IJCRR - 5(3), February, 2013
Pages: 104-107
Date of Publication: 18-Feb-2013
Print Article
Download XML Download PDF
PYOGENIC LIVER ABSCESS - CLINICAL, RADIOLOGICAL AND BACTERIOLOGICAL CHARECTERISTIC AND MANAGEMENT STRATEGIES
Author: C.P. Ganesh Babu, R. Kalaivani
Category: Healthcare
Abstract:Pyogenic liver abscess is one of the most common clinical condition seen in private set up. 100 patients with pyogenic liver abscess were managed at department of general surgery, MAPIMS between may 2006 to October 2009. The investigations conducted were abdominal ultrasound, chest x ray, complete blood count, liver function tests and hem agglutination tests. Depending on the size of the abscess the patients were managed by parental antibiotics and percutaneous needle aspiration or surgery. Results : pyogenic liver abscess common in males and seen in right lobe. 20% were multiple. percutaneous needle aspiration with parental antibiotics is the most successful therapy.
Keywords: pyogenic liver abscess, needle aspiration.
Full Text:
INTRODUCTION
Pyogenic liver abscess is a condition with significant morbidity and mortality. The most common presenting clinical symptoms are upper abdominal pain, tenderness, hepatomegaly, high grade fever, nausea, and vomiting. These features are variable depending on the size of the abscess, general health of the patients, associated diseases and complications. In majority of cases, underlying cause could not be identified. It may be because of bacterial or parasitic invasion of liver . Majority of abscess are solitary and sub- diaphragmatic and noted in the right lobe of liver. For the last two decade , the advances in the imaging field coupled with ultrasound guided percutaneous needle aspiration and drainage brought dramatic changes in the pattern of treatment of liver abscess.. The aim of our study was to determine the clinical, radiological and bacteriological characteristic of the condition.
MATERIALS AND METHODS
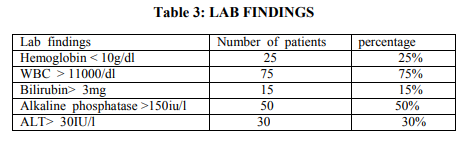
100 patients with pyogenic liver abscess were managed in the department of surgery in MAPIMS from may 2006 to October 2009. All the patients were sent to radiology department for the confirmation of diagnosis on ultrasound, chest x ray was also performed. Ultrasound guided percutaneous needle aspiration and drainage was performed in the radiology department. Other investigations include complete blood count, liver function tests, heamagglutination tests.(Table 3). Abscess smaller than 5cm were managed by parental antibiotics therapy while larger than 5cm were planned to be managed by ultrasound guided percutaneous aspiration.
RESULTS
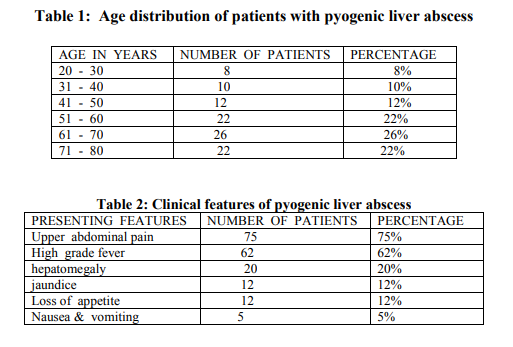
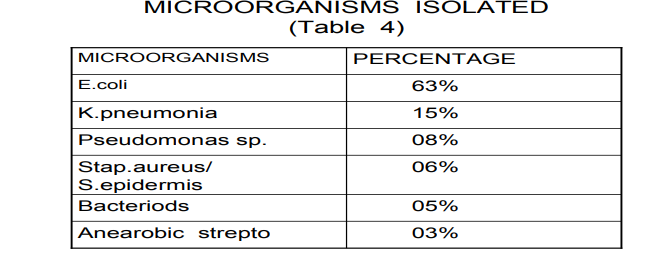
In our institution 85 out of 100 (85%) were males and 15 out of 100 (15%) were females, male: female ratio is 6:1. The patient’s age was ranging from 20 – 80 years. Mean age 50 years.5 Majority of patients (75%) with pyogenic liver abscess presented with upper abdominal pain , high grade fever was noted in 62%, hepatomegaly plus tenderness (20%) patients, jaundice in 12%, loss of appetite in 12%, nausea and vomiting was complaint in 5% of patients. (Table 2) 8 . Eighty five patients were diagnosed accurately on ultrasound with characteristic of lesion which plays central role for quick diagnosis. Intravenous antibiotic therapy ( cephalosporin combination with metronidazole and aminoglycosides) started to all patients. 52 patients improved completely by this regime. These patients were having a single abscess less than 5cms size. 28 patients having single abscess larger than 5cm were managed with antibiotic regime and percutaneous needle aspiration.4 . 20 patients having very large abscesses (10cm) were planned to be managed by antibiotic with catheter drainage. 15 patients got improved by this mode of management. Two patients planned for open surgery. 3 patients died, one due to septicemia, 2 because of organ failure. Blood cultures of 100 patients confirmed the presence of Escherichia coli in 36% while microbiological report of abscess aspirates of 63 patients confirm Escherichia coli.(Table 4). Other laboratory tests confirmed as Hb 11000 in 75 cases, bilirubin > 3mg in 15 cases, alkaline phosphatase > 150iu/L in 50 cases (Table 3).
DISCUSSION
In our study the most significant clinical feature of pyogenic liver abscess was upper abdominal pain with high grade fever, hepatomegaly and jaundice as reported by others. Patients with pyogenic liver abscess need rapid diagnosis. Advances in the imaging modalities like ultrasound and CT scan made a quick and early diagnosis possible. Abdominal ultrasound is diagnostic and always play a central role in diagnosis. Because of ultrasound the mortality of liver abscess has reduced from 30% to 10 to 20%. These improvement are due to improved imaging and effective antimicrobial therapy. In our study the diagnostic rate of ultrasound is 85%. Percutaneous aspiration in combination with systemic antibiotics should be considered as first line treatment. 28 patients with >5cm size abscess were managed by aspiration and antibiotics. Twenty patients with >10cms were managed by catheter. Failure of catheter drainage in our study is 5%... open surgery was planned. These patients were inaccessible to radiological intervention as they were multiple and large. 2 patients planned for surgery and 3 died because of sepsis. Literatures suggest that diabetic patients have increased risk. In our study 12 patients were diabetic and they were not responding well to antibiotic and stay longer. Escherichia coli was the most common pathogen isolated from aspirates/ blood of our patients. However, klebsiella, streptococcus, and enterococcus are also blamed.10). The underlying causes cannot not be made out. Literatures suggest most are cryptogenic. Only 12% of cases in our study were noted with complaint of acute/ chronic features of cholangitis .9) .
CONCLUSION
Patients with pyogenic liver abscess tend to be at high risk of morbidity especially elderly and diabetic. An early and accurate diagnosis coupled with aspiration/ drainage results in dramatic changes in prognosis. A high index of suspicion , rapid diagnosis and early administration of antibiotics with radiological interventions is an effective management strategy.
References:
1. Oschner A, Debaker M, Murray S. pyogenic abscess of liver. An analysis of forty-seven cases with of literature . Am j; Surg 1938; 40; 292-319.
2. Mehnaz A, Mohsin S. liver abscess in children not an uncommon problem JPMA 1991; 273- 275.
3. Balci NC, Semelka RC, Noone TC, et al. pyogenic hepatic abscess MRI findings on T-1 and T2 weighted and serial gadolinium – enhanced gradient echo images. J of MRI 1999; 9; 285- 90.
4. Chyus, HG Lor, Kan PS, Metroweli C. pyogenic liver abscess treatment with needle aspiration clinical radiol 1997 ; 52; 912- 6
5. Smoger SH, Mitchel CK, AcClave SA. Pyogenic liver abscess; a comparison of older and younger patients. Age and aging 1998; 27: 443- 8.
6. Stalin SC, Yelin AK , Donovan AJ, et al, pyogenic liver abscess; modern treatment. Arch Surg 1991; 126: 991- 6.
7. Karatassas A, Williams JA. Review of the royal Adelaide hospital 1980 -1987. Aust NZ Jsurg 1990; 60: 893 -7.
8. Chiru CT, Lin DY, Wu CS, et al. A clinical study of pyogenic liver abscess. J formes. Med assoc 1990; 86: 571- 576.
9. Lee KT, sheen PC, Chen JS, et al. pyogenic liver abscess - multivariate analysis of risk factors. World J Surg 1991; 15: 372 -7. 10. Gazi B, zibari, pyogenic liver abscess. Surgical infection 2000; 1; 15 - 21.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





