IJCRR - 8(24), December, 2016
Pages: 06-12
Print Article
Download XML Download PDF
A STUDY ON THE PREVALENCE OF NUTRITIONAL PROBLEMS OF SCHOOL GOING ADOLESCENT GIRLS OF KASHMIR VALLEY WITH SPECIAL FOCUS ON ANEMIA
Author: Darakshan Ali, Anjum Fazili, Rohul Jabeen Shah, Mir Mohammad Rafiq
Category: Healthcare
Abstract:Background: In India adolescents constitute about 22.8% of total population forming a significant proportion of the population [3].Nutrition is an important area of concern in adolescent health especially in girls. Improper nutrition in girls has been shown to lead to adverse intergenerational effects. Aims and Objectives: To identify the nutritional problems of school going adolescent girls of Kashmir Valley and to study the factors associated with anemia in these girls. Methodology: A cross sectional study design was adopted and the study was conducted in randomly selected schools in three districts of Kashmir Valley. A total of 428 girls in the age group of 12 to 18 years were included in the study. Data was collected using a pre-tested and pre-structured questionnaire which included assessment of the dietary habits, anthropometric measurements and general physical examination of the study population. Hb estimation of a subset of the study population was also done. Data was analyzed using SPSS 20.0. Results: It was seen that anemia was the most common nutritional problem in the adolescent girls seen in 53.30% of them followed by thinness in 35.70% of them [7] Other problems seen were overweight, obesity and thyromegaly.
Conclusion: Thus it is concluded from this study that a considerable proportion of adolescent girls suffered from nutritional problems which need to be addressed in order to improve the overall health status of these girls.
Keywords: Adolescents, Nutrition, Thinness, Overweight, Anemia
Full Text:
INTRODUCTION
The term "adolescence" is derived from the Latin word "ADOLESCERE" meaning "TO GROW" or "TO MATURE". WHO defines adolescence as the segment of life between the ages of 10 to 19 years. Adolescence is one window of opportunity which can be used effectively to inculcate good practices in individuals and hence in community [1].
Adolescents constitute about 20% of the total world population [2]. In India adolescents constitute about 22.8% of total population which in absolute numbers is approximately 273 million forming a significant proportion of the population[3].The importance of adolescents lies in the fact that they are going to be the adults of tomorrow and the future development of a nation rests in large part on the prospect of having adults who are educated, healthy and economically productive[2].
Nutrition is of importance especially in adolescent girls where malnutrition, anemia and stunting could have adverse intergenerational effects. Micronutrient deficiency is also seen in a significant number of adolescents. There is also increasing evidence that overweight and obesity is confined not only to adults but also being reported among the children and adolescents perhaps due to changing lifestyles.
In order to deliver health care services to adolescents it is important to know what the health problems and needs of these adolescents are. Our study aims to help planners and policy makers to provide services relevant to the needs of adolescents.
MATERIAL AND METHODS
OBJECTIVES
- To identify various nutritional problems of school going adolescent girls of Kashmir Valley.
- To identify various factors associated with anemia in these girls.
- To recommend measures for prevention and control of anemia.
METHODOLOGY
A cross sectional study design and multistage random sampling technique was used and the study was conducted in 18 Girls schools selected randomly from three districts of Kashmir Valley.
The calculation of required sample size was carried out using prevalence (p) as 50% and an allowable error of 5% and using the formula:
n= Z2p(1-p)/e2
n= estimated sample size
p= expected prevalence
Z= statistic for 95% level of confidence (1.96)
e= allowable error
Thus the sample size was 422 including a 10% for non-responders. To round off, a sample size of 450 was taken (including a margin of 10% for non-response rate)[7].
One district was selected from each of the three geographical regions of Kashmir valley. Since the enrolment ratio of school going adolescent girls in the age group of 12-18 years in urban and rural areas of Kashmir Valley is 1.07:1 [4], the calculated sample size was divided in the ratio of 1.07:1 between the selected urban and rural districts of Kashmir[7].
The study was conducted in a total of 18 schools. The number of students to be taken from each school and class was calculated on the basis of Probability Proportional to Size (PPS) technique. Adolescent girls aged 12-18 years who gave consent/whose parents gave consent to be a part of this study was included in the study[7].
ETHICAL ISSUES:
Ethical clearance was sought from the Institutional Ethics Committee. Besides this, proper permission was taken from Director School Education, Kashmir and concerned Chief Educational Officers of all the three districts as well as from the school authorities. Informed consent was taken from parents of the students. Consent was taken from the student as well. Confidentiality was maintained at all times and girls in need of medical attention were appropriately referred[7].
TOOLS FOR DATA COLLECTION:
Data was collected using a pre tested and pre structured proforma which included questions on social and demographic particulars and questions on diet and physical activity and a thorough clinical examination and anthropometry was also done.
The study population was categorized as thin, overweight and obese on the basis of BMI for age as per WHO growth reference values[5] and they were also categorized on the basis of Waist-hip ratio[6] as overweight and obese.
Micronutrient deficiencies included anemia which was assessed clinically and using laboratory investigation (Hb estimation) of a subset of the study population. Assessment of Iodine deficiency was done clinically based on the presence of thyromegaly.
Hemoglobin estimation was done on 50% of the study population which were selected by systematic random sampling.
DATA ANALYSIS:
Data was analyzed using SPSS version 20.00. A p value of ≤ 0.05 has been considered significant.
RESULTS
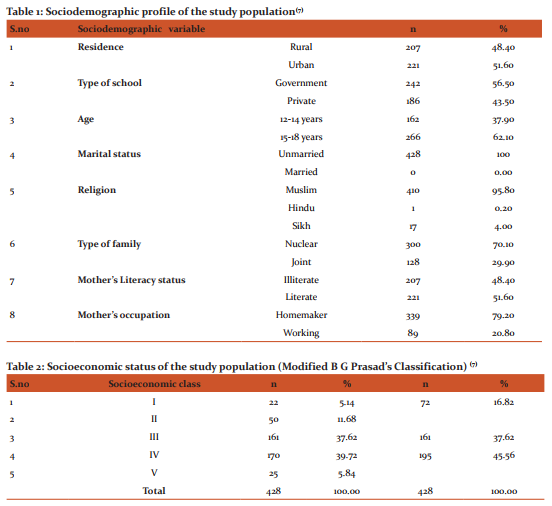
Table 1depicts the socio-demographic profile of the study population. It was observed that 48.40% of the adolescents belonged to a rural area while as 51.60% belonged to urban background. 37.90% study population was in the age group of 12-14 years and 62.10% were in the age group of 15-18 years. It was observed that almost all i.e. 95.80% participants were Muslims. (70.10%) participants came from nuclear families and 128 (29.90% ) came from joint families. It was seen that 48.40% participants had illiterate mothers and 51.60% had literate mothers and 79.2%had mothers who were homemakers and 20.80% had working mothers [7].
Table 2 depicts the distribution of study population on the basis of their SES. SE classes I and II have been grouped together and considered as upper class, SE class III considered as middle class and SE classes IV and V together considered as lower SE class. It was observed that 45.56% of the study population belonged to lower SE class followed by 37.62% belonged to middle class and 16.82% belonged to upper SE class [7].
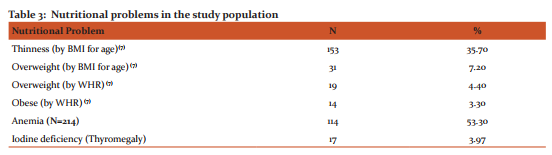
Table 3 depicts the prevalence of various nutritional problems in the study population. Most common nutritional problem encountered was anemia seen in 53.30% of the adolescent girls.
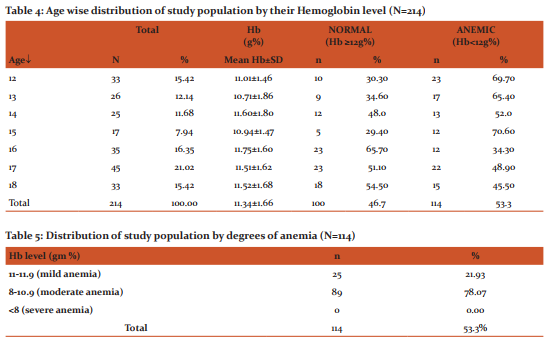
Table 4: This table depicts the age wise distribution of study population by their mean Hb level (81). The mean Hb level of the study population was 11.34+1.66g% . The overall prevalence of anemia was 53.3% , with highest prevalence seen at 15 years of age (70.6% %) and lowest at 16 years of age (34.3%).
Table 5: Out of the 114 anemics detected, 25 (21.93% ) were mildly anemic and 89 (78.07% ) had moderate anemia. However none of the adolescent girls was severely anemic.
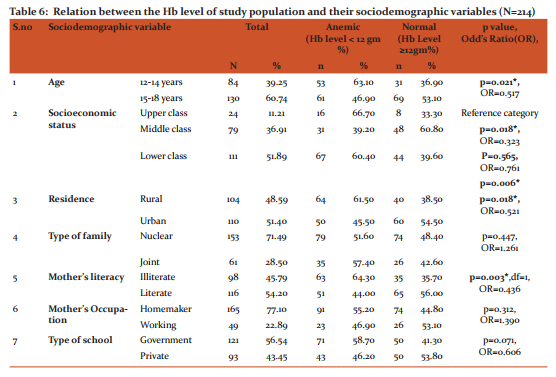
Table 6 depicts the relation between Hb level and sociodemographic variables of the study population. It was seen that the prevalence of anemia in the study population in the age group 12-14 years was significantly higher than in 15-18 years of age group (p=0.021). Also the prevalence of anemia in upper SE class was significantly higher than that in middle class (p =0.018). The prevalence of anemia among study participants from rural background was significantly higher than those from urban background (p = 0.018). Also the prevalence of anemia was significantly higher in study population whose mothers were illiterate than those with literate mothers (p==0.003).
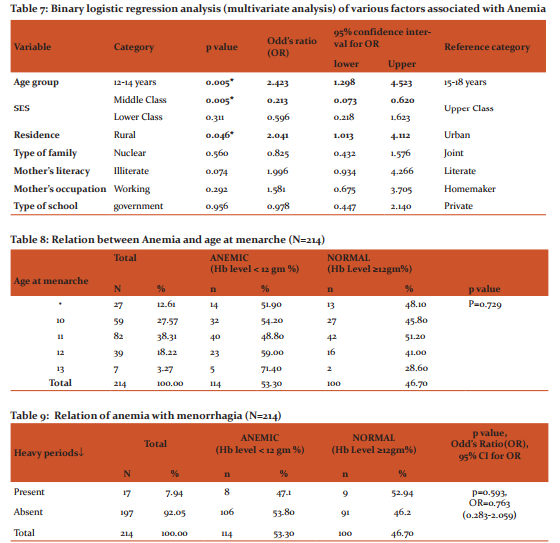
Table 7: On binary logistic regression analysis (multivariate analysis) the prevalence of anemia correlated strongly with Age, SES and residence of the adolescent.
Table 8 depicts the relationship of prevalence of anemia in study population with age at menarche. The association was not statistically significant (p 0.729).
Table 9 depicts the relation of anemia with heavy menstrual periods. The association of the prevalence of anemia and heavy menstrual periods was not statistically significant.
Discussion
The present study revealed that overall prevalence of thinness in the study population was 35.70% [7]. Anand K. et al observed almost a similar prevalence (30.1% ) of thinness in north Indian rural school going girls near Delhi [2]. A higher prevalence of thinness among adolescent girls was observed by Wasnik V et al in Andhra Pradesh (56.4% ) [8].
The prevalence of over-weight in the present study was 7.20 as per BMI for age[7]. Omobuwa O et al in their study on in- school adolescents in Nigeria found that 7.6% of them were overweight or obese which was similar to the results of our study [9]. Also, Van-Niekerk S M et al in their study on adolescent school children in Cape Town, South Africa reported that 7.7% adolescent girls were overweight based on BMI for age [10].
In the present study a total of 33(7.71% ) adolescents had a waist hip ratio of < 0.80[7] while as in a study conducted by Kumar CM et al in Andhra Pradesh 35% adolescent girls had a waist hip ratio of > 0.80 which is much higher than the present study [11].
In our study the overall prevalence of anemia was 53.3%. Out of the 114 anemic adolescents detected 21.93% were mildly anemic and 78.07% were moderately anemic. However, none of the adolescent girls was severely anemic. A similar prevalence of anemia(55.5% ) among adolescent girls was reported by Muzammil K et al in Dehradun[12] and(59.8% ) by Kaur S et al in Wardha[13]. However a higher prevalence(83.3% ) was reported by Dixit S et al in Lucknow[14] and Premlatha T et al in Tamil Nadu[15] who reported a prevalence of 78.75% with varying degrees ranging from mild, moderate and severe which were 37.5% , 35% and 6% respectively .
The present study revealed that the prevalence of anemia in the study population in the age group 12-14 years was significantly higher (63.10% ) than in 15-18 years of age group (46.90% ; p=0.021). A higher prevalence of anemia in the lower age group may be attributed to higher prevalence of menorrhagia (puberty me%norrhagia) at the time around menarche. A similar higher prevalence of anemia in 10-14 yr age group (60.71% )than 15-19 yr age group (57.44% ) was also reported by Dutt R et al in Maharashtra[16] and Rajaratnam J et al in Tamil Nadu (46.5% in 13-14 years age group and 44.05% in 15-19 years age group)[17].
In the present study the prevalence of anemia was significantly higher in upper SE class (66.70%) followed by lower class (60.40%) and middle class (39.20%, p= 0.006). A higher prevalence of anemia in the higher SE status may be attributed to the fact that adolescents from higher SE classes are more conscious of their body image and thus resort to practices like dieting which might lead to a deficiency of various macro and micronutrients including Iron leading to anemia. However, in contradiction to our study, Siddharam SM et al reported a higher prevalence of anemia in lower SE strata (29.61% in SE class IV and V) in Hassan district, Karnataka[18]. Similarly Gawarika R et al found the overall percent prevalence of anaemia among the adolescent girls of weaker economic group in Madhya Pradesh as 96.5% and among girls of middle or higher middle income group as 65.18 %[19].
Only 3.97% of our study participants in this study showed palpable thyromegaly.Rest of the study participants (96.02%) did not have any thyromegaly. A similar prevalence of thyromegaly (5.12%) in female adolescents in West Bengal was reported by Haldar A et al[20].
Conclusion
It is concluded from our study that a considerable number of adolescent girls suffered from various nutritional problems. The common nutritional problems observed in these girls were anemia, thinness, overweight and obesity.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors/ editors/ publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
Recommendations
Based on the results of our study the following recommendations are put forth:
- Since anemia was the most common nutritional problem seen in these adolescent girls, generating awareness among mothers on iron rich foods and their importance will be helpful in overcoming this problem.
- Undernutrition in the form of thinness was also seen in a considerable proportion of adolescent girls. In this regard, parents as well as teachers should be sensitized on under nutrition and the role of healthy diet [7].
- Over nutrition in the form of overweight and obesity was also seen in some of these girls. So, parents need to be educated about the importance of healthy eating habits and regular physical activity[7].
- Volunteers from among the school girls can be trained as peer educators who can in turn educate other girls regarding various aspects of nutrition.
- Operational research and behavioural studies for finding new and innovative ways with which to approach the nutrition problems during adolescence should be conducted on a large scale.
- Policymakers should be informed about the needs of young people and advocate for need based policy and program changes.
- Already existing Adolescent health programmes need to be monitored and evaluated to document evidence on effective implementation.
References:
1. Lal S, Adarsh, Pankaj. Textbook of Community Medicine. 3rd ed. New Delhi: CBS Publishers; 2013. p.155-6.
2. Anand K, Kant S, Kapoor SK. Nutritional status of adolescent school children in rural north India. Indian J paediatr.1999; 36: p.810-16.
3. WHO Nutrition in adolescents-Issues and challenges for the health sector. 2005. p.1.
4. International Institute for Population Sciences (IIPS), 2010. District Level Household and Facility Survey (DLHS-3 India). 2007-08; p.41. Accessed on 20th Feb, 2015.
5. www.who.int. 2014; Available from: http://www.who.int/ growth_ref/who2007_bmi_for_age/en/. Accessed on 10th Oct, 2014.
6. Kaur S, Walia I. Body mass index, waist circumference and waist hip ratio among nursing students. Nursing and Midwifery Research Journal. April 2007; 3(2): p.84-90.
7. Darakshan A, Shah RJ, Fazili AB, Rafiq MM, Mushtaq B,Iqbal QM, Dar SY. A study on the prevalence of thinness and obesity in school going adolescent girls of Kashmir Valley. IJCMPH. July 2016; 3(7): p.1884-93
8. Wasnik V, Rao BS, Rao D. A study of health status of early adolescent girls residing in social welfare hostels in Vizianagaram district of AP, India. IJCRIMPH. 2012; 4(1): p.72-83.
9. Omobuwa O, Alebiosu CO, Olajide FO, Adebimpe WO. Assessment of nutritional status of in school adolescents in Ibadan, Nigeria. SAFP. 2014; 56(4): p.246-50.
10. Van Niekerk SM, Grimmer K, Louw Q. The prevalence of underweight, overweight and obesity in a multiracial group of urban adolescent school children in the Cape Metropole area of Cape Town. S Afr J Clin Nutr. 2014; 27(1): p.18-24.
11. Kumar CM, Babu CS. Reproductive health problems of adolescent girls between 15 and 19 in Andhra Pradesh. Pak Peds J. 2012; 36(4): p.225-34.
12. Muzammil K, Kishore S, Semwal J. Common nutritional deficiencies of adolescents in Dehradun. Indian J. Sci. Res. 2010; 1(1): p.77-80.
13. Kaur S, Deshmukh PR, Garg BS.Epidemiological correlates of nutritional anemia in adolescent girls of rural Wardha. IJCM. October-December 2006; 31(4): p.255-8.
14. Dixit S, Kant S, Agarwal GG, Singh JV. A community based study on prevalence of anemia among adolescent girls and its association with iron intake and their correlates. Indian J Prev Soc Med. 2011; 24(4): p.393-8.
15. Premlatha T, Valarmathi S, Srijayanth P, Sundar JS, Kalpana S. Prevalence of anemia and its associated factors among adolescent school girls in Chennai, Tamil Nadu, India. EOA. 2012; 2(2): p.4. Accessed on 12th Oct, 2014.
16. Dutt R, Patil S, Joshi S, Mhatre R, Ramdev. Prevalence of anaemia among adolescent girls in rural area of Raigad district, Maharashtra. Indian J Prev Soc Med. 2009; 40(3 and 4): p.143-6.
17. Rajaratnam J, Abel R, Asokan JS, Jonathan P. Prevalence of anemia among adolescent girls of rural Tamil Nadu. Indian Paediatr. 2000; 37: p.532-6.
18. Siddharam SM, Venketesh GM, Thejeshwari HL. A study of anemia among adolescent girls in Rural Area of Hassan district, Karnataka, South India. Int J Biol Med Res. 2011; 2(4): p.922-4.
19. Gawarika R, Gawarika S, Mishra AK. Prevalence of anemia in adolescent girls belonging to different economic group. IJCM. October-December 2006; 31(4): p.287-8.
20. Haldar A, Kumar MA, Chatterjee T, Kumar SA, Basu SS. A cross sectional study on iodine deficiency disorder among school children in West Bengal. Indian J Nutr Diet. April 2004; 41(4): p.160-4.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





