IJCRR - 5(12), June, 2013
Pages: 72-76
Date of Publication: 28-Jun-2013
Print Article
Download XML Download PDF
FREQUENCY AND CLINICAL SIGNIFICANCE OF THE CONUS ARTERY AS THIRD CORONARY ARTERY ON 64-SLICE COMPUTED TOMOGRAPHY ANGIOGRAPHY (CTA)
Author: Ritu Mehta, Sanjeev agrawal
Category: Healthcare
Abstract:Background of the study: Wide information of the anatomy of coronary arteries is useful for a management decisions of the coronary artery disease or for systemic planning of surgery. The objective of this study is to establish variations of Conus coronary arteries which arise directly from aorta and revealing about their frequency .These findings would be of great significance in the interpretation of coronary arteriography, angiography and surgical myocardium revascularization. Methods: A total number of 111 angiograms were utilized for this study. The coronary angiographic images were evaluated in this study. The study is design to investigate the number by the mean of origin of right conus artery. Results: The results shows the right conus artery originates from right coronary artery in most of the people 77(69.3%). In this study right conus artery originate from same ostium in 15(13.5%) individuals and from Separate ostium (aortic) origin were seen in 18(16.2%). Conclusion: A selective Angiography is recommended for conus artery because the frequency of conus artery as the third coronary artery is 29.7% of screened cases of Cat-scan coronary angiography (CTA).
Keywords: Right conus artery (R.Con.A), right coronary artery (RCA), Ostium, pattern of origin, computed tomography Angiography (CTA)
Full Text:
INTRODUCTION
Two coronary arteries, the right and the left one are supplying blood to human heart in general population. Prevalence of Congenital coronary variations is are quite low, which is changing from 0.3% of autopsy reports to 1.3% of angiographic studies.(1,2) Sometimes extra coronary arteries are also present. The right conus artery (R.Con.A) considered as the third coronary artery, because it is originates as a separate artery from the anterior aortic sinus. (3) The right conus artery most frequently arises from the proximal part of the right coronary artery (RCA). The conus artery vascularises to the conus, or outflow tract, of the right ventricle and is usually found to be the first branch of the right coronary artery. (4) Several scientists have suggested that it provides a collateral connection between the right and left coronary arteries. The conus artery variation may be an advantage for the person having it. (5) Computed tomography Angiography (CTA) study facilitates the routine diagnostic workup for the management of Cardiac disorders. In Coronary artery diseases patients, it is also needed to carry out conventional angiography of the third coronary artery (6, 7). An intimate knowledge of the occurrence and distribution of conus coronary arteries is important for correct understanding of coronary angiograms, assessment of severity and effect of coronary insufficiency, and appropriate preparation and time being myocardium revascularisation (8).The purpose of this study is to establish variations of Conus coronary arteries which arise directly from aorta and its frequency.
MATERIAL AND METHODS
The patients, who had undergone The CT coronary angiograms for various reasons during 3 years at Geetanjali medical college and hospital, Udaipur, were included in this study. A. Exclusion criteria Patient with high calcium score >500 were excluded. B. CT scan and reconstruction parameters: All examinations were performed with a 64-slice CT scanner (Sensation 64, Siemens, Forcheim, Germany) with the scan protocol described in table no.1. C. Procedure: Pre-procedure precautions The patients were enquired, to rule out the presence of any drug allergy, to avoid the occurrence of any untoward anaphylactic reaction, during the procedure. Patient were advised to avoid tea and coffee a day prior to procedure. Blood urea and creatinine levels were checked before the procedure. The heart rate of patients were stabilised with an oral dose of 40 mg propronalol one hour before the scan ,in whom a heart rate were greater than 75 beats/min. Sublingual nitroglycerine was given to the patient just before the scan. A bolus of 100 ml of high iodinated contrast material (350 mg/ml ULTRAVIST German remedies) was injected into an antecubital vein of the right arm with a flow rate of 5 ml/s, followed by a 40-ml saline chaser. A bolus-tracking method was employed for the synchronization between arterial route of contrast material and MSCT-CA. The patient was now shifted to the CT scanner. Adequate counselling of patients were done to reduce anxiety, to preserve the best possible heart rate of 55-60 beats /min. CT angiograms of 110 patients were studied, to see the pattern of origin of right conus artery.
RESULTS
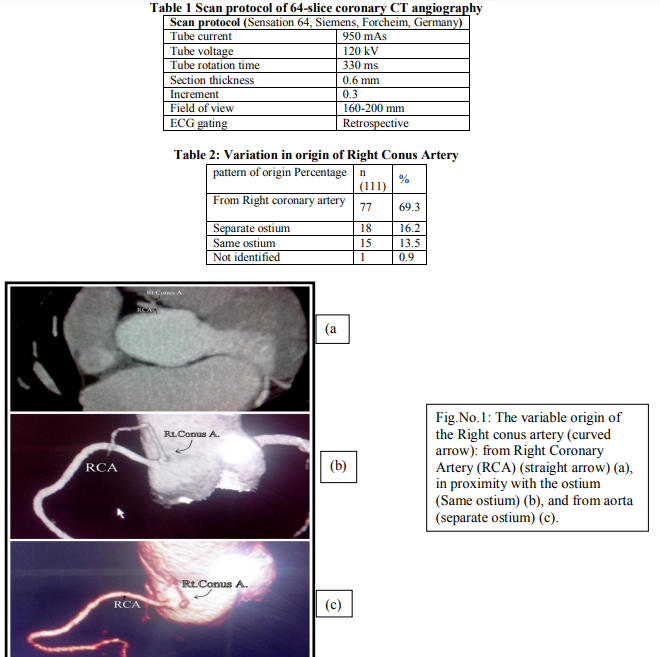
Variation in origin of Right Conus Artery Out of 111 patients, the right conus artery originates from the right coronary artery in 77(69.3%) patients , common origin from same ostium (right conus artery and right coronary artery ) was seen in 15(13.5%) patients and Separate ostium (aortic) origin of right conus artery were seen in 18(16.2% ) patients as shown in Table no.2.
DISCUSSION
The variations of number of coronary arteries are relatively common in population suggested by many scientists and could be beneficial for person or could create clinical consequences. Some authors described cases of occurrence of only a single coronary artery come up from the left (9) or the right (10) aortic sinus. This single coronary artery may be associated with cardiac complications like congestive heart failure, myocardial infarction and sudden cardiac death in young athletes (11) Hadžiselimovi? (12) points out that even three coronary arteries may arise independently from the right aortic sinus. Four coronary arteries were reported by Almira(2008) in one case, where both supernumerary arteries arose from the right aortic sinus.(13) Usually in most of the cases extra coronary artery begins from the right aortic sinus. Previous studies put forward several terms for classifying this artery: adipose artery, conal artery, arteria of Vieussens, preinfundiblar or supernumerary right coronary artery (12,14,15,16).Usually this coronary artery is a branch of Right coronary artery and called as right conus artery but it has three variations according to its origin. The most appropriate term for this artery when it originate from separate ostium, is the third coronary artery. Information about incidence of the third coronary artery are varying in different population from1.5% as stated by Lo (17) even to 62% as stated by Hadžiselimovi? (12).In our study right conus artery as third coronary artery was found in 29.7 % and this result correlated with Kalpana (2003) 24%, Pinar Kosar et al.(2009) 22% and difference with Susan standring (2006) 34% could be due to geographic variation (18,19,20). The other reason for this deference could be due to inability to selectively canulate conus /third coronary artery on conventional angiography. The common origin of right conus artery with right coronary artery was observed in 13 %.This may be useful while performing conventional coronary arteriography and angiography. Gajbe et al. suggested that a preliminary aortic root injection of dye method was followed to locate the exact number of orifice of the coronary ostia, in order to prevent the fatal outcome (21). An unusual conus artery arising independently from the RCA is mainly at risk for injury from ventriculostomy or other maneuvers carried out during heart surgery (22) According to Udaya Sankari T et al if right conus artery directly arises from the aorta (third coronary artery) than it creates double collateral circulation for intra-ventricular septum and myocardium of the left ventricle. This prevents the right coronary artery ?steal? phenomenon. ?Blessed are the people, those who are born with right conus artery with long branches? (23) In our study, the third coronary artery was found in 29.7% of screened cases what is comparable with the results showed by Yamagishi [30%] (24).In this study, 69.3% of the population had the right conus artery arising from the right coronary artery and in the rest 29.7% of the individual’s right conus artery either arose directly from the aorta or in common with right coronary artery. So the present study suggests that 29.7% of population needs care while performing coronary angiography to prevent fatal outcome. The third coronary artery could be very useful collateral in case of proximal RCA stenosis.
CONCLUSION
A non-invasive imaging of small mobile structures, such as coronary arteries has possible with the new advancement in imaging technology, such as multidetector ECG gated CT. Coronary artery diseases have high morbidity, mortality, and socioeconomic burden on society. A non-invasive detection of Right conus artery stenoses is corner stone in management of coronary artery disease with help of 64-slice computed tomography Angiography (CTA). A selective Angiography is recommended for conus artery because the frequency of conus artery as the third coronary artery is 29.7% of screened cases of CTA. The third coronary artery is appropriate term to categorize extra coronary artery which arises separately from the right aortic sinus. The third coronary artery is an extra artery or god blessing for whom that has it and be very valuable for collateral perfusion.
References:
1. Alexander RW, Griffith GC (1956) Anomalies of the coronary arteries and their clinical significance. Circulation 14:800–805.
2. Yamanaka O, Hobbs RE (1990) Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Cathet Cardiovasc Diagn 21: 28–40.
3. Gouda Hareesh, Meshri shashidhar Third coronary artery – Boon or Bane? Journal of Indian Academy of Forensic Medicine 2009, 31(1): 971-973.
4. Ivan Stankovic, Millica Jesic Morphometric analysis of the conal coronary artery. MJM 2004; 8:2-6.
5. Vilallonga J.R. Anatomical variations of the coronary arteries: The most frequent variations. Eur. J. Anat.2003;7(1):29-41
6. Feld S., Epstein M., Ayzenberg O., Caspi A. Non-visualized left anterior descending artery revealed on selective conus artery catheterization. Clin Cardiol. 1995;18(10):597-598
7. Levin D.C., Beckmann C.F., Garnic JD., Carey P., Bettmann M.A. Frequency and clinical signifi cance of failure to visualize the conus artery during coronary arteriography. Circulation.1981;63(4):833- 837
8. Tanigawa J., Petrou M., Di Mario C. Selective injection of the conus branch should always be attempted if no collateral filling visualises a chronically occluded left anterior descending coronary artery. Int. J. Cardiol. 2007; 115:126-127
9. Takano M., Seimiya K., Yokoyama S., Okamatsu K., Ishibashi F., Uemura R., Hata N., Mizuno K. Unique single coronary artery with acute myocardial infarction: observation of the culprit lesion by intravascular ultrasound and coronary angioscopy. Jpn. Heart J.2003;(44):271-276
10. Benslimane A., Funck F., Bellorini M., Lefevre T., Guillard N., Jacoly J. Single coronary artery arising from the right coronary sinus. Report of two cases. Arch. Mal. Coeur. Vaiss. 1998;91(12):1507-1508
11. Becker A.E. Congenital coronary arterial anomalies of clinical relevance.Coron. Artery Dis..1995;6(3)187—193.
12. Hadžiselimovi? H., Dilberovi? F., Ovna F.Blood vessels of the human heart: coronarography and dissection. Acta Anat. (Basel).1980;106(4):443-449 13. Almira Lujinovi*, Fehim Ov?ina, Ademir Tursi. Third coronary artery. Bosnian Journal of Basic Medical Sciences 2008; 8 (3): 226-229
14. Tanigawa J., Petrou M., Di Mario C. Selective injection of the conus branch should always be attempted if no collateral fi lling visualises a chronically occluded left anterior descending coronary artery. Int. J. Cardiol.2007;115(126):126-127.
15. David M. Fiss. Normal coronary anatomy and anatomic variations. Applied Radiology 2007;36(1)Supple: 14-26
16. Gupta S.K., Abraham A.K., Reddy N.K., Moorthy S.J. Supernumerary right coronary artery. Clin Cardiol. 1987;10(7):425-427
17. Lo E.A., Dia A., Ndiaye A., Sow M.L. Anatomy of coronary arteries.Dakar Med.1994;39(1):23-29
18. Kalpana M. A study on principal branches of coronary arteries in Humans. J Anat. Soc. India 2003; 52(2): 137-140.
19. Pnar Ko?ar, Elif Ergun, Ugur Ko?ar Anatomic variations and anomalies of the coronary arteries:64-slice CT angiographic appearance Diagn interv.radiog Dec 2009 ;15(4):275-283.
20. Susan Standring, Harold ellis, Jeremiah healy, Andrew william , David Jonn. Gray’s anatomy, 39th ed.London(uk):Elsevier;2006.p.1016.
21. Gajbe UL, Gosavi S, Meshram S ,Gajbhiye The anomalous origin of multiple coronary ostia and their clinical significance. Int.j.morp 2010 Feb; 4 (1): 2129-2133.
22. van GeunsRJ, Cademartiri F. Anatomy of the coronary arteries and vein in CT imaging. In: Schoepf UJ, ed. CT of the heart. Totowa, NJ: Humana, 2005; 219–228.
23. Udaya Sankari T , Vijaya Kumar J, Saraswathi P.The anatomy of right conus artery and its clinical significance. Recent Research in Science and Technology 2011, 3(10): 30-39
24. Yamagishi M., Haze K., Tamai J., Fukami K., Beppu S., Akiyama T., Miyatake K. Visualization of isolated conus artery as a major collateral pathway in patients with total left anterior descending artery occlusion. Cathet. Cardiovasc. Diagn.1988;15(2):95-98
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





