IJCRR - 5(7), April, 2013
Pages: 98-102
Date of Publication: 18-Apr-2013
Print Article
Download XML Download PDF
RARE DUPLICATION OF URETERS - LEFT SHOWING TWO DIVISIONS AND RIGHT SHOWING FOUR DIVISIONS WITH ANOMALOUS RIGHT KIDNEY
Author: Prabhakaran Kattimuthu, Manish Lamoria, Ankur Prahalad Bhai Patel, Rupesh Kumar
Category: Healthcare
Abstract:Embalmed cadavers were dissected as a part of medical undergraduate curriculum; any Unusual or Rare variations/ congenital anomalies were noted and photographed. Rare Duplication of Ureters \? Left showing Two Divisions and Right showing Four Divisions with Anomalous Right Kidney were noted. Varieties of congenital Anomalies associated with ureters are of importance to surgeons, Urologist and Gynecologists. Knowing common and rare variations of normal Anatomy helps to avoid undue complications during surgical procedure. Knowledge of Rare variations/congenital anomalies helps to understand the development of the particular structure better including their molecular regulations.
Keywords: Duplicated ureters, Anomalous Kidney
Full Text:
INTRODUCTION
Duplication of ureter results from early splitting of the ureteric bud (Sadler1 2006, Moore2 2008, Schoenwolf3 2009).Incidence of duplex ureters, that is two ureters on one side, is 1 in 125 individuals (Standring4 2005) where as incidence of the same bilaterally is 1 in 800 individuals (Standring4 2005).Varieties of congenital Anomalies associated with ureter are of importance to surgeons, Urologist and Gynecologists. Knowing common and rare variations of normal Anatomy helps to avoid undue complications during surgical procedure. Also knowledge of congenital anomalies helps to understand the development of the particular structure better.
MATERIALS AND METHODS
20 embalmed cadavers (cadavers were embalmed using standard embalming fluid containing formalin by gravity method and stored in formalin tanks) were dissected as a part of medical undergraduate curriculum in the dissection hall which is well ventilated and well illuminated. Conventional dissection methods using usual dissection instruments (scalpel, forceps, and scissors) were used following instructions of dissection manual (Romanes5 2004) layer by layer under daylight. Any unusual or rare variations/anomalies of the urinary system were noted and studied in detail. Blunt dissection was employed once rare variations/anomalies were detected in order to avoid any damage to the structures. Finally the dissected viscera were photographed using Kodak digital Camera 8.2 Megapixels in both anterior and posterior views.
OBSERVATIONS AND RESULTS
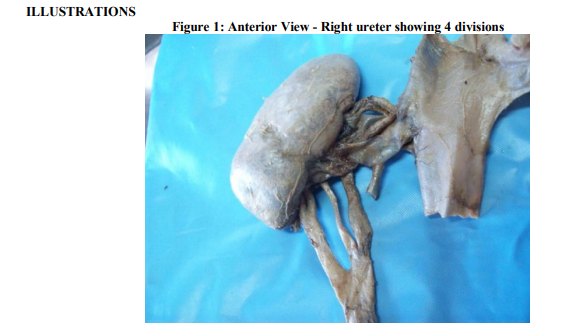
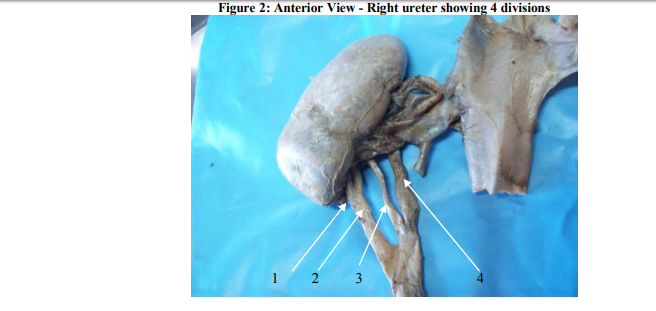
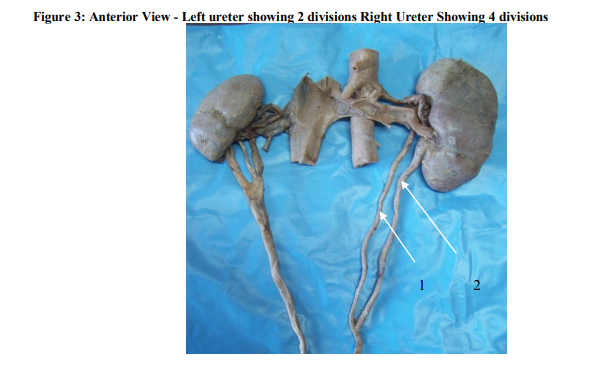
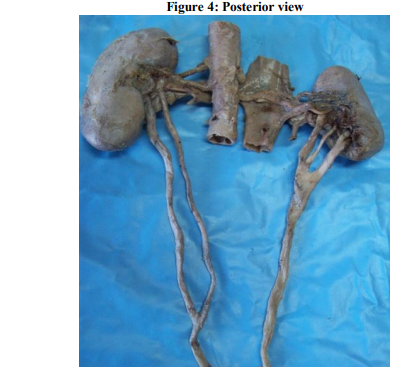
During cadaveric dissection interesting and rare duplication of ureters on both the right and left side were noted in a male cadaver aged around 60years. (Fig. 3 and 4).The right ureter showed 4 divisions which were partial since all the 4 divisions united soon (Fig. 1and2). Also the right kidney was much smaller in size compared to the left and was only one third -1/3rd the size of a normal kidney (Fig. 3 and 4). The left ureter showed 2 divisions which were once again partial as they united after some distance. Both the right and left ureters opened normally in to urinary bladder. DISCUSSION The ureteric bud develops from the mesonephric duct very close to its entry in to cloaca (Sadler1 2006, Moore2 2008, Schoenwolf3 2009, Standring4 2005). Ureteric bud further develops in to the collecting system and metanephric tissue cap surrounding the ureteric bud develops in to the excretory system. Duplication of ureter results from early splitting of the ureteric bud (Sadler1 2006, Moore2 2008, Schoenwolf3 2009). Incidence of duplex ureters that is two ureters on one side is 1 in 125 individuals (Standring4 2005) where as incidence of the same bilaterally is 1 in 800 individuals (Standring4 2005). Partial duplication of ureters is where the duplicated ureters unite and open as a single structure in to the urinary bladder (Sadler1 2006). Complete duplications are where the duplicated ureters open separately/independently in to the urinary bladder (Sadler1 2006). Many genes are involved in the differentiation of kidney .One of the important Genes Involved in the Differentiation of the kidney –WT1 expressed by the mesenchyme surrounding the ureteric bud that is metanephric tissue caps enables it to respond to induction by the ureteric bud (Sadler1 2006). Due to defect in the WT1 Transcription factor the metanephric tissue cap surrounding the ureteric bud has failed to respond to the induction by the ureteric bud. As a result on the right side the metanephric blastema has not developed completely resulting in anomalous or under developed right kidney. The 4 divisions of the ureter on the right side which unite shortly after some distance from the kidney could be the major and minor calyces, uniting to form the renal pelvis lying outside and at a lower level than the normal location due to underdeveloped or anomalous right kidney.
CONCLUSION
Rare duplication of ureter – Left showing two divisions and right ureter 4 divisions with anomalous right kidney. Due to defect in the WT1 Transcription factor the metanephric tissue cap surrounding the ureteric bud has failed to respond to the induction by the ureteric bud. As a result on the right side the metanephric blastema has not developed completely resulting in anomalous or under developed right kidney. The 4 divisions of the ureter on the right side which unite shortly after some distance from the kidney could be the major and minor calyces, uniting to form the renal pelvis lying outside and at a lower level than the normal location due to underdeveloped or anomalous right kidney. Different Varieties of congenital Anomalies associated with ureters are of importance to surgeons, Urologist and Gynecologists. Knowing common and rare variations of normal Anatomy helps to avoid undue complications during surgical procedure. Also knowledge of congenital anomalies helps to understand the development of the particular structure better including their molecular regulations.
ACKNOWLEDGEMENT
Authors acknowledge the great help received from the scholars whose articles cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. Authors are grateful to IJCRR editorial board members and IJCRR team of reviewers who have helped to bring quality to this manuscript.
DECLARATION
The manuscript represents valid work and that neither this manuscript nor one with substantially similar content under the present authorship has been published or is being considered for publication elsewhere and the authorship of this article will not be contested by anyone whose name (s) is/are not listed here, and that order of authorship as placed in the manuscript is final and accepted by the co-authors.
References:
1. Sadler, T.W., Langman’s Medical Embryology, 10th ed.Lippincott Williams and Wilkins, 2006; P 233-235
2. Moore, K.L., Persaud, T.V.N., The Developing Human Clinically oriented Embryology, 8th ed. Saunders ELSEVIER, 2008; P 255
3. Schoenwolf ,G.C., Bleyl, S.B., Brauer, P.R., Francis, P.H., Larsen’s Human Embryology, 4 th ed. Churchill Livingstone ELSEVIER , 2009; P 497
4. Standring, S., Ellis, H., Healy, J.C., Johnson, D., Williams, A., Gray’s Anatomy the Anatomical basis of clinical practice, 39th ed. Churchill Livingstone ELSEVIER, 2005; P1285
5. Romanes, G.J., Cunningham’s Manual of practical Anatomy, 15th ed.Oxford medical Publications, 2004; Vol. II., P 165.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





