IJCRR - 5(11), June, 2013
Pages: 118-122
Date of Publication: 18-Jun-2013
Print Article
Download XML Download PDF
MASSIVE HEMOPERITONEUM SECONDARY TO CORPUS LUTEAL CYST RUPTURE WITH NODULAR HEPATIC CIRRHOSIS- INTRAOPERATIVE DIAGNOSIS- CASE REPORT
Author: Nayak Samir R., Kasimbi G., Soren K. Dilip, Aswini V., Rao Bhaskara Ganni
Category: Healthcare
Abstract:Rupture of an ovarian cyst is a common occurrence in women of reproductive age. Bleeding from ruptured corpus luteum may vary from mild hemorrhage to massive hemoperitoenum leading to shock necessating urgent surgical intervention. We present a 21 year female admitted with gross pallor, fainting attacks, abdominal distension .she had 6 weeks history of amenorrhoea.Clinically and sonologically the patient was diagnosed as ruptured ectopic pregnancy with massive hemoperitoneum but urine pregnancy test was negative. The laparoscopy revealed gross hemoperitoneum, ruptured left ovarian cyst with grossly nodular cirrhotic liver. There was no prior history or treatment suggestive of hepatic cirrhosis. The massive hemoperitoneum from luteal cyst rupture was secondary to deranged coagulation mechanism due to nodular cirrhotic liver. The laparoscopic procedure recorded, the journals regarding the topic searched and reviewed.
Keywords: Corpus luteal cyst, hemoperitoneum, cirrhotic liver
Full Text:
INTRODUCTION
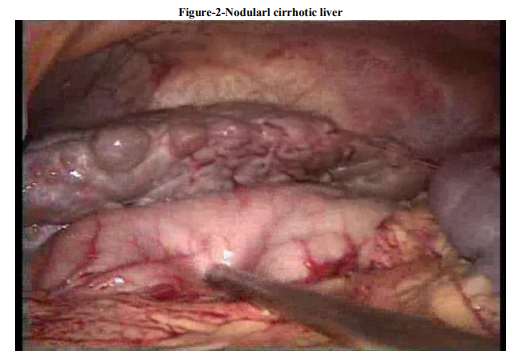
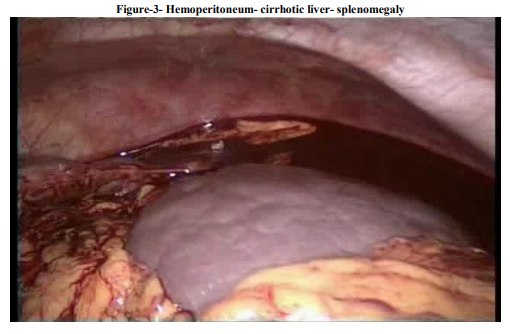
Ovarian cyst occurs during reproductive years, at end of menstrual cycle, or during pregnancy. The usual manifestations are palpable adnexal mass, abdominal pain if torsion or rupture of the cyst occurs. The presentation of ruptured luteal cyst may vary from no symptoms to symptoms and sign of acute abdomen. Ruptured corpus luteal cyst in some instances causes massive intraperitoneal hemorrhage leading to death [1] Predisposing factors for massive hemoperitoneum from ruptured ovary are abdominal trauma, bleeding diathesis, anticoagulation therapy, or patient with dialysis, recent sexual intercourse [2] A young female admitted with provisional diagnosis of ruptured ectopic pregnancy and gross hemoperitoneum. Diagnostic laparoscopy revealed gross hemoperitoneum with ruptured corpus luteal cyst.Uterus and both the tubes were found normal. To be surprise, there was grossly nodular cirrhotic liver with enlarged spleen. The massive hemoperitoneum with rupture ovarian cyst was secondary to thrombocytopenia due to nodular cirrhotic liver. The patient was not aware of hepatic cirrhosis or she was not having any symptoms related to cirrhosis. Nodular liver and splenomegaly was diagnosed intraoperatively. This type of presentation is not mentioned earlier.
PATIENT AND METHODS
21-year female presented to the emergency department with complain of severe abdominal pain of 8 hours duration .She had fainting attack two times with reeling of head. She had history of amenorrhea for 6 weeks. The pain was severe at periumblical and suprapubic region . She denied any vaginal bleeding or discharge. Her gynaeic history was irregular periods occurring 25 to 45 days interval. She was sexually active , had 2 children and tubectomised. At admission she was drowsy and clinically gross pallor. Her blood pressure was 90/60 mmHg. Pulse rate was 120 / minute, respiratory rate was 22/ minute,temperature 99degree farenhit.There was no petechial hemorrhage over skin. She was anicteric. Cardiovascular examination –heart rate was 120/ minute with normal 1st and second heart sound. Lungs were clinically clear. There was mild abdominal distension with diffuse tenderness in all quadrants. Free fluid was noticed on percussion.On vaginal speculum examination there was no blood in the vaginal vault. The cervical os was closed. Uterus size could not be ascertained due to tenderness. The left adnexae was more tender on bimanual palpation. The patient laboratory values were Hb % - 5 gm /dl, platelet count -33000/cmm. Total WBC 8,000/cmm.Urine pregnancy test was found to negative.Pelvic sonogram was performed which revealed uterus 7.2x 5.8x 4.1 cm. The endometrial echo was 1.2 cm thick and no intrauterine pregnancy. The left adenaxa measured 4.5 x 5.6 cm.Gross amount of fluid seen in abdomen. The final sonological impression was ruptured ectopic pregnancy with gross hemoperitoneum. The patient was taken to the operating room with a presumptive diagnosis of a ruptured ectopic pregnancy.Laparoscope done keeping camera port at umblicus. Hemoperitoneum of approximately 2 .5 liters with blood clots in the pelvis was seen.Fallopian tubes, the right ovary and the uterus were normal. A left ovarian cyst size 6x5 cm resembled a corpus luteum with a small rupture with ongoing bleed. Liver was grossly cirrhotic with enlarged spleen.Left ovarian cystectomy was performedachiving excellent homeostasis. The laparoscopic procedure was uneventfull.She was transfused with 2 units of packed red blood cells and 3 packets of platelets. Injection VIT K was supplemented. She was discharged on 4th postoperative day to home in stable condition after taking the opinion from the medical gastroenterologist regarding nodular liver. The histopathology report showed corpus luteum cyst with hemorrhage.
DISCUSSION
Acute lower abdominal pain, dizziness, fainting attack in a reproductive age group with history of amenorrhea, the ectopic pregnancy may be the first provisional diagnosis. A ruptured ovarian cyst can produce massive hemoperitoneum, with clinical symptomatology and son graphic features that closely mimic those of other disorders, in particular ectopic pregnancy. [1] Ovarian hemorrhage from corpus luteum of menstruation or pregnancy can be life threatening surgical condition which occurs at all stages of a woman reproductive life. A corpus luteal cyst predispose to rupture, delay in menses and pregnancy – increase risk of abortion and ectopic pregnancy[2 3] Negative pregnancy test may not exclude ruptured ectopic pregnancy [4].Pelvic sonogram plays a pivotal role in the diagnosis and management of lower abdominal pain in reproductive age group[5]. The sonogram performed by radiologist did not reveal an intrauterine gestational sac and the presence of clots in cul-de-sac fluid was noted. Moreover, it was highly suggestive of ectopic pregnancy in the left adnexa. If the patient is clinically unstable, large amount of free fluid in abdomen and pelvis differentiating between a ruptured ectopic and a ruptured hemorrhagic corpus luteum is unimportant, since in either case laparotomy/laparoscopy is indicated[3] Laparoscopy surgery for diagnosis and treatment of women with ruptured hemorrhagic corpus luteum appears superior to laparotomy [6]. We did diagnostic and then therapeutic procedure for our case. Diagnostic laparoscopy with documentation showed hemorrhagic ovarian cyst, hemoperitoneum and nodular cirrhotic liver. The intraoperative diagnosis changed from ruptured ectopic pregnancy to significant hemorrhage from hemorrhagic ovarian cyst. The massive hemoperitoneum resulted from thrombocytopenia due to nodular cirrhotic liver Review of literature reported rupture of corpus luteal cyst occurred during the secretory phase and most women reported recent sexual intercourse prior to the onset of pain. There have been case reports of luteal cyst rupture with massive hemoperitoneum during dialysis, thrombolytic therapy, patient with Hb SC disease, and patient on anticoagulation therapy.[7,8,9,10] In our patient the past history was nil significant.Luteal cyst rupture with gross hemoperitoneum and the incidental finding of nodular hepatic cirrhosis in laparoscopy not earlier mentioned. Thrombocytopaenia is common finding in patient with sever liver disease. Thrombocytopaenia of less than 30,000 associated with spontaneous bleeding is usually not sen in uncomplicated cirrhosis[11].In the reported case, blood platelet count was significantly decreased to 30,000/cmm with elevated PT and APTT. This deranged coagulation profile was the precipitating factor for massive haemoperitoneum following rupture of luteal cyst.
CONCLUSION
Rupture ectopic and ruptured luteal cyst are the important cause of hemoperitoneum in the reproductive age without history of trauma. In a setting of massive haemoperitoneum intervention is unavoidable but the exact cause/predisposing factor may go unnoticed with convetional approach where seeing a cirhhotic liver is difficult with lower abdominal inscision.Laparoscopy in an otherwise healthy woman may unmask the underlying pathology like liver disease related bleeding derangements and facilitates further management.
Sources of Conflict NIL
ACKNOWLEDGEMENT
Authors acknowledge the great help received from the scholars whose articles cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. Authors are grateful to IJCRR editorial board members and IJCRR team of reviewers who have helped to bring quality to this manuscript.
References:
1. Hallatt JG, Steele CH Jr, Snyder M. Ruptured corpusluteal cyst with Hemoperitoneum: A study of 173 surgical cases. Am J Obstet Gynecol. 1984 May 1;149(1):5-9
2. Sivanesaratnam V , Singh A, Rachagan SP, Raman S.Intraperitoneal hemorrhage from a ruptured corpus luteum. A cause of acute abdomen. In women med J Aust. 1986 APR 14:144(8):411-4
3. Aggarwala Anjal,Goel Poonam,Wanchu Madhavi,Malhotra Rimpy,Malhotra sarala.Ruptured corpus luteum with hemoperitoneum.Journal obst and gynaecology india 2004:54:488-90
4. Yi-An A,Gino Farina, halene Lhamon.Ruptured ectopic pregnancy with a negative urine pregnancy test. The journal of urgent care medicine 2007:26-28
5. Lawrence A Cicchiello, Ulrike M Hamper, Leslie M Scoutt ultrasound evaluation of gynecologic causes of pelvic pain. Obstet Gynecol Clin North Am 2011 Mar ;38 (1):85-114, Teng SW, Tseng JY, Chang CK, Li CT, Chen YJ, Wang PH Comparison of laparoscopy and laparotomy in managing hemodynamically
6. stable patients with ruptured corpus luteum with hemoperitoneum. J Am Assoc Gynecol laparoscope 2003 Nov;10(4):474-7
7. Muller CH, Zimmermann K, Bettex HJ. Near-fatal intra-abdominal bleeding from a ruptured follicle during thrombolytic therapy. Lancet Jun 15 1996;347(9016):1697. [Medline].
8. Gupta N, Dadhwal V, Deka D, Jain SK, Mittal S. Corpus luteum hemorrhage: rare complication of congenital and acquired coagulation abnormalities. J Obstet Gynaecol Res Jun 2007;33(3):376- 80.[Medline].
9. V. Andikyan, J. Ronald, C. Bowers. Massive hemoperitoneum secondary to ruptured corpus luteum cyst of pregnancy in 17-year old female with Hemoglobin SC disease. The Internet Journal of Gynecology and Obstetrics 2010;12 Number 2:351
10. Fraley DS, Johnston JR, Bruns FJ, Adler S, Segel DP. Rupture of ovarian cyst: massive hemoperitoneum in continuous ambulatory peritoneal dialysis patients: diagnosis and treatment.Am J Kidney Dis. 1988 Jul;12(1):69-71.
11. Ahmadhameed, Samina Naeem, A. Saeed Shaikah Irfan Khursheed,Ambreen Hamid,I.A Naveed. An Assessment Of Coagulation Parameters In Liver Cirrhosis medica/Biomedica

|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





