IJCRR - 5(4), February, 2013
Pages: 121-125
Date of Publication: 28-Feb-2013
Print Article
Download XML Download PDF
EFFECT OF DURATION OF EXPOSURE TO SILICA DUST ON LUNG FUNCTION IMPAIRMENT IN STONE CRUSHER WORKERS OF MARATHWADA REGION
Author: Sachin B Rathod, Smita R. Sorte
Category: Healthcare
Abstract:Silicosis is one of the oldest occupational disease. It kills thousands of people every year all over the world. It is an irreversible fibrotic process without cure and so best treatment is prevention. Prevalence of silicosis in India differs according to amount of silica in dust and time interval of exposure. Due to lack of data from Marathwada region of Maharashtra, we aimed this study to know effect of duration of exposure to silica dust in stone crusher workers. A cross-sectional type of observational study was conducted. Pulmonary function tests were recorded in 120 male stone crusher workers. Intergroup statistical analysis amongst the workers depending on duration of exposure was carried out by Analysis of Variance (ANNOVA). We found that pulmonary function test bears relationship with duration of exposure, as the duration of exposure increases the pulmonary function tests goes on decreasing.
Keywords: Pulmonary function test, stone crusher workers, silica, lung function test, silicosis, duration of exposure
Full Text:
INTRODUCTION
Today the industrial revolution has brought about the remarkable changes in ecosystem and atmosphere. The stone crushing industry in India has been growing rapidly due to increasing demand from the construction industry and present emphasis on developing the country’s infrastructure. There are more than 12,000 stone crushing units in India (1), these stone crushing units are an unorganized sector of the country. The stone contains approximately 100% free silica and the stone crushing process liberates huge amount of respirable crystalline silica dust in the working environment. (2) Exposure to crystalline silica can result in respiratory and non- respiratory health effects. The first known respiratory ill effect due to inhaled crystalline silica was reported by ancient Greek as silicosis, which is one of the oldest occupational disease and still kills thousands of people every year all over the world. Silicosis is also known as Potter's rot. The full name of illness is pneumonoultramicroscopicsilicovolcanokoniosis. Exposure to large amount of free silica can pass unseen because silica is non-irritant, odorless and does not lead to any immediate evident effect and therefore confused with ordinary dust. The inhaled silica particles are removed from the lung at a very slow rate. Thus, even if exposure is stopped the retained particles may continue to exert their effect on lung. Leigh et al have estimated an annual incidence of occupational diseases between 9, 24,700 and 19, 02,300, leading to over 1, 21,000 deaths in India. (3) Studies carried out by National Institute of Occupational Health observed prevalence of some lung diseases are 54.5% in slate pencil (4), 15.2% in Potteries (5), 38% in Agate Polishing, 21% in Stone Quarries, and 12% in stone crushing.(6) Silicosis is an irreversible fibrotic process without a cure and so treatment rests on preventing insult to the lungs. Being a respiratory ailment, this group of disorder impairs the pulmonary function tests. (7) Very few epidemiological studies on silicosis are conducted in India showing the prevalence of silicosis as 12- 54%. (3) This varying prevalence in various sectors is credited to different silica concentration in the work environment and duration of exposure to Silica dust. Till date no study has been conducted on stone crusher workers of Marathwada region to find the effect of duration on pulmonary function test. Paucity of data provides strong rationale to initiate research on the effect of duration of exposure on lung function tests in stone crusher workers of Marathwada region.
METHOD AND MATERIALS
A cross-sectional type of observational study was conducted at 7 various stone crusher units of Marathwada region of Maharashtra, between the period December 2009 to July 2011. The pulmonary function tests were carried out in 120 male stone crusher workers. Selection criteria were male stone crusher workers aged between 25-55 years, exposed to stone dust for more than 5 years, non smokers and not suffering from any chronic disease. They were divided into three groups according to duration of exposure as 5- 10yrs (51 workers), 11-15yrs (42 workers) and >15yrs (27 workers). Institutional ethics committee approval was taken. Informed consent was taken from all the workers participating in the study. Pulmonary function tests was recorded on computerized ‘MEDSPIROR’ (manufactured by Recorders and Medicare System Pvt. Ltd, Chandigarh) a high performance pneumotachometer that fulfils the criteria for performance and reproducibility laid down by American Thoracic society (ATS). All tests were performed during morning hours. The procedure of lung function tests was explained to all subjects along with demonstration prior to recording. Proper trials were given to ensure that subjects understand and become confident about the whole procedure. The reading was taken in a comfortable upright sitting position in front of the apparatus. Then each subject was asked to perform forced Expiratory manoeuvre and maximum Ventilation volume manoeuvre .(8,9) For forced expiratory manoeuvre workers was asked to take a maximum inspiration then pinch nose and expire forcefully and completely in the mouthpiece of the instrument. For maximum Ventilation volume manoeuvre workers were asked to take a maximum inspiration then pinch his nose and expire as deeply and rapidly as possible for 6 seconds in the mouthpiece. Three readings were taken and best of these was taken for calculation. Parameters considered for study was forced vital capacity (FVC -lit), forced expiratory volume in 1 second (FEV1-lit), peak expiratory flow rate (PEFR -lit/sec), maximum expiratory flow rate (FEF25-75 % - lit/sec), maximum voluntary ventilation (MVV-lit/min). Intergroup statistical analysis amongst the workers depending on duration of exposure was carried out by Analysis of Variance (ANNOVA).
RESULT
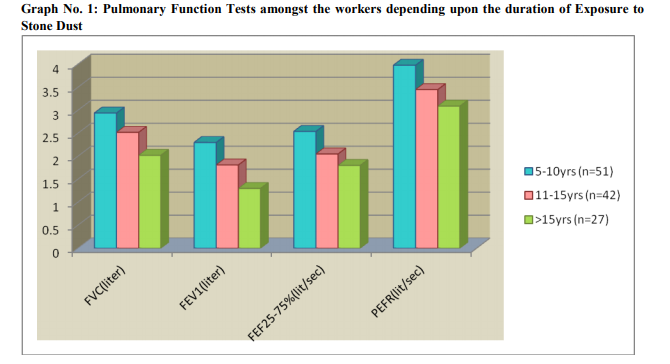
Table no. 1 and graph no. 1 shows effect of duration of exposure on pulmonary function test on stone crusher workers. Stone crusher workers were grouped into three categories depending on duration of exposure, 5-10yrs (n=51), 11-15yrs (n=42) and >15yrs (n=27). The values of FVC (P<0.001), FEV1 (P<0.001), FEV1% (P<0.001), FEF25-75% (P<0.001), PEFR (P<0.001), and MVV (P<0.001) goes on decreasing in stone crusher workers as the duration of exposure to stone dust increases.
DISCUSSION
Silica and silicates constitute the bulk of most kind of rocks, clays and sands. (10) The silica dust which is ubiquitous in atmosphere still outnumbers the other type of dust, thus making silicosis most frequently occurring pneumoconiosis. (7) Silicosis is an irreversible fibrotic process without a cure, so it should be prevented by early diagnosis. Even if the exposure to dust is stopped, the silica keeps on producing its effect. Our study was aimed to find the effect of duration of exposure on lung function tests in stone crusher workers of Marathwada region We found that as the duration of exposure to dust increases, the pulmonary function test goes on detoriating in stone crusher workers of Marathwada region Many studies are in line with our study. Ghotkar et al (11), Lious S H et al (12), Koo Jung et al (13), Subbhasini et al (14), Tiwari R et al (7), Baharami et al34 (15), Chattopadhya et al2 (16) Johncy et al (17) observed that the pulmonary function tests decline gradually with increasing duration of exposure to dust. Workers exposed to silica dust affect airway patency and lung parenchyma. Prolonged exposure to silica will aggravate all these changes in the lungs and hence all the pulmonary function tests values decreased, as the duration of exposure to silica dust goes on increasing. Decreased Fev1 and fev1% indicated obstructive changes, decreased Fev1 25-75 indicates small airway obstruction and decreased PEFR and indicates large airway obstruction. Decreased FVC indicates restrictive changes. In our study decreased values of FVC, FEV1, FEV1%, FEF25-75%, PEFR, MVV shows, mixed type of lung function impairment in stone crusher workers exposed to stone crushing dust. Hertzberg et al (18), Urom et al (19) observed restrictive type of lung function impairment. Ghotkar et al (11) concluded that obstructive type of changes was observed in quartz workers. Tiwari R et al (7), Chatopahay et al (16), Jayawardhane et.al (20) said that workers exposed to silica dust shows obstructive and restrictive type of lung function impairment. We concludes pulmonary function test bears relationship with duration of exposure, as the duration of exposure increases the pulmonary function tests goes on decreasing.

References:
1. Gottesfeld P, Nicas M, Kephart JW, Balakrishnana K, Rinehart R. Reduction of respirable silica following the introduction of water spray applications in Indian stone crusher mills. Int J occup Environ Health 2008;14(2):94-103.
2. Tiwari RR, Sathwara NG, Saiyed HN. Serum copper levels among quartz stone crushing workers: A cross sectional study. Indian J Physio Pharmacol 2004;48(3):337-342.
3. Saiyad HN, Tiwari RR. Occupational health research in India. Industrial Health 2004;42:141-148
4. Saiyed HN, Parikh DJ, Ghodasara NB, Sharma YK, Patel GC, Chatterjee SK. Silicosis in slate pencil workers: I. An environmental and medical study. Am J Ind Med.1985;8(2):127–133.
5. Saiyed HN, Ghodasara NB, Sathwara NG, Patel GC, Parikh DJ, Kashyap SK. Dustiness, silicosis and tuberculosis in small scale pottery worker. Indian J Med Res. 1995 Sep;102:138- 42.
6. An Uncommonly Diagnosed Common Occupational Disease. ICMR Bulletin 1999; 29(9). [Internet]. [Cited on 2010 Nov 21]. Available from: http://icmr.nic.in/busep99.htm
7. Tiwari RR, Narain R, Patel BD, Makwana IS, Saiyad HN. Spirometric measurements among quartz stone ex-workers of Gujarat, India. J Occup Health 2003;45:88-93.
8. A.K.Jain. Textbook of Physiology.4 ed. Avichal publishing compony; 2009. Pulmonary function tests; p.488-489.
9. P.S.Shankar. Pulmonary Function Tests in Healthy and Disease. 1st Edition 1998.
10. Kulkarni GK. Prevention and control of silicosis: A national challenge. Indian Journal of Occup Envior Med 2007;11(3):95-96
. 11. Ghotkar VB, Maldhure BR, Zodpey SP. Involvement of lung and lung function tests in Stone quarry workers. Ind. J. Tub. 1995;42:155-160.
12. Liou SH, Shih WY, Chen YP, Lee CC. Pneumoconiosis and pulmonary function defects in silica- exposed fire brick workers. Arch Environ Health 1996;51(3):227-233.
13. Koo JW, Chung CK, Chung YP, Lee SH, Lee KS, Roh YM, Yim HW. The effect of silica dust on ventilatory function of Foundry workers. J Occup Health 2000;42:251-257.
14. Subhashini AS, Satchidhanandam N. Maximal expiratory flow volume curve in quarry workers. Indian J Physiol Pharmacol 2002 Jan;46(1):78-84.
15. Bahrami AR, Mahjub H. Comparative study of lung function in Iranian factory workers exposed to silica dust. Eastern Mediterranean Health Journal 2003;9(3):390-398.
16. Chattopadhyay BP, Gangopadhyay PK, Bandopadhyay TS Alam J. Comparison of pulmonary function test abnormalities between stone crushing dust exposed and non exposed agricultural workers. Environmental Health and Preventive Medicine 2006;11:191- 198.
17. Johncy S, Ajay KT, Dhanyakumar G, Raj PN, Samuel VT. Dust exposure and lung function impairment in construction workers. J Physiol Biomed Sci 2011;24(1):9-13.
18. Hertzberg VS, Rosenman KD, Reilly MJ, Rice CH. Effect of Occupational Silica Exposure on Pulmonary function. Chest 2002;122(2):721- 728.
19. Urom SE, Antai AB, Osim EE. Symptoms and lung function values in nigerian men and women exposed to dust generated from crushing of granite rocks in Calabar, Nigeria. Nigerian Journal of Physiological Sciences 2004;19(1-2):41-47.
20. Jayawardana P, Tennakoon S, V Bandara. Respiratory symptoms and ventilatory function among granite workers working in quarries installed with mechanical crushers in and around Kandy Muncipality limits. Journal of the college of community physician of Sri Lanka 2009;13(2):9-15.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





