IJCRR - 5(8), April, 2013
Pages: 79-83
Date of Publication: 25-Apr-2013
Print Article
Download XML Download PDF
PREVALENCE AND DETERMINANTS OF DISABILITIES IN RURAL ELDERLY IN CHITTOOR DISTRICT, ANDHRA PRADESH
Author: Swarnalatha N.
Category: Healthcare
Abstract:Similar to developed countries, aging was increased in India. Because of epidemiology and demographic transition phase, chronic diseases and disabilities were increasing. Socio-economic factors and chronic diseases were the major reasons for geriatric disability. There is a dearth of community based studies from India for geriatric disabilities and its associated risk factors; the present study was undertaken with the following objectives. Study objectives: To determine the prevalence of disability and its association with the age, gender and other selected variables in a rural geriatric population. Study design: cross-sectional, observational community based study. Study Period: April 2009 to September 2009. Study Setting: Villages covered under Rural Health Centre, which is a rural field practice area, attached Community Medicine department, S.V. Medical College, Tirupati. Study Subjects: 400 individuals aged 60 years and above of both sexes equally were interviewed by house-to-house visits. Study Method: Study subjects were selected by random sampling technique. Study was conducted by house-to-house visits. Clinical examination, observation and interview were conducted with a pre-designed and pre-tested proforma. Sample Size: 400. Study analysis: The data are analysed statistically using SPSS software 17 version. Results: The prevalence of disability was 70%. Most prevalent disability was vision (63.5%). The disability prevalence was high among 80 years and above elderly and it was increasing with age. The prevalence of disability was high among males (69.5%) than females (70.5%). In present study 46.5% elderly having one disability. Age, literacy, marital status and cognitive impairment were having statistical significant association with the disability.
Keywords: Geriatric population, disability, rural area.
Full Text:
INTRODUCTION
India is the 2 nd largest country in the world in terms of geriatric population. The proportion of elderly persons in Indian population is increasing as a result of many contributing factors i.e., a significant decline in birth rate, increase in life expectancy due to advancement in medical treatment and technology, prevention and eradication of many infectious diseases and improved nutrition, hygiene and sanitation. Though there is increased life expectancy, the health conditions of the people in their late stage have been observed to be worsening. Illness and injuries along with degeneration of body organs result in hospitalization or decreased activity, which may subsequently lead to disability or dependency. Disability is found to be major health concern among the elder people as it seriously affects the economic, social and psychological aspect of life. There are discussions about vulnerable groups like women, schedule castes and tribes etc. Elderly is another important group which need attention because of their increasing number. The incidence of disabilities is higher in developing countries than in the industrialized countries. Disabled individuals in the community face many social problems. They are perceived only in the light of their infirmities. There are a number of studies that look at the health conditions of elderly in developing countries. Though disability is the commonest problem, there are very few community based studies that look into the elderly disability pattern in India. Interestingly, most of the studies focus on the disability patterns of the younger population. However, there is very little information about gender differentials in disability among the elderly in developing countries, like India. Little is known about association of disabilities among elderly with gender, marital status, living arrangements etc. No similar study had been conducted in the past among geriatric population in Chandragiri, a rural area of Chittoor district. Considering this background, the present study was initiated in rural area of Chittoor district with the following objectives
1) To assess the prevalence of disability among 60 and above age group.
2) To find out the association of disability with age, gender and other selected variables in a rural elderly population.
MATERIAL AND METHODS
A community based cross sectional study was conducted from April2009 to September 2009 in rural field practice area of Rural Health Centre, Chandragiri, Chittoor district which is a field practice area of Sri Venkateswara Medical College, Tirupati. To draw a simple random sample with 10% of non respondents, approximately 400 subjects (aged 60 years and above) of both sex was included in the study. Data were collected from the study population by house to house visits using a pre designed, pre tested proforma after taking a verbal consent. Predictor variables included were socio demographic variables such as age, gender, literacy status, occupation, marital status, type of family, living status, socio economic status, status in the family, economic dependency, addiction, cognitive impairment and depression. Outcome variable was disability. Socio economic status was classified according to Aggarwal classification . Folstein’s Mini Mental Status Examination (MMSE) questionnaire was used to assess the cognitive status and Yesavage’s Geriatric Depression Scale (GDS) – Shorter version was used to detect depression status of the study subjects. Data was analysed using SPSS 17 version and the results were recorded as frequencies, percentages. The tables were used for comprehensive viewing of the results. The chi square test was used whenever necessary. Value < 0.05 was taken as criteria for significance for all purposes. Binary logistic regression analysis with significance was also done.
RESULTS
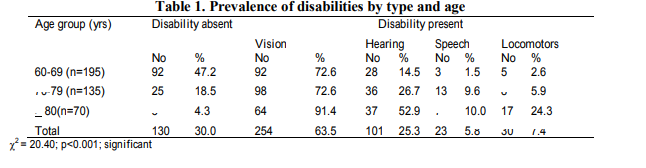
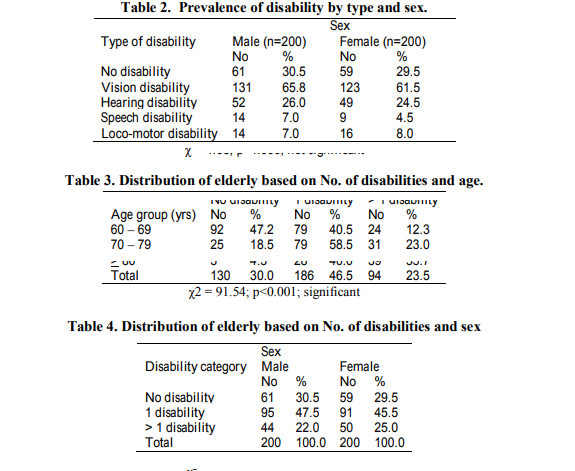
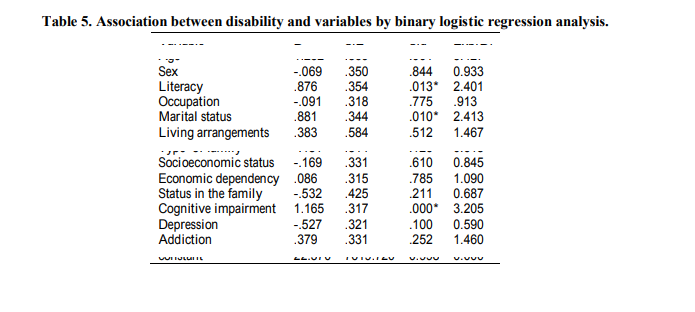
In current study prevalence of disability was 70.0% (Table1). The prevalence of various types of disabilities was found to increase with age and the differences were statistically significant. Most prevalent disability was vision (63.5%) followed by hearing (25.3%), loco motor disabilities (7.4%) and speech (5.8%). Prevalence of various types of disabilities was found to be more or less similar in both males and females and it was not statistically significant (Table 2). 46.5% elderly having 1 disability while 23.5% were having more than 1 disability. Proportion of subjects having more than one disability was increasing with age and it was statistically significant (Table 3). The prevalence of having one or more than one disability was found to be high in females (70.5%) compared to males (69.5%). However, the difference was not statistically significant (Table 4). Association of different socio demographic characteristics, economic dependency, status in the family, cognitive impairment and depression with disability was analyzed by binary logistic regression (Table 5). Among these variables age, literacy, marital status and cognitive impairment were significantly associated with disability.
DISCUSSION
The prevalence of disability in current study was 70%. Joshi et al found that 87.5% elderly had minimal to severe disabilities . Mangalore study showed the disability prevalence as 65.8% . Venkata Rao et al and Krishnamachari Srinivasan studies revealed the disabilities prevalence as 74.12% and 58% respectively 6, 7 . In North Indian study the prevalence of various impairments was 48% . The present showed variation in prevalence of disability among geriatric population in comparison to other studies. This may be due to methodological reasons. The prevalence of disability was increasing with age and it was statistically significant. Many studies related to disability among elderly have confirmed that increasing age tend to be associated with increased risk of disability 5, 6, 8, 9 . The prevalence of disability was high among males (69.5%) than females (70.5%) and it was not statistically significant. In current study 63.5% elderly having vision disability which was a major disability. Venkata Rao et al and Grover et al studies revealed vision disability as 56% and 69% respectively 6, 10 . In present study, cataract was observed to be responsible for visual disability. The prevalence of visual impairment in the present study was found high among males than females. The reason was probably due to tendency of early health seeking behaviour in men as compared to women. In present study hearing impairment was 25.3%. Various studies in India showed prevalence of hearing impairment ranging from 22% to 43.3% 10, 11 . Even higher prevalence of hearing impairment (46%) was reported by Vijaya Kumar 12 Earlier population studies from India have reported that impairment in hearing and visual functions as important causes of disablement in the elderly 13 . Similar findings were observed in current study. In present study loco motor disability was 7.4%. Goswami et al study reported loco motor disability as 11% in the elderly, without much difference in any gender . Speech disability in present study was 5.8% and Venkata Rao et al study revealed speech disability as 4% In present study 46.5% elderly having one disability while 23.5% were having more than one disability. Venkata Rao et al and Goswami et al studies revealed that 74.12% and 48.0% of the aged population were having at least one disability repectively 6, 8 . In present study the proportion of persons having one or more than one disabilities increased with the age. Present study found that age, literacy status, marital status, cognitive impairment was significantly associated with disability (binary logistic regression analysis). Similar association was also reported in different studies 14, 15 . Similar to current study, Italy showed that cognitive impairment is a more powerful predictor of impaired functional activities than disease burden 16
CONCLUSION
Disability is an important health problem among elderly in rural area of India. There is need to provide appropriate awareness, comprehensive and accessible services, so as to enable the elders to realize their full potential and lead a comfortable, healthy and happy life. The mobile health clinics equipped with these facilities may be a solution.
ACKNOWLEDGMENTS
I thank all the study participants and their families for their cooperation during the study period. Author acknowledges the great help received from the scholars whose article cited and included in references of this manuscript. The author is also grateful to authors/editors/publishers of all those articles, journals from where the literature for this article has been reviewed and discussed. Author is grateful to IJCRR editorial board members and IJCRR team of reviewers who have helped to bring quality to this manuscript.
References:
1. Aggarwal OP, Bhasin SK, Sharma AK, Chabra P, Aggarwal K, Rajoura OP. A socioeconomic status of a family: Preliminary study. Indian Journal of Community Medicine 2005; 30(4): 111 14.
2. Folstein MF, Folstein SE and Mc Hugh PR. “Mini Mental State”. A Practical method for grading the cognitive status of patients for the clinicians. Journal of psychiatric Research 1975;12:189 98.
3. Yesavage JA. Geriatric depression scale (Short version). Psychopharmacology Bulletin 1998;24:709 11.
4. Joshi K, Kumar R, Avasthi A. Morbidity profile and its relationship with disability and psychological distress among elderly people in Northern India. International Journal of Epidemiology 2003;32:978 87.
5. Ganesh KS, Yadav A, Sajjan BS and Kotian MS. Epidemiology of disability among geriatric population in the semi urban area of Mangalore city, Karnataka. Indian Journal of Gerontology 2008;22(1):35 42.
6. Venkatarao T, Ezhil R, Jabbar S, Ramakrishnan R. Prevalence of disability and handicaps in geriatric population in rural South India. Indian Journal of Public Health 2005;49(1):11 7.
7. Krishnamachari Srinivasan, Mario Vaz and Tinku Thomas. Prevalence of health related disability among community dwelling urban elderly from middle socioeconomic strata in Bengaluru, India. Indian J Med Res 2010;131:515 21.
8. Goswami A, Reddaiah VP, Kapoor SK et al. Prevalence and determinants of disability in the rural elderly population in Northern India. Indian Journal of Physical Medicine and Rehabilitation 2005; 16:39 44.
9. Dhar HL. Emerging Geriatric Challenge. JAPI 2005;53:867 71.
10. Grover V, Aggarwal OP, Tiwari RS, Markandey N. Prevalence of health problems among the elderly in rural areas of Delhi. Indian J Preventive Social Medicine 2000; 31:47 51.
11. Dr. Chandra Paul Singh. Socio economic status and health conditions of landless rural aged in Haryana. Help Age India Research and development Journal 2005; 11:7 15.
12. Vijaya Kumar S. Rural elderly health status and available health services. Help Age India Research and development Journal 1996; 2:16 22.
13. Venkoba Rao A. The health care of the rural aged – kallandiri experience. Indian Journal of Social Psychometry 1997; 298.
14. Fuller Thomson E and Minkler M. Functional limitations among older American Indians and Alaska natives. Findings from the census 2000 Supplementary survey. American Journal of Public Health 2005;95:1945 48.
15. Hayward MD and Heron M. Racial inequality in active life among adult Americans. Demography 1999; 36:77 91.
16. Scalan JM, Binkin N, Michieletto F, Lessig M, Zuhur E, Borson S. Cognitive impairment, chronic disease burden and functional disability: a population study of older Italians. Am.J geriatr psychiatry 2007; 15:716 4.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





