IJCRR - 5(12), June, 2013
Pages: 104-111
Date of Publication: 28-Jun-2013
Print Article
Download XML Download PDF
BOMB BLAST IN HYDERABAD 2013: A MEDICAL ANALYSIS
Author: K. Vishnu Prasad, Vimala Thomas, K. Padmaleela, Bheemathati Ranga Rao
Category: Healthcare
Abstract:Terrorist activities have become increasingly and Hyderabad has been often a key witness to such activities. The most recent being on the 21st February 2013, when twin bomb blast rocked the peace fabric in Hyderabad and where 96 victims were injured and 17 killed. Objectives: 1) To detail the action taken post bomb blast 2) Analyse the demographic profile of the victims, 3) Enumerate the pattern of injuries and disability sustained by the victims and 4)Recommend measures for Mass casualty Emergencies. Method: Data collected from the primary site of bomb blast and also data received at the Directorate of Medical Education. Case records of patients taken prospectively as well as retrospectively from the hospitals were used. Results: A total of 113 people were affected, and 17 of them died (12 on the spot and 5 later) giving an overall mortality rate of 15% (17 out of 113) and a 'critical mortality rate' of 4.9% (5 out of 101). A higher number of males were dead (16 out of 17) and injured too (80 out of 96). The common injury patterns were Penetrating Wounds (54.5%) followed by fractures (23.9%) and Tympanic membrane Perforation (11.5%). Around 63% of the injured were left with no disability and 2% with severe disability. Rapid action taken by the emergency health team, like in triaging, quick transportation, emergency care services and follows up care, helped in saving numerous lives and also in decreasing the disability among the injured. 7 T's for management of disaster emergencies have been suggested - Timely intervention; Triage; Transportation; Treatment Protocols; Transfusion and Treatment Supplies; Team Leadership and Spirit; Training. Conclusion: Most of the injuries were due to penetrating metallic sharps contained in the explosives. Males were more affected than females. Timely intervention and good hospital care definitely helps save a number of lives. Still standard guidelines and protocols for managing mass casualty emergencies need to be developed in India.
Keywords: Bomb Blast, Triage, Injuries, Emergency, Disability.
Full Text:
INTRODUCTION
WHO defines disaster as ‘any occurrence that causes damage, economic destruction, loss of human life and deterioration in health and health services on a scale sufficient to warrant an extraordinary response from outside the affected community or area.’ A disaster could be natural or man-made hazard. What we witnessed on the 21st of February 2013, at Hyderabad was a manmade disaster – Bomb blast by terrorists. Terrorism (as developed by Cunningham1 ) is defined as the illegitimate use or threat of violence to further political objectives. It is illegitimate in that it targets civilians. It is designed to affect the audience by creating psychological states of fear in order to influence decision-makers to change policies, practices or systems that are related to the perpetrators’ political objectives.1 Bombs are attractive to terrorists because they are relatively easy to design, assemble, and deliver, and because they are sudden and violent in nature.2 Mass casualties following disasters are characterized by such numbers, severity, and diversity of injuries that can overwhelm the ability of local medical resources to deliver comprehensive and definitive medical care to all victims.3 Large blasts often produce such massive numbers of victims that medical systems can be totally overloaded and incapacitated unless they are prepared to handle the medical consequences of such events. Terrorist bombings around the world during the past 35 years have occurred primarily in urban areas and they frequently generate multiple casualties, but one has to be prepared for this. The most important means of preparing for the large casualty loads caused by bombing disasters is to understand the patterns of injuries and logistical problems that result.4 Andhra Pradesh and in particular Hyderabad has been exposed to terrorist activities for many years. Hyderabad was on the edge after twin blasts which occurred on August 25th 2007 where at least 43 people were killed and more than 70 others were injured as two bombs rocked a crowded outdoor auditorium and a popular eatery (Gokul Chat) in Hyderabad. These blasts occurred at 8:10 pm in the night. Another incident occurred on May 18th 2007, where at least 10 people were killed and more than a dozen injured in blast at 17th century Mecca mosque in Hyderabad. The most recent one was on 21st February 2013 where there was twin bomb blast at Anand Tiffin Centre in Dilsuknagar area in Hyderabad. Till date very few attempts have been made to analyze the medical situations of the victims post bomb blast in India, hence we are attempting to do one. This paper aims to throw light on the action take, the demographic profile of the victims, patterns of injuries sustained by the casualties and the residual disability they are left with and also suggestions for preparedness to tackle such emergencies.
METHOD
On Thursday, 21st February 2013, a terrorist bomb attack was perpetrated in Hyderabad, Andhra Pradesh, which led to a mass injury situation. Twin blasts a few minutes apart shook the entire neighbourhood of Dilsukhnagar area in Hyderabad. The explosions took place between 07:00 and 07:03 PM. This paper is based on the overall information and data collected by the authors and also reported by the Director of Medical education, on the number of victims treated at the different hospitals and primary care facilities at the scene. Data on the patients received at the various hospitals (Both private and Government) treatment taken and their status was taken concurrently and in a few parts obtained retrospectively. Data was analyzed and interpretations made. Out of the 113, casualties, 17 died. Data on the remaining 96 victims forms part of the basis of this report.
RESULTS
Initial emergency treatment and triage was carried out by emergency medical services (108- EMRI) near the scenes of the blasts. Triage of the disaster victims was done at the bomb blast site and the victims were segregated based on their severity and sent to Osmania General Hospital and other nearby private hospitals. Critically injured patients were sent first, followed by patients with intermediate needs, and then by those with minor injuries.
The vast majority of survivors were evacuated by 108 ambulances and many others by private ambulances and vehicles. Most casualties arrived at the hospitals between 7:30 pm and 9:30pm. The average distance of the private hospitals from the bomb blast site was 3 kilometre +/- 0.5 kilometres and Osmania General Hospital was about 6 kilometres away. As suggested by Forensic experts, ammonium nitrate material was used along with sharp metal objects in the bombs. This resulted in multiple injuries, superficial and deep wounds which penetrated the vital internal organs of the body, fractures and head injuries among the victims. These type of injuries cause massive bleeding, shock and collapse and hence some of the victims died on the spot.
The Explosion and the casualties
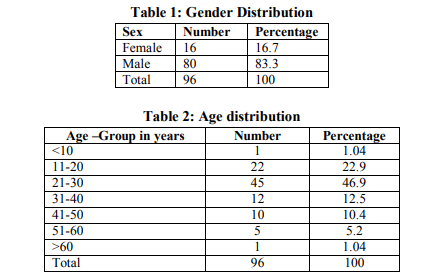
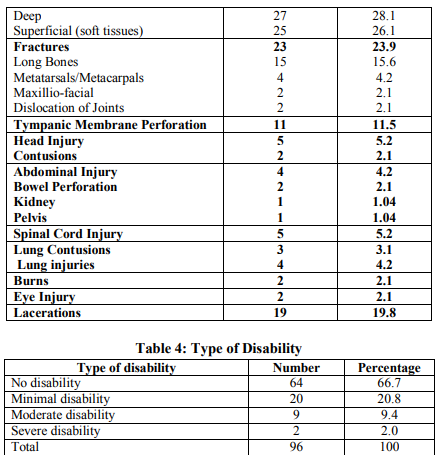
The explosions resulted in 113 casualties, 12 of who were killed immediately (deaths at the scene). There were 5 subsequent deaths (while resuscitation and in-hospital deaths), which occurred either on the same day or later on, among the 101 victims who were reported to the nearby hospitals, bringing the total death toll to 17 and the overall mortality rate to 15% (17 out of 113) and the ‘critical mortality rate’ to 4.9% (5 out of 101). The 'critical mortality rate' – the death rate among the critically injured survivors – more accurately reflects the magnitude of the disaster and the results of medical management than does the overall mortality rate, and so it should be used when comparing the outcomes from different disasters.5 The number of injured left who took treatment in the hospitals was 96. A number of procedures were performed as part of the initial resuscitation and stabilization of the injured victims upon arrival to the Emergency departments of the hospitals. Some of these procedures included medication (92.7%), fluid administration (68.8%) insertion of nasogastric tube (20.8%), and endo-tracheal intubation (7.3%). Subsequently all other medical measures were taken up. More than 20% of the victims received blood transfusions during their stay at the hospitals, some of them receiving up to 10 units of blood. Study Population Among the injured (n=96), the vast majority were males (n=80, 83.3%). Even among the 17 dead, 16 were males. (Table 1) Age wise distribution is as detailed in Table 2 with the highest percent seen in the age group 21- 30 years (46.9%) followed by 11-20 years (22.9%), the young adults. Injury Characteristics The majority of the victims sustained injury to multiple body regions with different types of injuries. Since the explosive devices contained multiple types of foreign bodies, such as shell fragments, nails, bolts, and metal balls it resulted in a combination of penetrating, blast, blunt and burn injuries. More than 54% had penetrating injuries which were either deep open wounds (28.1%) or superficial wounds (26.1%). The next most common type of injury was fractures (23.9%), the majority being long bones fracture (15.6%). This was followed by tympanic membrane perforation (11.5%). A summary of the type of injuries sustained is detailed in Table 3.
Disability
On analysis of the type of disability sustained by the injured we could conclude that majority (66.7%) have no disability, nearly 21% have minimal disability and about 2% have severe disability. The classification of disability is based on the guidelines issued by the Government of India.6
DISCUSSIONS
Terrorists worldwide have repeatedly shown their willingness and ability to use explosives to inflict significant death, destruction, and fear. Explosive devices are the most common weapons used by terrorists. A sudden and unpredictable bombingrelated Mass Casualty Emergency requires an immediate response; disrupts communication systems; interrupts transportation of casualties, medical personnel, and supplies; and may overwhelm the capacity of responding agencies. Hyderabad has been repeatedly been exposed to bomb blast and with time and experience the preparedness to tackle such mass casualty emergency has improved. Co-incidentally while comparing the number of victims (dead and injured) affected in the last bomb blasts (Gokul Chat) in Hyderabad (on 25th August 2007), to the present, the number were the same 113. The sites selected by the terrorists were crowded areas in both the bomb blast situations. The overall mortality rate for Gokul Chat bomb blasts was 38.1% (dead – 43/113) and for the present one it was 15% (17/113). Some of the factors which could have decreased the mortality rate could have been:
- Speed with which the transportation of the victims were done from the scene of the blast along with adequate triaging.
- Immediate emergency care at the hospitals including blood transfusions which played a crucial role in saving a number of lives
- Role played by the private hospitals as part of their corporate social responsibility and the immediate resuscitation and follow up care given to the victims definitely helped minimize the death toll.
In a study done by J Peral Gutierrez de Ceballos et al,3 where they studied the bomb explosions in Madrid, which resulted in 2062 casualties, the overall 'critical mortality' rate was 17% whereas in another study done by Katz et al,7 they found that after a bomb explosion in a bus the mortality rate was 10.3%. Males were predominantly affected for both injured and the dead. This was also seen in a study done by Kobi Peleg et al,8 where they analyzed the gunshot injuries and explosive injuries and they found that more than 71% affected were males. They however found that patients injured in explosions were children and the elderly which is in variation to our study where we have found that it was the young adults who were affected more. In our study the most frequent injuries found in the bomb blast victims was penetrating injuries, followed by fractures and tympanic membrane perforation. In a study done by J Peral Gutierrez de Ceballos et al3 in Madrid, the most frequent injuries found in the bomb blast victims were tympanic membrane perforations, chest injuries, shrapnel wounds and fractures. In yet another study done by Kobi Peleg et al,8 overall, apart from chest, spine, and abdominal injuries, which are more frequent in Gun Shot Wound victims, all other body regions are injured more frequently in explosion One of the most consistent injury patterns noted among survivors of terrorist bombings is the overwhelming predominance of relatively minor, noncritical injuries that are not lifethreatening.9,10 These are usually caused by secondary and tertiary blast effects, and are typically soft tissue and skeletal injuries that nevertheless tend to be extensive and contaminated, and require multiple procedures. A similar pattern has emerged in our study too. An analysis of the patterns of injury from this event has shown that most of the survivors had no critical injuries or disability as was also seen in other similar studies.5,11,12 The high immediate death rate was probably because of the extreme magnitude of the explosive force as was also reported in a study done by Frykberg et al.5 Most of the fatally injured victims died at the scene of the bomb blast. A similar pattern was seen in other studies too.5,11,12
Recommendations
The following points need to be considered for managing Mass Casualty Emergencies.
7 T’s of Management of Mass Casualty Emergency
1. Timely intervention (golden hour)
2. Triage
3. Transportation
4. Treatment Protocols
5. Transfusion and Treatment Supplies
6. Team Leadership and Spirit
7. Training of the Emergency team
1. Timely intervention
In emergency medicine, the Golden hour is the first 60 minutes after the occurrence of a major multisystem trauma. It is widely believed that the victim’s chances of survival are greatest if he or she receives definitive care within the first hour. The golden hour can be summarized by the 3R rule, “Getting the right patient to the right place at the right time.”13 In a large-scale event, each hospital should have the capability to increase staffing, rapidly assess available bed status, and open occupied beds, especially in the Emergency Department, operating rooms, and intensive care units.
2. The triage system
Triage (French: sorting) means categorization and distribution of casualties, which establishes priorities and proper location of treatment. The triage must be carried out at the disaster site as well as in the hospital. Identification: A simple method of identification, such as a tag banded to a victim, transmits information regarding patient identification. Patients can be classified according to their therapy needs viz. 1) Requiring only outpatient treatment. 2) Requiring indoor admission and expectant treatment, 3) Needing immediate exploration and 4) Capable of tolerating delayed treatment. Sections for each group can be temporarily created. Subsequently, these patients can be managed effectively by different groups of doctors.14 Another immediate priority is to setup a triage area at the entrance into the Emergency Department (ED) treatment area, which allows for unimpeded ambulance flow outside the ED and helps to avoid the immediate need to retriage casualties once inside the ED. Triage can be performed capably by experienced emergency physicians or mid-level surgeons, saving senior trauma surgeons for more effective roles in the ED or operation room.2
3. Transportation
This is of vital importance when coping with such disasters. Well equipped Ambulances with facilities for resuscitation (like endotrachel intubation) and also with ventilatory and monitoring services should be made readily available. Any delay at times result in late initiation of the management of a few patients. Coordinated transportation service is vital.
4. Treatment Protocols
As part of the response to a terrorist bombing, revision to standard of care is required. No universal methodology exists for altering standards of care. Standard Treatment protocols are needed to be developed to cater to the specific injuries post a bomb blast.
5. Transfusion and Treatment Supplies
If a terrorist bombing occurs, large amounts of blood will be required since many victims are seriously injured. The blood banking community should be well prepared to address blood needs in the event of such disasters. Shortages of essential equipment and supplies often occur in the aftermath of a terrorist bombing. Emergency stocks should always be made available. The emergency mass critical care plan should address hemodynamic resuscitation and support using intravenous fluids and vasopressors, administration of antibiotics and other diseasespecific countermeasures, prophylactic interventions to reduce adverse consequences of critical illness, and basic modes of mechanical ventilation.15
6. Team leadership and Team Spirit
Effective preparedness and response demand an established, functional leadership structure with clear organizational responsibilities. There should be a Hospital Emergency Incident Command system. In many instances, particularly at the local operational level, such preparation has not occurred. Consequently, confusion over specific roles and responsibilities during response efforts could occur. The team spirit needs to be kept motivated at all times since seeing the injured and dead in spite of their best efforts, the emergency team may experience feeling of sadness, helpless, and anxiety.
7. Training
Disaster preparedness and response education is not included in most medical or nursing school curricula. Standardized training that addresses clinical care and systems issues should be given to all levels of providers. More physicians and surgeons, require further education on the planning and emergency response process so as to be prepared to tackle any emergency mass casualty situation.
CONCLUSIONS
Most of the injuries were due to penetrating metallic sharps contained in the explosives. Males were more affected than females, with the age group of 21-30 years being most affected. Timely intervention and good hospital care definitely helps save a number of lives. Emergency Preparedness to tackle medical emergencies post a bomb blast needs a lot of planning and team work. Training the emergency team on triaging and providing good transportation facilities and ensuring an adequate supply of blood, drugs and equipment in the hospitals will go a long way in saving numerous lives and also in reducing the morbidity of the injured.
CONFLICT OF INTEREST None ACKNOWLEDGEMENTS
The authors wish to thank the emergency team (EMRI), doctors, and nurses, paramedical staff of the Government and Private hospitals, Aarogyasri Team and the local community. Authors acknowledge the help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to the authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Cunningham, W. G. (2003). Terrorism: Definitions and typologies. Terrorism: Concepts, Causes, and Conflict Resolution. Fort Belvoir, VA: Defense Threat Reduction Agency and George Mason University’s Institute for Conflict Analysis and Resolution.
2. M. Kalemoglu. The Medical Management Of Bomb-Blast Scenes In The Emergency Department. The Internet Journal of Rescue and Disaster Medicine. 2007; Volume 6 No 1.
3. Statement on Disaster and Mass Casualty Management: Committee on Trauma, American College of Surgeons
4. J Peral Gutierrez de Ceballos, F TuréganoFuentes, D Perez-Diaz, M Sanz-Sanchez, C Martin- Llorente, and JE Guerrero-Sanz 11 March 2004: The terrorist bomb explosions in Madrid, Spain – An analysis of the logistics, injuries sustained and clinical management of casualties treated at the closest hospital. Crit Care. 2005; 9(1): 104– 111.
5. Frykberg ER, Tepas JJ. Terrorist bombings: lessons learned from Belfast to Beirut. Ann Surg. 1988; 208:569–576.
6. Office of the Chief Commissioner for persons with Disabilities. Government of India. Disability guidelines.
7. Eliezer Katz, Boaz Ofek,, Jacob Adler, Harry B. Abramowitz, Michael M, Krausz. Primary Blast Injury After a Bomb Explosion in a Civilian Bus. Ann. Surg. April 1989; Vol. 209 - No. 5.
8. Kobi Peleg, Limor Aharonson-Daniel, Michael Stein, Moshe Michaelson, Yoram Kluger, Daniel Simon, Israeli Trauma Group (ITG), and Eric K. Noji. Gunshot and Explosion Injuries; Characteristics, Outcomes, and Implications for Care of Terror-Related Injuries in Israel. Ann Surg. 2004 March; 239(3): 311–318.
9. Brismar B, Bergenwald L. The terrorist bomb in Bologna, Italy, 1980: An analysis of the effects and injuries sustained. J Trauma 1982;22:216–220.
10. Biancolini CA, Del Bosco CG, Jorge MA. Argentine Jewish community institution bomb explosion. J Trauma 1999; 47:728– 732.
11. Frykberg ER. Medical management of disasters and mass casualties from terrorist bombings: How can we cope? J Trauma 2002;53:201–212.
12. Teague DC.Mass casualties in the Oklahoma City bombing. Clin Orthop 2004;422:77–81.
13. www.traumafoundation.org/restricted/tinymc e/jscripts/tiny_mce/plugins/filemanager/files/ About%20Trauma%20Care_Golden%20Hou r.pdf. Retrieved on 9-03-2013.
14. AN Supe. Disaster management- are we ready? Journal of Postgraduate Medicine 1993; 39:2-4
15. Centers for Disease Control and Prevention. In A Moment’s Notice: Surge Capacity for Terrorist Bombings. Challenges and Proposed Solutions.

|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





