IJCRR - 5(10), May, 2013
Pages: 110-116
Date of Publication: 25-May-2013
Print Article
Download XML Download PDF
HISTOPATHOLOGICAL STUDY OF ORAL CAVITY LESIONS: A STUDY ON 100 CASES.
Author: Nikunj V. Mehta, Kalpana K. Dave, R.N.Gonsai, H.M.Goswami, Purvi S. Patel, Tarang B. Kadam
Category: Healthcare
Abstract:Background: Oral cavity is one of the most common sites for tumours and tumour like lesions in males especially in India. Squamous cell carcinoma is single most common malignant lesion of this region and related to continuous use of tobacco. Aims and objectives: To study the histopathology of different benign and malignant oral lesions and to compare the observed findings to similar studies with relation to age, sex and site distribution. Materials and methods: This was a retrospective study carried out in the Department of Histopathology, B.J.Medical College, Civil Hospital, Ahmedabad from January 2012 to December 2012. A total of 100 cases of oral cavity lesions were studied. Results: Benign lesions were more common than malignant lesions. The most common site was buccal mucosa with 32 cases (32%) followed by lip with 22 cases (22%). Out of the 100 cases, 75 cases (75%) were benign and 25 cases (25%) were malignant. Out of 25 malignant cases, 22 cases (22%) were conventional squamous cell carcinoma and 1 case each of clear cell odontogenic tumour, low grade mucoepidermoid carcinoma and verrucous carcinoma. Conclusion: A higher degree of suspicion, based on clinical findings and associated risk factors, precise histopathological typing of lesions to confirm or rule out malignancy is essential in the management of oral lesions.
Keywords: Oral cavity, Benign, Malignant.
Full Text:
INTRODUCTION
The oral cavity is one of the most common sites for various tumours and tumour like lesions. Oral cavity lesions are usually asymptomatic. It has been proved that there is relationship between ill fitting dentures, tobacco chewing and cigarette smoking with pathological lesions, both benign and malignant(1,2). Benign lesions are the most common with the commonest being mucocele, inflammation, fibroepithelial polyp, hemangioma, fibroma and submucosal fibrosis(3,5). Among the malignant lesions, squamous cell carcinoma is single most common malignant lesion of this region. The most common sites are buccal mucosa, lip, tongue and palate(6,7) .
MATERIALS AND METHODS
Retrospective study was carried out in the Department of Histopathology, B.J.Medical College, Civil Hospital, Ahmedabad from January 2012 to December 2012. A total of 100 incisional biopsied specimens were processed by routine paraffin method followed by Hematoxylin and Eosin stain and reviewed by pathologists.
RESULTS
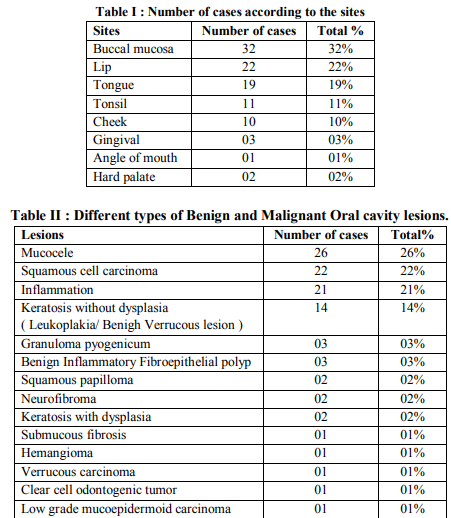
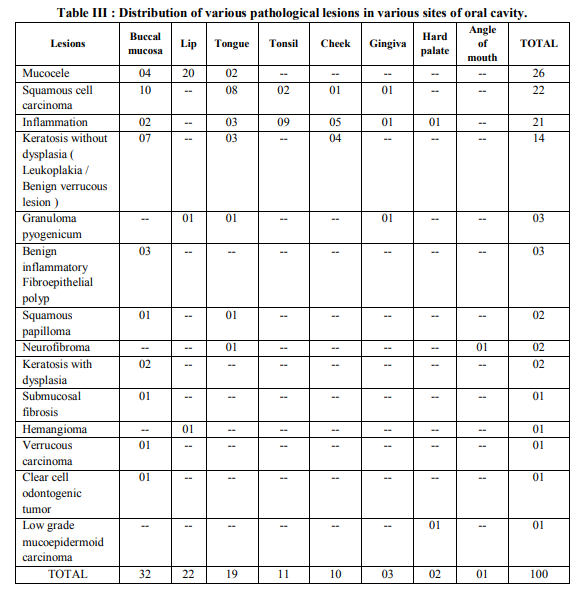
In the present study the affected age range was from 7 to 80 years with a mean age of 35 years. The youngest patient (7 year old male) presented with Granuloma pyogenicum of upper lip and the oldest patient (80 years old male) with mucous retention cyst of buccal mucosa. Lesions were more common in male (71 cases; 71%) than in females (29 cases; 29%). The more common age group was 18-40 years. Among 100 cases, 25 cases (25%) were malignant and 75 cases (75%) were benign ( Table II ). The most common site was the buccal mucosa (32%) in the present study ( Table I ). The characteristic common locations of individual oral lesion were shown in Table III.
DISCUSSION
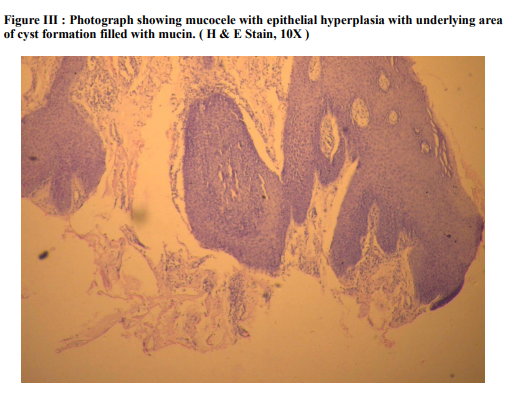
Oral cavity is one of the most common sites for neoplasm in males especially in India which is due to higher tobacco chewing or smoking. The study from January 2012 to December 2012 includes a variety of 100 oral cavity lesions, both benign and malignant which were then analyzed for the purpose of studying the clinical aspects as well as histopathological patterns of oral lesions. The observations were recorded and compared with work of other reputed study of researchers. Our study showed benign lesions were more common than malignant lesions which was also shown in the study of other researchers. The incidence of both benign and malignant lesions in our study were 75 cases (75%) and 25 cases (25%) respectively. Similar finding was seen in a study done by Shamim et. al. who evaluated 244 oral gingival lesions in India and showed nonneoplastic in 75.5% and neoplastic in 24.5%(1) . Another study done by Mujica et al. where of the lesions were benign and comprised of either inflammatory or reactive lesions(2) . In our study, the affected age range was 07 to 80 years with mean age of 35 years. In a study done in Northern Jordanian population by Khateeb et al, the age of the patient ranged from 6 to 98 years (3). In another study done by Furlong et al, the youngest patient was 9 years and the oldest was 92 years old(5). Peak incidence of oral cavity lesions were seen in age group 18 to 40 years which was comparable with study done by AlKhateeb et al where the majority of lesions were seen in 2nd to 4th decade(3) . Although oral cavity lesions are common among all the ages & can affect any site. Predominance of involvement is noted in different sites in different studies. Al-Khateeb et al. study show predominance of palatal lesion, Pudasaini et al. study show predominance of lip lesion while in our study most common site of involvement is buccal mucosa(3,4) . In our study there were 22 cases of squamous cell carcinoma ( Figure I ), the age ranging from 40- 65 years. In studies done by Ildstad et al and Weber et al, majority of the squamous cell carcinomas were seen in the 6th decade(6,7) . Mucocele ( Figure III ) was seen in 26 cases (26%) and 20 cases occurred in lip (20%), 4 cases occurred in buccal cavity and 2 cases occurred in tongue . Oliveira et al also showed that the lip was the common site for mucocele in his study(8) . Clear cell odontogenic tumor ( Figure II ) is a rare odontogenic tumor arising from the anterior region of mandible characterized histologically by sheets of cells with clear cytoplasm lying in fibrous stroma(09). It occurs in patients ranging from 14 to 89 years (mean 55.6 years), sixth decade being the most frequent(09). Female :Male ratio is 11:8(10). According to a study conducted by Siriwardena et al. the most common location was the premolar area of both the jaws(11). There was 1 case of clear cell odontogenic tumor from 1 st premolar to 3rd molar on right side of lower buccal vestibule in 62 year old male in our study. Verrucous carcinoma is a specific, welldifferentiated and nonmetastasizing variant of squamous cell carcinoma(12) . It appears as a painless, thick white plaque resembling a cauliflower. The most common sites of oral mucosal involvement include the buccal mucosa, followed by the mandibular alveolar crest, gingiva and tongue. Most patients are elderly males(12). In our study there is a case of verrucous carcinoma in 50 years old male patient. Site is buccal mucosa.
A mucoepidermoid carcinoma is a tumour that usually occurs in the salivary glands. They contain three cellular elements in varying proportions: squamous cells, mucus-secreting cells, and "intermediate" cells. It is most common in middle age group (35 - 65 years) (13) . Women are more commonly affected than men (3:2), and the mean age at onset is in the 5th decade of life. Out of major salivary glands, parotid gland is the most common site. Out of minor salivary glands ( palate, retromolar area, floor of the mouth, buccal mucosa, lip, tongue ), palate is the most common site (13). In our study, there is a case of 30 years old female patient diagnosed as low grade mucoepidermoid carcinoma of hard palate. Other benign lesions that we came across in our study were hemangioma, fibroma, submucosal fibrosis, fibroepithelial polyp and papilloma. Studies have shown that these lesions are not very common but often occur in the oral cavity(3,5) .
CONCLUSION
In our study, we concluded that majority of oral cavity lesions were benign. However, the origin and nature of the oral cavity lesions cannot be confirmed by clinical examination alone. Hence, it is must to have a histopathological examination to confirm the histogenesis and malignant potential of the oral lesions.
ACKNOWLEDGEMENT
We would like to express our gratitude to Department of Pathology, B.J. Medical College, Ahmedabad. We also acknowledge the great help received from the scholars whose articles cited and included in references of this manuscript. We are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. We are grateful to IJCRR editorial board members and IJCRR team of reviewers who have helped to bring quality to this manuscript.
References:
1. Shamim T, Varghese VI, Shameena PM,et al. A retrospective analysis of gingival biopsied lesions in south Indian population : 2001- 2006.Med Oral Pathol Oral Cir Buccal 2008; 13: E414-8.
2. Mujica V, Rivera H, Carrero M. Prevelance of oral soft tissue lesions in an elderly Venezuelan population. Med Oral Pathol Oral Cir Bucal 2008;13:E270-4.
3. Al-Khateeb TH. Benign oral masses in a Northern Jordanian population- a retrospective study. Open Dent J 2009;3:147- 53.
4. Pudasaini S, Baral R, Oral cavity lesions: A study of 21 cases, Journal of Pathology of Nepal (2011)Vol.1,49-51.
5. Furlong MA,Fanburg-Smith JC, Childers EL. Lipoma of the oral and maxillofacial region: site and subclassification of 125 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2004;98:441-50.
6. Ildstad ST, Bigelow ME, and Remensnyder JP. Squamous cell carcinoma of the alveolar ridge and palate. A 15-year survey. Ann Surg 1984;199:445-53.
7. Weber RS, Peters LJ, Wolf P, Guillamondegui O. Squamous cell carcinoma of the soft palate, uvula, and anterior faucial pillar. Otolaryngol Head Neck Surg 1988;99:16-23.
8. Oliveira DT, Consolaro A, Freitas FJ. Histopathological Spectrum of 112 cases of mucocele. Braz Dent J 1993;4:29-36.
9. Muramatsu T, Hashimoto S,Inoue T,Shimono M,Noma H, Shigenmatsu T : Clear cell odontogenic carcinoma on the mandibleHistochemical and immunohistochemical observation with a review of literature. J Oral Pathol Med 1996;25:516-521.
10. Madhu K. Nair, E. Jefferson Burkes and Onanong Chai-U-Dom: Radiographic manifestation of clear cell odontogenic tumor. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2000;89: 250-254.
11. B.S.M.S. Siriwardena, W.M. Tilakaratne, R.M.S.K. Rajapaksha : clear cell odontogenic carcinoma- A case report and review of literature. Int J Oral Maxillofac Surg;33;512- 514.
12. Rosai amd ackerman’s, surgical pathology, 3 rd edition, verrucous carcinoma :Chapter 5:246-247.
13. Som PM, Curtin HD. Head and Neck Imaging, Volume 1 und. Mosby. (2003)ISBN:0323009425.

|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





