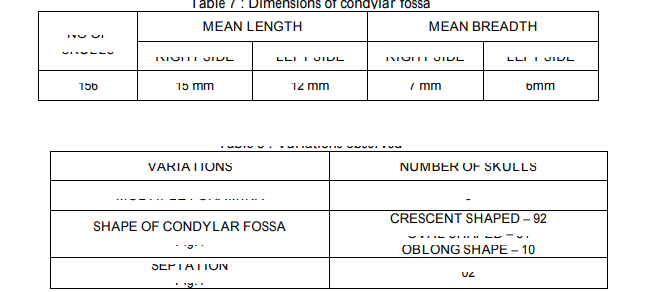
The posterior part of the occipital condyles exhibits a depression known as the condylar fossa. The superior articular facet of the atlas is accommodated within this fossa during movements of the atlanto occipital joint. Rarely within this fossa does a foramen be present which is called as the condylar canal or the posterior condylar canal . This foramen can be either unilateral or bilateral and the foramen may or may not be patent. If the foramen is patent, it usually transmits an emissary vein to the sigmoid sinus and nerves which supply the dura mater of the posterior cranial fossa. This emissary vein is called as the posterior condylar vein which connects the veins present in the sub occipital triangle with that of the sigmoid sinus The posterior condylar emissary vein communicates posteriorly with the vertebral venous plexus in the condylar fossa and anteriorly with the jugular bulb or the vein in the hypoglossal canal . The posterior condylar canal may also present itself as a doubled entity . Many canals exist in and around the occipital condyles which are grouped as paracondylar canals . These paracondylar canals when patent transmit emissary veins which can communicate with other veins The posterior condylar canal also transmits meningeal branches of the occipital artery . Anatomically the occipital dural venous sinus inside the falx cerebelli and occasionally it may present as a paired structure. This sinus usually drains into the confluence of sinus which is present close to the internal occipital protuberance and at the junction of falx cerebri and falx cerebelli. The posterior condylar vein which passes through the posterior condylar canal drains into the occipital sinus Compression of structures passing through the foramen can occur during movements of the atlanto occipital joint because the posterior margin of the atlas fits itself into the condylar fossa when the neck is fully extended . Such pressure on neurovascular structures can result in clinical symptoms. However there are reported cases of dural arteriovenous fistulas of the posterior condylar vein The lateral transcondylar approach is a surgical approach for skull base surgery. Particularly this approach involves extensive dissection and may cause injure the neurovascular structures . Many studies exist about the occipital condyles and its variations but there are not many studies about the posterior condylar canal and its variations of Indian ethnicity in literature. Therefore a thorough knowledge of the bony architecture of the posterior condylar canal and its variations is needed to be known before any procedure.
MATERIALS AND METHODS
About 156 human skulls were obtained from the department of Anatomy, Vinayaka Missions Kirupananda Variyar Medical College, Salem for the purpose of study. The equipments used for the purpose of study were hand lens, vernier calipers, measuring tape and digital photography equipment. The parameters studied were presence and absence of the foramina, whether the foramina were unilateral or bilateral, whether the foramina were patent or not, predominance of patency, dimensions of the condylar fossa and any abnormal bony variations in architecture were documented.
Statistical Analysis
Standard deviation, mean values and the range were calculated from the obtained results and parameters measured were evaluated by the paired sample t test to differentiate between the right and the left sides. The resultant p value was less than 0.05 making it statistically significant.
RESULTS
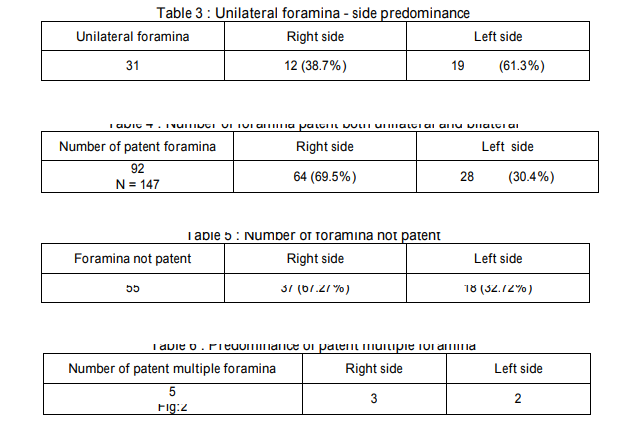
Of the 156 skulls studied, in 09 skulls the foramen was absent bilaterally (Table 1). In the remaining 147 skulls the foramen was present unilaterally in 31 skulls and bilaterally in 116 skulls (Table 2). Among the unilaterally present foramina it was more predominant on the left side (Table 3) and patent foramina were more on the right side (Table 4).Also foramina were not patent more on the right side (Table 5). Multiple foramina were present only in 05 skulls examined (Table 6).The dimensions of the condylar fossa were more on the right side than the left. Variations were also observed in the shape of the condylar fossa and appearance of the foramina (Table 8).
DISCUSSION
The posterior condylar canal is almost a constant entity in the condylar fossa and only in a miniscule percentage the canal is absent making it and the structures traversing through it clinically significant. In the present study, out of a 156 skulls studied, the foramen was absent bilaterally in 5.76% of the skulls therefore the structure is clinically important because the foramen is present in 94.2% and it connects the xtracranial veins with the intracranial dural venous sinuses. In the present study there is preponderance towards bilaterally present foramen (78.9%) and unilateral being (21.1%). Surprisingly when the foramen was unilateral more orientation was shown on the left side (61.3%) than the right (38.7%). Of the examined skulls more number of foramina was patent on the right side (69.5%) than the left (30.4%). In the skulls where the foramina were not patent there is a significant shift to the right (67.2%) than the left side (32.72%). Going by the significant number of patent foramina, planning and execution of any surgical procedure should consider any venous vascular abnormality which can produce serious repercussions intracranially either be it a fistula or a bleed. Planning any invasive procedures in specific cases of dural arteriovenous fistulas, the dimensions of condylar fossa are important for limiting the field of exposure. Of the examined skulls the crescent shaped condylar fossa was the most common (58.9%) followed by oval shaped (34.6%) and oblong shape (6.4%). The measurements of space where the articulation of the atlas takes place the mean length and breadth is more on the right (15mm and 7mm) than the left side (12mm and 6mm). The present study indicates that condylar fossa is broader on the right side than the left side. Surgical approaches to the foramen magnum and the craniocervical junction like the far lateral approach will involve extensive dissection of structures related to the posterior condylar canal and particularly the posterior condylar canal. Findings of the present study will serve as a bench mark as it pertains to Indian ethnicity and thorough knowledge of the surgical anatomy of this region and its reported variations should be disseminated to surgeons who perform difficult and complicated surgical procedures.
ACKNOWLEDGEMENTS
The authors sincerely wish to thank the management, administrators and the Professor and Head of the department of Anatomy of Vinayaka Missions Kirupananda Variyar Medical College, Salem for their whole hearted support and permissions to utilize their resources and conduct this study. The authors acknowledge the great help received from the scholars whose articles cited and included in references of this manuscript. The authors are also grateful to authors/editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. Authors are grateful to IJCRR editorial board members and IJCRR team of reviewers who have helped to bring quality to this manuscript.
References:
1. Susan Standring. Gray’s Anatomy, 40th Edition. Anatomical basis of clinical practice, Churchill Livingstone, London. 2008; 40:415.
2. Susan Standring . Gray’s Anatomy, 40th Edition. Anatomical basis of clinical practice, Churchill Livingstone, London. 2008; 40:432.
3. Toshio Matsushima et al; in Microsurgical Anatomy For lateral Approaches to the foramen magnum with special Reference to transcondylar fossa Approach. Skull base surgery, Vol 8, Number 3, 1998; 119.
4. Berge, J. K and Bergman, R.A. Variation in size and in symmetry of foramina of the human skull. Clin. Anat., 14 (6):406 13, 2001.
5. Tuli. A; et al, Incidence, morphology and Clinical relevance of bony canals and vascular grooves in the paracondylar region of adult human skull. J Clin Neurosci. 2008 Jun; 15(6): 689 92. Epub 2008 Apr 10.
6. H. Kiyosue, et al ; Dural Arteriovenous Fistula Involving the posterior condylar canal; Am J Neuroradiol 28: 1599 601, Sep 2007.
7. SanMillan Ruiz D, Gaillound P, Rufenacht DA, et al. The Cranio cervical venous system in relation to cerebral venous drainage. AJNR Am J Neuroradiol 2002; 23: 1500 08.
8. Emel AVCI et al; Anatomical Variations of the foramen Magnum, occipital condyle and Jugular Tubercle; Turkish Neurosurgery 2011, Vol: 21, No: 2, 181 190.

|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





