IJCRR - 5(7), April, 2013
Pages: 103-111
Date of Publication: 18-Apr-2013
Print Article
Download XML Download PDF
SAFETY OF BILATERAL SINGLE STAGE TOTAL KNEE REPLACEMENT UNDER ONE ANAESTHESIA IN TERMS OF PERIOPERATIVE COMPLICATIONS
Author: Shekar M., Chandrasekar C., Sharan Patil
Category: Healthcare
Abstract:Total knee arthroplasty is now the most common joint replacement procedure performed worldwide and many patients require bilateral replacement. Total knee arthroplasty can provide reliable pain relief and correction of limb alignment in patients with moderate or severe arthritis. It follows that when both knees are affected by the end stage arthritis, replacement of one of the two does not fully restore function and the patient remains significantly debilitated. The surgeon and patient are then faced with the decision of whether to proceed with a staged bilateral total knee replacement, done as two unilateral procedures performed on different days, or a single stage procedure on the same day. Our aim was to assess the safety of single stage bilateral total knee arthroplasty under one anesthetic in terms of perioperative morbidity and mortality and the clinical outcome of the procedure.Fifty patients with 100 knees were studied prospectively from the time of admission to final follow up at SPARSH Hospital, Bangalore, between July 2006 to December 2008.The average postoperative knee score at 6 th month follow up was 86.4, which has a statistical significance in terms of functional outcome . Bilateral single stage procedure has definite advantages of reducing the hospital stay and early rehabilitation of the patients suffering from severe bilateral knee arthritis.
Keywords: Bilateral, total knee arthroplasty, complications
Full Text:
INTRODUCTION
Surgical intervention for bilateral gonarthrosis can be performed either with a same day bilateral procedure or with a staged bilateral procedure requiring two separate unilateral procedures performed on different days. Bilateral total knee arthroplasty was primarily being reserved for patients thought to be at high risk for anesthesia which was expanded to include most patients with nearly equal arthritic involvement of both knees by Minter JE et al. 1 The one year mortality rate after bilateral total knee replacement is 2.7%. 2 Therefore patients undergoing bilateral total knee replacement are in general at no more risk of dying than are individuals of similar age dying of natural causes. Additionally, it is estimated that a second arthroplasty would, at a minimum, double the mortality rate associated with unilateral procedures. 2 Patients with concomitant cardiopulmonary conditions may not be good candidates for single stage bilateral procedure, as it increased the risk of cardiopulmonary complications and mortality. 3 The knee lies superficially beneath the skin and the fascial envelope and is covered by only a limited amount of well vascularized muscle as well as by a watershed area of vascular supply to the skin, which lies directly anteriorly in the position of the typical skin incision. Hence, total knee replacement has been associated with greater rate of infection. 4
MATERIALS AND METHOD
Fifty patients with 100 knees were studied prospectively from the time of admission to final follow up at SPARSH Hospital, Bangalore.
Period of study: Between July 2006 to December 2008.
Inclusion criteria
- Patients aged between 50 80 years.
- Bilateral advanced arthritis.
- ASA Grade I and II.
- Well motivated patient.
Exclusion criteria
- Age more than 80 years.
- ASA Grade III and IV.
- Uncontrolled diabetes and hypertensive with renal functional disturbances, Neuropathy.
- Presence of systemic and local infections.
- Mentally ill patients.
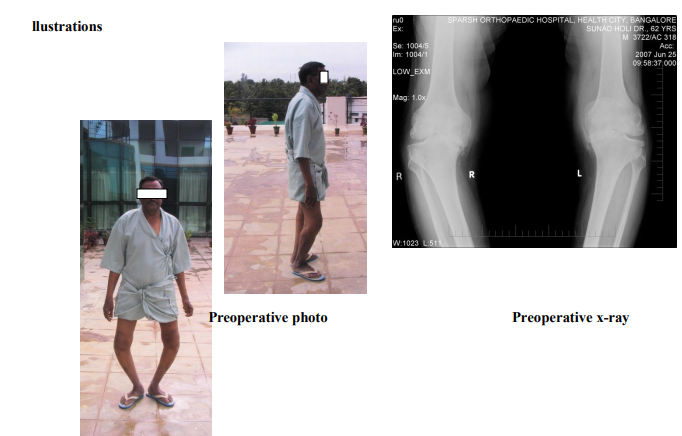
- Patients were admitted one day prior to surgery. Clinical evaluation of all the patients was done by taking complete history and examination of the knees. Standing AP and lateral views of both knees were taken. Preoperative knee scores were calculated by using modified Insall’s knee society scoring system5 which includes both subjective and functional components.
- Routine blood investigations as for any major surgery and ECG, 2D ECHO was done. Special investigations like pulmonary function tests, dobutamine stress ECHO was done in relevant cases. Preoperative photographs and videos were recorded. A preoperative checklist was prepared and followed. Proforma was prepared and applied for all the cases. The nature of bilateral total knee replacement including its need, advantages, disadvantages, outcomes and consequences were explained to the patients and their attendants and a valid informed consent was taken. Preanesthetic evaluation and fitness was obtained before the surgery.
STATISTICAL METHODS
Descriptive statistical analysis has been carried out in the present study. Results on continuous measurements are presented on Mean?SD (Min Max) and results on categorical measurements are presented in Number (%). Significance is assessed at 5% level of significance. Repeated Analysis of variance (RANOVA) has been used to find the significance of study parameters between three or more groups of patients and Student t test (two tailed, dependent) has been used to find the significance of study parameters on continuous scale with in each group. Chi square/ 3x3 Fisher Exact test has been used to find the significance of study parameters on categorical scale between two groups.
RESULTS
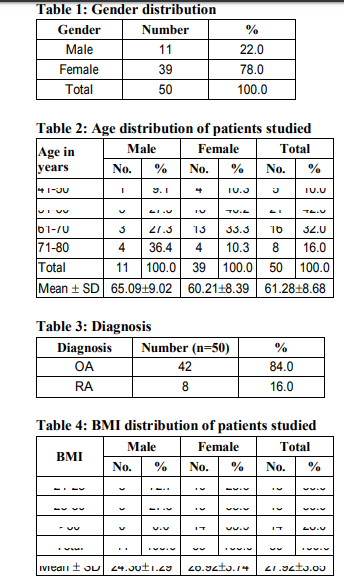
Patient demographics Thirty nine patients were females and 11 patients were males (Table 1).The average age of patients was 61.2 years (43 78 years) (Table 2). Forty two patients were suffering from osteoarthritis (OA) and 8 patients had rheumatoid arthritis [RA] (Table 3). Body mass index (BMI) distribution is as shown in Table 4. Average preoperative knee score was 29.5 (3 63). (Table 5). Average preoperative haemoglobin was 12.4g %( 10.2 15.4g %).
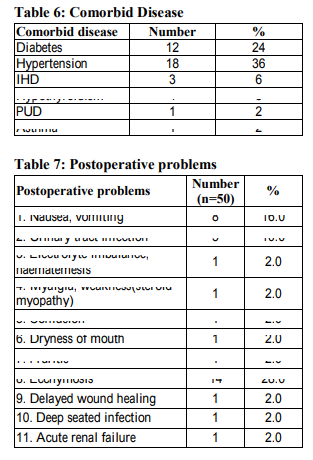
Comorbidities Twenty six patients belonged to ASA class I and twenty four patients were ASA class II. Associated comorbidities is as shown in Table 6.
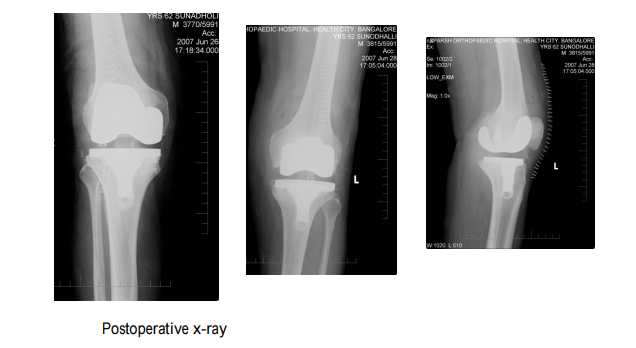
Surgical parameters Forty eight patients were operated under epidural anaesthesia and two patients under general anaesthesia. Cruciate retaining (CR) femoral prosthesis was used in 74 knees (37 patients) and cruciate sacrificing (CS) type in 22 knees (11 patients). Cruciate sacrificing rotating platform (RPF) was used in 4 knees (2 patients). Average duration of the surgery was 3 hours 50 minutes. Deep vein thrombosis (DVT) prophylaxis was not used routinely. Deep vein thrombosis prophylaxis was used in only 4 patients . One had past history of varicose veins, two were on regular aspirin and one had difficulty in early mobilization.
Duration of follow-up
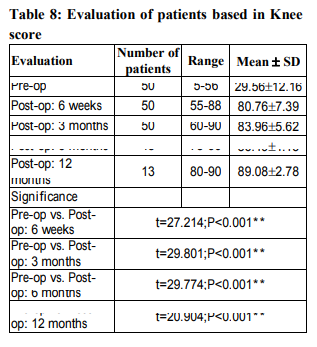
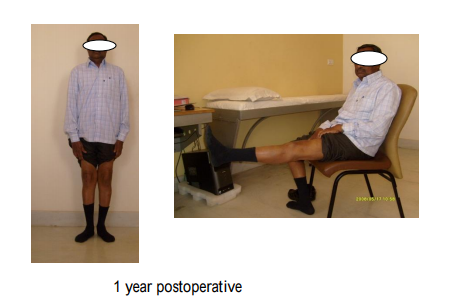
Thirteen patients had a follow up of one year or more and 37 patients were followed up for 6 months. A 70 year old lady with comorbidities such as diabetes, hypertension developed signs of acute renal failure on the same day of surgery. Later her renal parameters came to normal. Though her rehabilitation was delayed, she was able to walk well with good functional range of movements at the time of discharge. Deep seated infection was seen in one patient, who was a 72 year lady without any co morbidities. She was on intravenous antibiotics for 3 weeks, later switched over to oral for another 3 weeks. Following the revision surgery she improved well. Wound healing problem was seen in one patient, who required secondary suturing. Other minor postoperative problems are listed in the table 7. There were no deaths. None of the patients had symptoms suggestive of deep vein thrombosis, pulmonary embolism or myocardial infarction. None of the patients were readmitted within 30 days. The average duration of hospital stay was 11.6 days. The average postoperative knee score at 6 th month follow up was 86.4, which has a statistical significance in terms of functional outcome (Table 8). Immediate postoperative knee scores were low in older age group, but at 6th month follow up it was almost similar in all age groups (Table 9). Males had better functional outcome than females (Table 10).
DISCUSSION
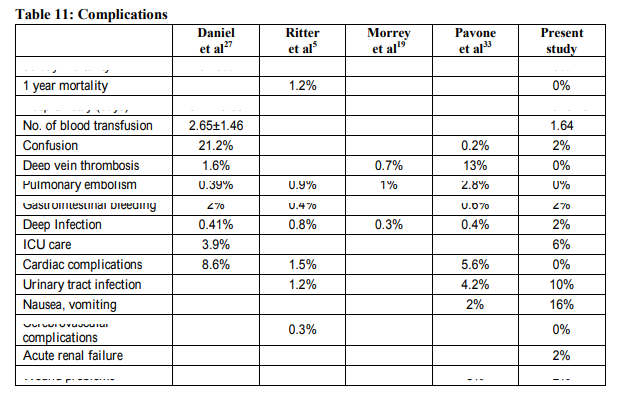
Adequate data from several sources in the literature have documented that the functional result of a single stage bilateral procedure compares favourably with the result of single procedure. Our study compares well with the already reported literature although there are certain discrepancies (Table 11). Daniel et al 6 and Lombardi et al 7 found that patients who were 80 years or more at the time of surgery, whether they underwent single stage bilateral or unilateral total knee arthroplasty, had higher rates of complications than did their younger counter parts. Pavone et al have concluded that patients belonging to ASA class I and class II had less chance of complications than ASA class III and ASA class IV in their study. These two studies prompted us to exclude patients who are more than 80 years of age and those belonging to ASA grade III and IV from this study. The expected mortality rate for an average 68 year old person is 2.3%. 9 All the procedures in the present study are done in a sequential manner. There were no mortalities in our series. Several authors have found an increased prevalence of cardiovascular complications after bilateral total knee replacement. Lynch et al 10 compared 98 matched patients over the age of 82 years who had either unilateral or single stage total knee replacement and concluded that elderly patients may not have the reserve to manage the fluid shifts that occur after a bilateral procedure. Thus elderly patients undergoing bilateral total knee replacement are at a slightly higher risk for perioperative cardiac complications. None of the patients in the present series had cardiovascular complications. Fat emboli secondary to the release of marrow contents from the intramedullary canals of the femur and the tibia have been described after bilateral total knee replacement. 11,12 One of our patients had significant postoperative confusion which prompted us to think of possible fat embolism phenomenon but it resolved completely on oxygen supplementation. After bilateral total knee replacements patients have a considerable risk of thromboembolic complications. Soudry et al 13 , who evaluated 304 patients and reported a twofold increased relative risk of deep vein thrombosis in the cohort treated with unilateral arthroplasty. Chemoprophylaxis for deep vein thrombosis is not routinely used in our practice. We restrict its use to patients at high risk for deep vein thrombosis. These patients generally would fall into ASA grades III and IV and hence were excluded from this study. However, four patients in this study received chemoprophylaxis. One had calf pain and tenderness in the postoperative period. Doppler studies ruled out measurable deep vein thrombosis for this patient, but chemoprophylaxis was started and continued till the patient was mobilized independently. One had past history of varicose veins and the remaining two were on regular aspirin. Mechanical measures such as early ambulation, compression stockings/bandages were routinely used in all patients. However, calf/foot pump was not used in this series. The routine use of indwelling epidural analgesia may also be one of the contributing factor for reduced incidence of deep vein thrombosis in this study. While successful total joint replacement offers dramatic and lasting improvement in the quality of life, deep infection is the most feared complication of this procedure as it threatens the function of the joint, the preservation of the limb, and occasionally even the life of the patient. 4 Most of the authors also believe that reduced duration of surgery and using separate sterile set of instruments for the other knee may reduce chance of infection. We had one deep infection in our series. Lynch et al 10 have shown the occurrence of renal failure in 3 patients out of 98 following bilateral total knee replacement and 2 patients out of 98 following unilateral total knee replacement. Most of the studies show that the rate of requirement of blood transfusion following bilateral single stage total knee replacement is more when compared to unilateral total knee replacement. The average requirement of number of blood units was 2.65 according to Daniel et al. 2 The average requirement of number of blood units in this study is 1.64. The number of patients requiring more than three units of blood in this series was 4%. There has been marked decline in the hospital stay and rehabilitation time for patients having bilateral knee replacements. The overall hospital stay has decreased from one month in the early studies 13,14 to less than 10 days in the more recent literature. 15,16
SUMMARY AND CONCLUSIONS
Bilateral single stage total knee replacements were carried out for 50 patients in this study under a single anesthesia. All the patients were operated by the same surgical team, using standard surgical technique. Postoperative rehabilitation was carried out according to standard protocol. We had four major complications, which includes one deep infection, one acute renal failure, one peptic ulcer disease and one steroid induced myopathy. These were treated accordingly. We also had minor complications such as nausea, vomiting and urinary tract infection in few patients. There was no mortality and no cardiovascular and thromboembolic complications in our series. The average duration of hospital stay was 11.6 days. The mean postoperative knee scores were 86 at th month and 89 at 12 th month follow up, which has statistical significance. Our results are very well comparable with the already reported series. We had few perioperative complications. Major complications in our series including deep infection and acute renal failure were seen in patients who were more than 70 years old. Hence, it may be prudent to think that Indian patients who are more than 70 years age may not be good candidates for single stage procedures. This also correlates with some of the earlier reports. Bilateral single stage procedure has definite advantages of reducing the hospital stay and early rehabilitation of the patients suffering from severe bilateral knee arthritis. It should be emphasized, however, that, as with any surgical procedure, the ultimate result will depend in large part on the expertise of the surgeon and the established pattern of preoperative medical clearance and postoperative management. When the surgeons are experienced in replacement of the knee and have adequate operating room support and assistance, we think that the obvious social and economic advantages of bilateral single stage knee replacement can be offered without compromising the patient’s functional result or increasing the risk of complication or death.
References:
1. Minter JE, Dorr LD. Indications for bilateral total knee replacement. Contemp Orthop 1995; 31: 108 111.
2. Daniel P. Bullock et al. comparision of simultaneous bilateral with unilateral total knee arthroplasty in terms of perioperative complications. J Bone Joint Surg 2003 Oct; 85 A (10): 1981 1986.
3. Camilo Restrepo et al. Safety of simultaneous bilateral total knee arthroplasty A meta analysis. J Bone Joint Surg Am 2007 Jun; 89: 1220 1226.
4. Ayers, David C et al. Common complications of total knee arthroplasty. J Bone Joint Surg Am 1997 Feb; 79 A (2): 278 311.
5. Insall JN, Dorr LD et al. Rationale of the knee society clinical rating system. Clin Orthop 1989; 309: 102 109.
6. Daniel A. Oakes et al. Bilateral total knee replacement using the same anesthetic is not justified by assessment of the risks. Clin Orthop 2004 November; 428: 87 91.
7. Lombardi AV et al. Simultaneous bilateral total knee arthroplasty: Who decides? Clin.Orthop 2001; 392: 319 329. 8. Vito Pavone et al. Perioperative morbidity in bilateral one stage total knee replacements. Clin Orthop 2004 April; 421: 155 161.
9. National Center for Health Statistics. U. S. decennial life tables for 1989 91. Hyattsville: US Department of health and Human services; 1997: 98 1150.
10. Lynch, Nancy M. Trousdale, Robert T. Ilstrup, Duane M. Mayo Clinic Proceedings, 1997 Sept; 72(9): 799 805.
11. George T. Kolettis et al. Safety of 1 stage bilateral total knee arthroplasty. Clin Orthop 1994; 309: 102 109.
12. Dorr LD et al. Fat emboli in bilateral total knee arthroplasty: Predicting factors for neurologic manifestations. Clin Orthop 1989; 248: 112 118.
13. Michael Soudry et al. Succesive bilateral total knee replacement. J Bone Joint Surg 1985 Apr; 67 A (4): 573 576.
14. Ernest L. Gradillas et al. Bilateral total knee replacement under one anesthetic. Clin Orthop 1979May; 140: 153 158.
15. Worland RL et al. Simultaneous bilateral total knee replacement versus unilateral replacement. Am J Orthop 1996; 25: 292 295.
16. Lane et al. Simultaneous bilateral versus unilateral total knee arthroplasty: Outcomes analysis. Clin Orthop 1997; 345: 106 112.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





