IJCRR - 5(12), June, 2013
Pages: 97-103
Date of Publication: 28-Jun-2013
Print Article
Download XML Download PDF
A STUDY TO EVALUATE WORKING PROFILE OF ACCREDITED SOCIAL HEALTH ACTIVIST (ASHA) AND TO ASSESS THEIR KNOWLEDGE ABOUT INFANT HEALTH CARE
Author: Shashank K. J. , M.M. Angadi , K. A. Masali, Prashant Wajantri, Sowmya Bhat, Arun P. Jose
Category: Healthcare
Abstract:Background: One of the main aspects of National rural health mission (NRHM) is to develop a band of Accredited Social Health Activist (ASHA) workers in the rural areas with the purpose of supporting the community to access public health services. She is assigned one thousand populations and given training for 4 months. The discourse on the ASHA's role centers around three typologies: ASHA as an activist, as a link worker or facilitator, and as a community level health care provider. Objectives: 1) To assess the social and working profile of ASHA workers. 2) To assess the knowledge of ASHA workers on infant health care. Methodology: A cross sectional study was done on 132 ASHA workers selected from 5 random PHCs in Bijapur taluk. Data was collected in a prestructured proforma using interview technique from June to October, 2012. Data was represented in the form of proportions and figures. Results: Average working population of each ASHA was found to be 1078 persons, with 10 household visits/week. 45 (34.1%) ASHA opined that breast feeding should be stopped by one years of age, 34 (25.8%) to discontinue breastfeeding in case of diarrheoa. 58 (43.9%) conveyed that mothers can take Oral Contraceptive Pills during lactation. Conclusion: The effectiveness of ASHA worker largely depends on the training and support from both the health system and the community. Majority of them were not aware about their role in behaviour modification with regards to infant feeding. Reorientation training programmes should be conducted to improve their efficacy.
Keywords: NRHM, ASHA, infant, breast feeding.
Full Text:
INTRODUCTION
The National Rural Health Mission (NRHM) was launched in the year 2005 to enhance the effectiveness of public health care system especially in rural areas. The main aim of NRHM is to provide accessible, affordable, accountable, effective and reliable primary health care, and bridging the gap in rural health care through creation of a cadre of Accredited Social Health Activist (ASHA). The objective of the NRHM is to strengthen the healthcare delivery system with a focus on the needs of the poor and vulnerable sections among the rural population. The ASHA programme is considered as being vital to achieving the goal of increasing community participation with the health system, and is one of the key components of the NRHM, a flagship programme of the central government of India1 . The general norm will be ‘One ASHA per 1000 population’. ASHA must be primarily a woman resident of the village - ‘Married/Widow/Divorced’ and preferably in the age group of 25 to 45yrs having commitment for social work . ASHA should have effective communication skills, leadership qualities and be able to reach out to the community. She should be a literate woman with formal education up to Eighth Class2 . ASHA will undergo series of training to be completed in 23 days spread over a period of 12 months to acquire efficiency in counseling, identifying health related problems and necessary actions to tackle the situations 2 . This will help in reducing Infant mortality rate (IMR), Maternal mortality rate (MMR) as well as control of specific diseases, and improvement of nutrition status of children and mothers and to achieve health related millennium development goals. ASHA will take steps to create awareness and provide information to the community on determinants of health such as nutrition, basic sanitation & hygienic practices, healthy living and working conditions, information on existing health services and the need for timely utilization of health & family welfare services. The discourse on the ASHA’s role centers around three typologies - ASHA as an activist, as a link worker or facilitator, and as a community level health care provider.3 She will counsel women on birth preparedness, importance of institutional delivery, exclusive breastfeeding and weaning practices , immunization, contraception and prevention of common infections including Reproductive Tract Infection/Sexually Transmitted Infection (RTIs/STIs) and care of infants and young child . ASHA will be the first port of call for any health related demands of deprived sections of the population, especially women and children, who find it difficult to access health services.2 As the performance of ASHA is crucial in achieving the aim and objective set under NRHM, this study was done to access the social and working profile of ASHA and their knowledge regarding infant health care in Bijapur taluk of Karnataka state.
OBJECTIVES
1) To assess the social and working profile of ASHA workers. 2) To assess the knowledge of ASHA workers on infant health care.
MATERIALS AND METHODS
Out of 12 Primary health centre (PHC) in Bijapur taluk , 5 PHC’s were randomly selected for the study. After obtaining prior permission from the District health officer (DHO) , the study was conducted . The ASHA workers were contacted in their respective PHC during their monthly review meetings . After explaining the purpose of the study and obtaining oral consent, the study was conducted using interview technique. Information was collected in a prestructured proforma by the investigator. The study was conducted from June 2012 to October 2012 . Every month one PHC was visited and information was collected from the ASHA. Out of 150 ASHA workers from the 5 PHC ‘s only 132 ASHA workers could be contacted during their monthly meeting. Data was represented in the form of proportions , percentages and figures.
RESULTS
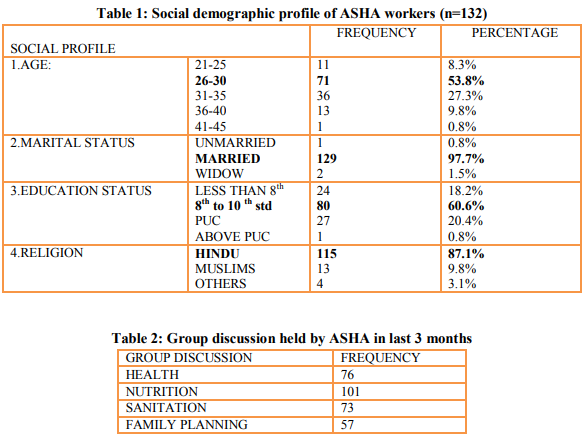
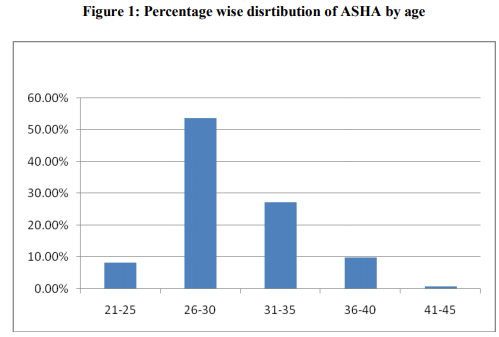
The average age of ASHA workers is 30 years, with majority 71 (53.8%) of them in the age group of 26 to 30 years.129 ( 97.7%) of them are married and 115 (87.1%) were Hindu by religion.80 (60.6%) of ASHA had formal education till 8TH standard as recommended in NRHM. [ TABLE 1] [FIGURE 1]
WORKING PROFILE OF ASHA WORKERS
The average working population of ASHA was 1078 persons/ASHA with an average of 10 household visits/week/ASHA. Each ASHA works for about 3.8 hours / day and 29.3 hrs/week/ASHA on an average.
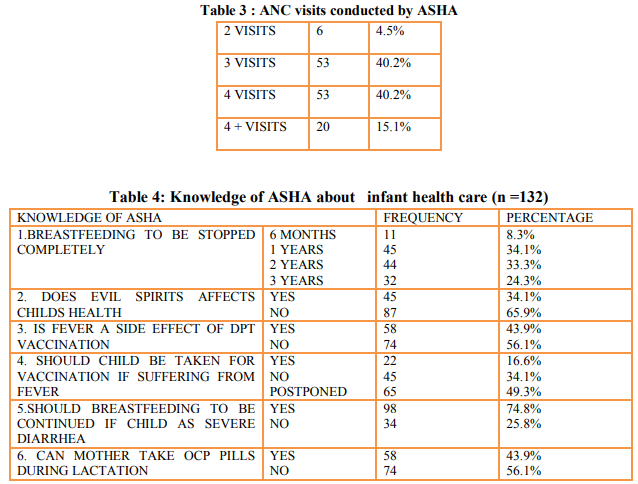
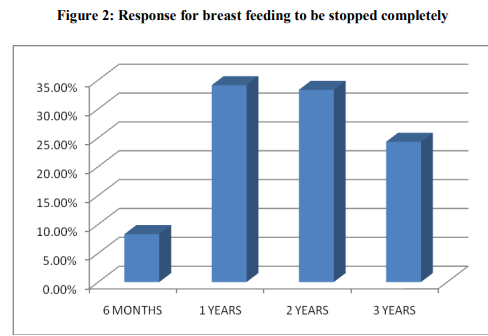
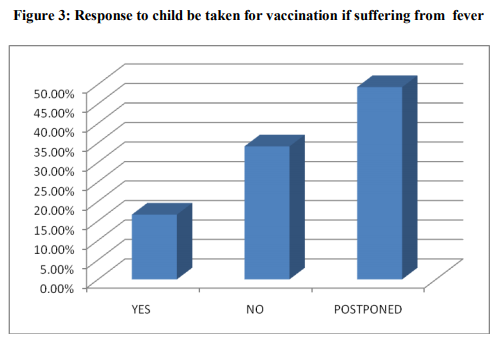
Only 26 (19.7 %) of ASHA held group discussion with the people on all aspects like health, nutrition, sanitation, family planning. Majority of ASHA 101 (76.5 %) had discussion on nutrition related topics with the community in last three months[Table 2] An average of 31 Antenatal cases was registered by ASHA last year at their respective PHC . 53 (40.2%) of ASHA said that they do 4 ANC visits and another 53 (40.2%) of ASHA did 3 ANC visits for every registered ANC cases with them.[Table 3] Knowledge of ASHA workers about infant health care All the 132 ASHA workers opined that food intake should be increased by the mother during the pregnancy period along with increased iron and vitamin supplementation. 87.1% of ASHA educate about breastfeeding to the mother before the delivery and 100% of them educate the mother and advocated breastfeeding to the new born as soon as possible after delivery. All the 132 ASHA workers gave the correct responses regarding prevention of hypothermia , care of umbilical cord, prelacteal feeds and exclusive breastfeeding practices. Regarding complete cessation of breast feeding 11(8.3%) said at 6 months, 45(34.1%) said by 1 years of age,44(33.3%) said at 2 years of age, 32(24.3%) said at 3 yrs of age. [Figure 2] 45(34.1%) of ASHA still believe that evil spirits affects the child health. Only 58(43.9%) were aware that child suffers from fever after DPT vaccination . 65(49.3%) ASHA opined to postpone the vaccination if child is suffering from high grade fever [Figure 3]. All the 132 ASHA’s agreed that ORS should be the initial treatment for diarrhea in children. 98(74.8%) advised mother to continue breastfeeding even if child is suffering from severe diarrhoea.58(43.9%) of ASHA said that lactating mother can take oral contraceptive pills during the period of lactation.[Table 4]
DISCUSSION
All the 132 ASHA workers who were interviewed were working in their respective villages, which is an important and positive finding of the study. The average age of ASHA is 30 years with majority of them being between the age group of 26-30 years. In the study done by Nirupam Bajpai et al 4 the average age of ASHA was 31 years with majority of them in the same age group as in our study. Similar findings were also seen in the study done by Prof. Deoki Nandan.5 18.2% of ASHA had received education till 8th standard , which is similar to the findings of Prof. Deoki Nandan 5 done in the city of Cuttack . 129(97.7%) of the ASHA were married , which is comparable with the other studies done on ASHA by various authors 4,5,6,8 . Each ASHA worker was supposed to work for a recommended population of 1000 persons /ASHA as per NRHM guidelines 3 . In most of the studies the working population of ASHA varied from as low as 454 persons/ASHA in Chattishargh to 1431 persons /ASHA in the State of Uttar Pradesh 4 . In our study, the average population each ASHA was serving was 1078 persons which is almost equal to the recommendation in NRHM. One of the main working modalities of ASHA workers is conducting of household visits in the community for ANC,PNC, Infant care , immunization and care of the sick. On an average each ASHA was conducting 10 household visits every week in our study which is much lesser than the number of visits by ASHA in the study done by Nirupam Bajpai 4 , where each ASHA conducted 21 house visits every week. Each ASHA on an average registered 31 ANC cases in their respective PHC in the last one year, which is higher than the results found in other studies 4,5. The brighter aspects among the ASHA’s in our study was that 80.4 % of them conducted 3- 4 ANC visits for every registered pregnancy. Nirupam Bajpai et al 4 in their study found that only 56 % of ASHA conducted 3-4 ANC visits. Most of the ASHA had proper knowledge about health education and guidance to be given for mother about breast feeding practices.106(87.1%) of ASHA educated the mother about breastfeeding and its importance before delivery and 100 % of them educate and also insisted on immediate breastfeeding after delivery. Nirupam Bajpai et al 4 in their study done on ASHA in Rajastahan found that 98 % of the ASHAs educate the mother regarding breastfeeding antenatally and 96 % educate the mother postnatally. In our study 34. 1% of ASHA’s still believe that evil spirits have an effect on a child’s health which shows the misconceptions that exists in them even after undergoing training regarding causation of disease. In our study 58(43.9%) of ASHA were aware of the importance of immunization and the adverse events follwing immunization. In the study done by Srivathsha et al 70. 1% of them had good knowledge regarding importance of immunization and its adverse effects. Darshan K. Mahyavanshi Etal 6 observed that 36.92 % of ASHA had good knowledge about immunization. 43.9 % of ASHA’s wrongly advised, OCP as a method of family planning during lactation .
CONCLUSION AND RECOMMENDATION:
In a developing country like India , where more than 70 % of the population reside in the rural areas , the strengthening of the health care facility is one of the top most priority of the government. Among the various national programmes launched by the Government of India, NRHM is one of the major programmes meant for the improvement of the healthcare system in rural areas. The creation of ASHA cadre is one of the major initiatives under the NRHM. All the ASHAs in our study were residents of the community they served in , as a result of which they formed a very effective link between the delivery of health services and the community. The ASHA preferred to do their duties that were associated with financial incentivies such as ANC ,PNC and Immunization services rather than other activities like health education, nutrition, sanitation and family planning. Most of them had good knowledge about ANC, PNC and Infant care but lacked proper knowledge on family planning methods and immunization. ASHA’s also believe that evil spirits have an effect on a child’s health. Hence during the training process we need to concentrate on educating the ASHA on family planning aspects especially for the newly wed couples and contraception during the post natal period and remove belief in effect of bad eye on health. The training programme should also focus on making the ASHA understand the importance of her role in providing immunization services for the community. The Government can also conduct frequent refresher training programmes for the ASHA to strengthen their knowledge and also inform them of recent advances and changes in approach to various public health issues . The most motivating factor for the ASHA is the financial incentives what they get from government and hope of getting absorbed into government jobs in future.
ACKNOWLEDGEMENT
Authors acknowledge the great help received from the scholars whose articles cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. Authors are grateful to IJCRR editorial board members and IJCRR team of reviewers who have helped to bring quality to this manuscript.
References:
1. Park K .Health programmes in Inda. In: Park’s textbook of Preventive and social medicine.21th ed. Jabalpur: M/s Banarsidas Bhanot; 2011.p 405.
2. Government of India, NRHM-ASHA (2005) Module Guidelines,Ministry of Health and Family Welfare, New Delhi.
3. (Internet ref: http://www.mohfw.nic.in/NRHM/RCH/guideli nes/ASHA_guidelines.pdf).
4. Mony P and Raju M . BMC Proceedings 2012: 6 (suppl 5) ; p124) Nirupam Bajpai and Ravindra H. Dholakia, Improving The Performance Of Accredited Social Health Activists In India: South Asia, Columbia University : Working Paper No. 1; May 2011.p 15-19.
5. Prof. Deoki Nandan. A Rapid Appraisal Of Functioning Of Asha Under NRHM In Cuttack, Orrisa: National Institute of Health and Family Welfare, New Delhi; 2007-2008. p 17.
6. Darshan K. Mahyavanshi Etal . A cross sectional study of the knowledge, attitude and practice of ASHA workers regarding child health (under five years of age) in Surendranagar district. Healthline ISSN 2229- 337X : Volume 2 Issue 2 ;July-December 2011.p 50-53.
7. Shrivastava SR , Shrivastava PS . Evaluation of trained Accredited Social Health Acivist (ASHA)workers regarding their knowledge .attitude and practices about child health. Rural and Remote Health 2012:2099
8. S. Haider , S. Vivek Adhish , Sanjay Gupta , Neera Dhar , Utsuk Datta , S. Menon, Deoki Nandan. A rapid appraisal of SAHIYA (ASHA) in Jharkhand. Health and Population: Perspectives and Issues; Vol. 31 (2); 2008. P 80-84.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





