IJCRR - 5(4), February, 2013
Pages: 136-140
Date of Publication: 28-Feb-2013
Print Article
Download XML Download PDF
STUDY OF PALMAR DERMATOGLYPHICS IN CARCINOMA OF CERVIX
Author: Balsurkar Smita Kashinathappa, Khanzode Lata S.
Category: Healthcare
Abstract:In developing countries, most common cancer among women worldwide is carcinoma of cervix. The sample constituted 110 histopathologically confirmed cases of carcinoma of cervix and 110 normal healthy females with no obvious genetic disorder. Different parameters like fingertip patterns, interdigital area patterns, total finger ridge count (TFRC), absolute finger ridge count (AFRC), atd angle, palmar ridge count (a-b, b-c, c-d, t-d) were studied. Statistical analysis of data showed significant increase in frequency of whorls, total finger ridge count (TFRC), absolute finger ridge count (AFRC) & atd angle in both hands of carcinoma cervix patients as compared to controls. There was significant decrease in frequency of ulnar loops & t-d ridge count in both hands of carcinoma In developing countries, most common cancer among women worldwide is carcinoma of cervix. The sample constituted 110 histopathologically confirmed cases of carcinoma of cervix and 110 normal healthy females with no obvious genetic disorder. Different parameters like fingertip patterns, interdigital area patterns, total finger ridge count (TFRC), absolute finger ridge count (AFRC), atd angle, palmar ridge count (a-b, b-c, c-d, t-d) were studied. Statistical analysis of data showed significant increase in frequency of whorls, total finger ridge count (TFRC), absolute finger ridge count (AFRC) & atd angle in both hands of carcinoma cervix patients as compared to controls. There was significant decrease in frequency of ulnar loops & t-d ridge count in both hands of carcinoma cervix patients as compared to controls. While there was no any significant difference in the frequency of radial loops, arches, interdigital area patterns & a-b, b-c, c-d ridge counts between patients & controls.cervix patients as compared to controls. While there was no any significant difference in the frequency of radial loops, arches, interdigital area patterns & a-b, b-c, c-d ridge counts between patients & controls.
Keywords: Dermatoglyphics, Fingertip patterns, Interdigital area patterns, Finger ridge counts, atd angle, Palmar ridge counts.
Full Text:
INTRODUCTION
The skin on the fingertips, palmar surface and plantar surface of man has ridges, which form configurations that are unique to every individual. “Dermatoglyphics” is scientific study of epidermal ridges and their configurations on the volar aspect of palmar and plantar regions (Cummins and Midlo, 1926)3 . The dermatoglyphic patterns make their appearance on volar aspect of palm as early as 6th to 7th week of gestation. They become prominent and subsequently reach their maximum size by 12th week of gestation. Once formed in intrauterine life, these patterns don’t change throughout life (Penrose, 1969)8 . Carcinoma of cervix is the second most common cancer among women worldwide. Primary cause of carcinoma of cervix is not precisely known. Etiological factors for most of the malignancies in general include genetical, environmental or both. Twin studies have shown that heredity plays a role in its etiology. On the other hand the fact that carcinoma of cervix is uncommon in married Jewish women suggest involvement of some racial factors. The present study was undertaken to evaluate dermatoglyphic pattern in females of carcinoma cervix. An attempt was done to draw the conclusion regarding genetic basis of carcinoma cervix.
MATERIAL AND METHODS
The sample constituted 110 patients suffering from carcinoma of cervix, all above 25 years of age group. All patients in this study were histopathologically confirmed cases of carcinoma cervix. While selecting patients of carcinoma cervix, care was taken to rule out any other associated genetic disorder. The control group constituted of 110 females from general population which were normal healthy females with no other obvious genetic disorders, all above 25 years of age group. While selecting control, care was taken to rule out any hereditary disease and carcinoma in the family. Dermatoglyphic prints were taken by ‘INK METHOD’ described by Cummins (1936)2 . The subjects were asked to clean their hands and to dry them but leave some moisture. The requisite amount of ink was placed on the glass slab. It was uniformly spread by the rubber roller. The thin film of ink was applied on the palm by passing the inked rubber roller uniformly over the palm and digits taking care that the hollow of the palm and the flexor creases of the wrist were uniformly inked. The hands of subject were then placed on the sheet of paper from proximal to distal end. The palm was gently pressed between inter–metacarpal grooves at the root of fingers and on the dorsal side corresponding to thenar and hypothenar regions. The palm was then lifted from the paper in the reverse order from distal to proximal end. The fingers were rolled from radial to ulnar side to include all the patterns. The prints were subjected for detail dermatoglyphic analysis with the help of magnifying hand lens. Qualitative parameters (fingertip patterns- arches, radial loops, ulnar loops & whorls, patterns in five interdigital areasthenar/I, II, III, IV & hypothenar areas) & Quantitative parameters ( Total finger ridge countTFRC, Absolute finger ridge count- AFRC, atd angle, palmar ridge count like a-b, b-c, c-d & t-d ridge counts) were studied. For statistical analysis of qualitative data Chisquare test (X2 ) and for quantitative data t- test were applied.
OBSERVATION AND RESULTS
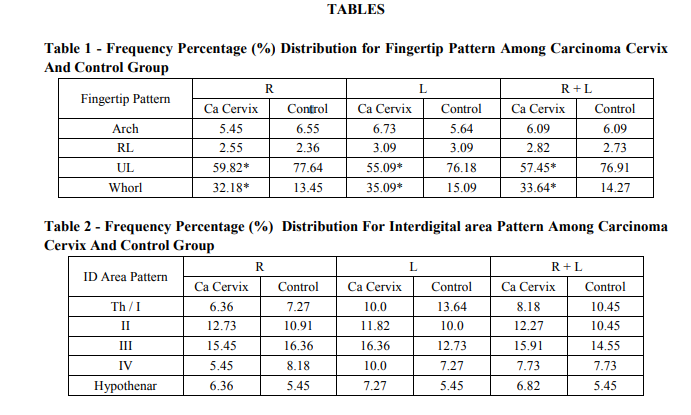
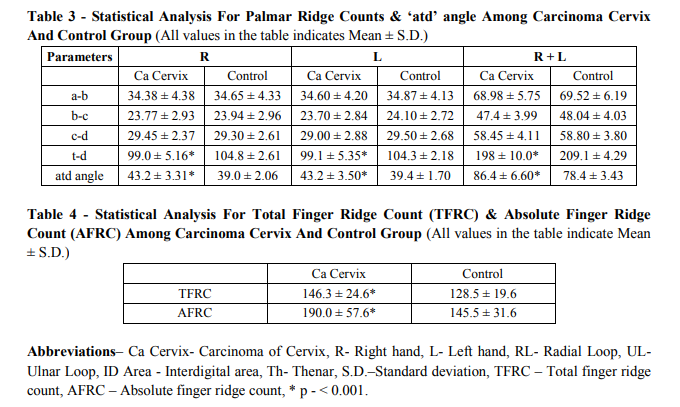
There was significant increase in frequency of whorls, total finger ridge count (TFRC), absolute finger ridge count (AFRC) & ‘atd’ angle in both hands of carcinoma cervix patients as compared to controls (p < 0.001). There was significant decrease in frequency of ulnar loops & t-d ridge count in both hands of carcinoma cervix patients as compared to controls (p< 0.001). While there was no any significant difference in the frequency of radial loops, arches, interdigital area patterns & a-b, b-c, c-d ridge counts between patients & controls (p > 0.05).
DISCUSSION
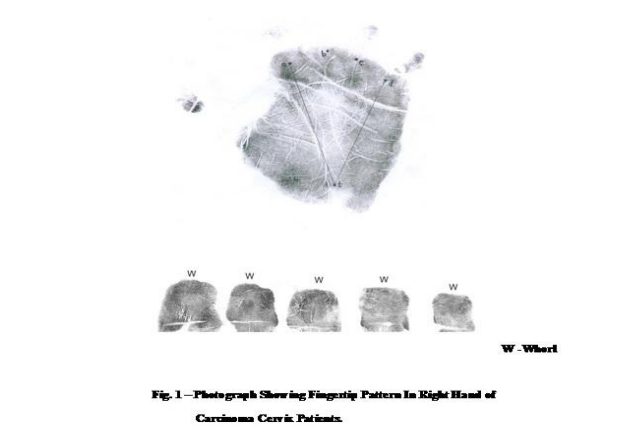
In developing countries, carcinoma cervix accounts for 80% of cancer & has genetic background (Park, 2000)6 . In malignancy there is increased and uncontrolled growth and since growth is controlled by genes, it indicates that genetic factor is involved in all cancers. However in some cancers primary cause is environmental and some cancers are common in certain races. The etiology of carcinoma of cervix is not clearly defined. Both racial and genetic factors seem to play a part in its causation. Twin study has shown that identical twins have slightly higher concordance of carcinoma of cervix as compared to non identical twins. This suggest genetic basis of carcinoma of cervix. Very little study has been done uptill now on dermatoglyphic features in carcinoma cervix. So the present study is undertaken to find out the variation of palmar dermatoglyphic pattern in carcinoma cervix which is compared and correlated with various workers. Pal G. P. et al (1985)7 observed significant high frequency of arches & low frequency of ulnar loops in both hands of patients of carcinoma of cervix. While Inamdar V.V. et al (2006)4 observed significant high frequency of whorls, low frequency of ulnar loops in both hands, in addition they also observed increased frequency of arches in left hand of carcinoma cervix group as compared to control group. Reddy S.S. et al (1977)9 has observed significant high frequency of whorls only in patients. Present study has revealed significant high frequency (p < 0.001) of whorls (Fig.1) and low frequency (p < 0.001) of ulnar loops in both hands of carcinoma cervix group as compared to control group (Table 1). While frequency of arches and radial loops were found to be non significant (p > 0.05) in both hands of carcinoma cervix group as compared to control group. Pal G. P. et al (1985)7 reported difference for III interdigital area where patients showed significant low frequency for presence of pattern while Inamdar V.V. et al (2006)4 has not observed significant difference for presence of interdigital area pattern between carcinoma cervix and control group. Reddy S.S. et al (1977)9 observed significant difference in frequency of presence of patterns in I, II and IV interdigital areas of patients and controls. In present study no difference (p > 0.05) was observed in the frequency of presence of patterns in palm i.e. I, II, III, IV and hypothenar patterns, in carcinoma of cervix group and control group (Table 2), which matches with the study of Inamdar V.V. et al (2006)4 . No significant difference was observed in a-b ridge count in carcinoma of cervix and control group by Reddy S.S. et al (1977)9 and Pal G.P. et al (1985)7 . Inamdar V.V. et al (2006)4 also has not observed any significant difference in a-b, b-c and c-d ridge count in carcinoma of cervix and control group. In present study, there was no difference (p > 0.05) in a-b, b-c and c-d ridge counts among carcinoma of cervix and control group, in both hands (Table 3). Inamdar V.V. et al (2006)4 & Reddy S.S. et al (1977)9 have reported significant decrease in t-d ridge count in both hands of carcinoma cervix group. Pal G.P. et al (1985)7 has observed decrease in t-d ridge count in both hands of carcinoma cervix group but it was not significant. Present study has observed significant decrease (p < 0.001) in t-d ridge count in both hands of carcinoma cervix group as compared to control group as observed by previous workers (Table 3). Pal G.P. et al (1985)7 reported significant increase in the value of ‘atd’ angle while Inamdar V.V. et al (2006)4 & Reddy S.S. et al (1977)9 have observed significant decrease in the value of ‘atd’ angle in both hands of carcinoma cervix group as compared to control group. In present study the value of ‘atd’ angle was found to be increased significantly (p < 0.001) in both hands of carcinoma cervix group as compared to control group (Table 3) which was also reported by Pal G.P. et al (1985)7 . As there is negative correlation between ‘atd’ angle and t-d ridge count (Berg, 1968)1 , decrease in t-d ridge count will give higher value of ‘atd’ angle. This correlation was not observed by Reddy S.S. et al (1977)9 and Inamdar V.V. et al (2006)4 . Pal G. P. et al (1985)7 reported significant decrease while Inamdar V.V. et al (2006)4 & Reddy S.S. et al (1977)9 have reported significant increase in total finger ridge count in patients as compared to controls. Present study has revealed a significant increase (p < 0.001) in total finger ridge count in patients as compared to controls (Table 4). As present study has revealed high frequency (p < 0.001) of whorls in patients (Fig.1), total finger ridge count is increased in carcinoma cervix group as compared to control group. As there is considerable variation with respect to finger ridgecount asymmetry and diversity from finger to finger (Jantz R.L., 1975)5 , the variation of mean total finger ridge count between the study of previous workers and present study is considerable. Absolute finger ridge count (AFRC) which represents the sum of ridge counts from all the separate triradii on all the ten digits was not studied by previous workers. A significant increase (p < 0.001) in absolute finger ridge count in carcinoma of cervix group as compared to control group was observed in present study (Table 4).
CONCLUSION
The results of our study along with those of other studies showed certain specific association between carcinoma of cervix and ridges indicating that genes which are responsible for disease are also responsible for abnormal ridge formation. This study has indicated that genetic background does exist for the same. A few of the contradictory findings between present study and other study groups can not be explained at this stage. Such variations between populations living in different regions are well known. But dermatoglyphic findings, which have shown association with the carcinoma of cervix, as a diagnostic aid will be of limited use at this stage. More detailed studies in different populations and in big sample size are desirable before arriving at some definitive conclusion.
References:
1. Berg J.M. (1968): A study of t-d dermal ridge count on the human palm. Human Biology, 40: 375-385.
2. Cummins H. (1936): Dermatoglyphic stigmata in mongolism idiocy. Anatomical record 64: (supplement – 2): 11.
3. Cummins H. and Midlo C. (1926): Palmar and plantar epidermal ridge configurations (Dermatoglyphics) in European Americans. American Journal of physical Anthropology, 9: 471 – 502.
4. Inamdar V. V., Vaidya S. A., Kulkarni P., Devarshi D. B., Kulkarni S., Tungikar S. L. (2006) : Dermatoglyphics in carcinoma of cervix. Journal of Anatomical society of India, 55 (1): 57 – 59.
5. Jantz R. L. (1975): Population variation in asymmetry and diversity from finger to finger for digital ridge - counts. American Journal of physical Anthropology, 42 (2): 215.
6. K park (2000): Textbook of preventive & social medicine, 16th edition by m/s Banarasidas Bhanot publishers 2000, 16: 288.
7. Pal G. P., Routal R. V., Bhagwat S. S. (1985): Dermatoglyphics in the carcinoma of the cervix. Journal of Anatomical society of India, vol. 34, no. 3: 157 – 161.
8. Penrose L. S. (1969): Dermatoglyphics. Journal of Scientific American, 221: 71 – 82.
9. Reddy S. S., Ahuja Y. R., Reddy O. S. (1977): Dermatoglyphic studies in carcinoma of the cervix. Indian Journal of Heredity, 1977, 9: 35 – 40.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





