IJCRR - 5(12), June, 2013
Pages: 39-44
Date of Publication: 28-Jun-2013
Print Article
Download XML Download PDF
CLINICALLY SIGNIFICANT ANATOMICAL VARIATIONS OF THE LEFT CORONARY ARTERY IN HUMAN CADAVERIC HEARTS
Author: P. Dharmendra, Takkallapalli Anitha, Seema Madan, PradeepLondhe
Category: Healthcare
Abstract:The anatomy of the coronary vessels has been described in detail for atleast 3 centuries. Detailed appreciation of the normal origin, course, branching and myocardial distribution of these vessels is vital so that variations of the normal anatomy can be more easily recognized and applied to clinical practice. Knowledge of normal anatomy and variations in the branching pattern of coronary arteries is very important to identify the cause of coronary artery diseases and to perform therapeutic, radio diagnostic and surgical procedures. Since the left main coronary artery system is the commonly affected vessel and is the first vessel to show blockages, this study was conducted. 93 formalin fixed hearts were collected in the department of anatomy over a period of 2010 to 2012 and dissected. Origin, length, number of terminal divisions and the area of distribution of left main coronary artery was noted. The present study showed that the left coronary artery originated from left posterior aortic sinus except in one heart where it originated from right coronary sinus. The mean length of left coronary artery is 9.2 \?0.31mm, mean outer diameter was 4.64 \? 1.03.In 58.6% cases it bifurcated, in 35.48% cases it trifurcated and in 6.45% hearts it tetrafurcated.
Keywords: Left main coronary artery, variations, tetrafurcation, angiographic anatomy.
Full Text:
INTRODUCTION
The incidence of coronary artery diseases has seen an increasing trend in developing countries in the last few decades. The study of variations of coronary arteries especially the left main coronary artery can be of immense help to clinician planning interventional procedures such as stenting, balloon dilatation or graft surgery, particularly when there are secondary changes of calcification, plaque formation and stenosis [1]. In the vast majority of people, there are two main coronary arteries, right and left, which arise from separate ostia in the ascending aorta [2].Most of the area of heart is supplied by the left main coronary artery. The area irrigated by each of coronary arteries using postmortem angiography shows that the left main coronary artery irrigates 68.8% of the cardiac muscle mass, 41.5% by left anterior descending artery and 27.3% by the left circumflex artery[3]. These values may vary depending upon the coronary arterial dominant pattern. The left coronary artery arises from the left sinus of valsalva and courses laterally between the base of pulmonary trunk and left atrium. The left coronary artery usually divides into two major branches, the left anterior descending and left circumflex arteries. A third branch originates between the angle formed by the left anterior descending and the left circumflex arteries and has various names, including “ramus intermediate”, “median artery” , “left diagonal artery” and “straight left ventricular artery [2].
MATERIALS AND METHODS
93 formalin fixed heart specimens were collected from the department of Anatomy, Chalmeda AnandRao Institute of Medical Sciences, Bommakal Karimnagar-Andhra Pradesh, India over a period of 3 years and preserved in 10% formalin. Skin incisions were given and thorax was opened as per instructions of cunningham’s manual of practical anatomy 15th edition [4].The great vessels were ligated and the heart specimens were removed along with them. The coronary arteries were traced from their origin. Length and outer diameter of left main coronary artery were noted using a verniercaliper. Photographs were taken, all the information was meticulously tabulated, statistically analysed and compared with earlier studies. The following criteria have been taken into consideration. i).Origin of left main coronary artery. ii).Length and outer diameter of left main coronary artery. iii).Termination of left main coronary artery.

DISCUSSION
Variations related to the origin and course of coronary arteries may be benign or malignant [5]. The latter predisposes a person to early vascular compromise, ischaemia and fatal infarction. Benign anomalies of origin of left coronary artery include. i). A single coronary artery arises from the right cusp and divides into right coronary artery and left coronary artery, with the left coronary artery coursing anterior to the right ventricular outflow tract [7].
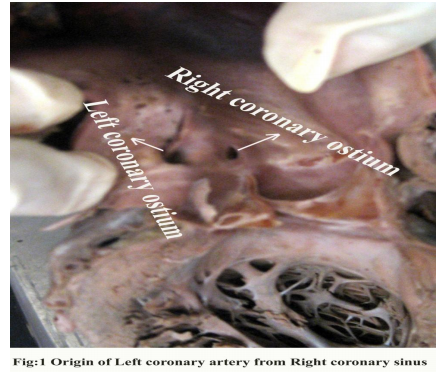
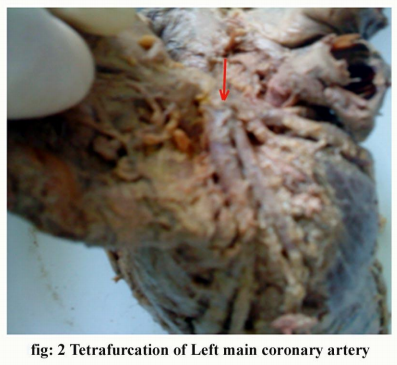
ii). A single coronary artery arises from the left cusp and divides into the right and left main coronaries, with the right coronary artery coursing posterior to the aorta. Malignant anomalies of origin of left coronary artery include. i). Malignant left coronary artery: This occurs when the left coronary artery arises from the right cusp and courses between the aorta and pulmonary artery. In this interarterial segment of the artery is subjected to compression during heavy exercise and can cause sudden death in young persons or athletes. Basso [6] considered that the left coronary artery originating from the right cusp and crossing between the right coronary artery and aorta was more dangerous than right coronary artery taking similar path, as a larger volume of myocardium is put at risk in the former case.[fig: 1] The variations in the origin of coronary arteries may be explained on embryological basis. The first evidence of coronary vessel development is the appearance at the beginning of the fifth week of intrauterine life of a structure like blood islands just under the epicardium in the sulci of developing heart [8,10]. According to the theory of Ogden J; there is a dual origin of coronary arteries, proximal and distal. The distal portion develops first. It is comprised of a retiform vascular network, similar to the capillary network that forms in the other parts of body. This network develops in the interventricular and atrioventricular grooves and forms a complete ring around the developing vessels (peritruncal ring) and communicates with the heart chamber and extra cardiac great vessels. Further development of some vessels and regression of others, the final coronary pattern develops. This theory adequately explains the variations of coronary vasculature [9,10]. In our present study the left coronary artery arose normally from left posterior aortic sinus and in 1.07% of hearts it arose from right coronary sinus. ostium was present below the supra ventricular ridge.[fig:1] [Table no: 1] The length of the left main coronary artery in general varies from 2 to 12 mm but may be upto 30mm. It’s diameter, ranging from 5 to 10 mm is generally inversely related to its length [2].Green G.E. et al [11] studied the length of the left main coronary artery in 50 consecutive autopsy specimens in which 48% of cases, the length of left main coronary artery was 10 mm or less and in remaining 52% cases, the length was up to 25 mm. the short left main coronary artery explains some failures of adequate coronary perfusion. During aortic valve surgery, myocardial perfusion depends on the placement of one or more cannulas in the coronary arteries. In this regard, the length of left main coronary artery prior to its bifurcation is particularly important. A short main trunk makes carrying out coronary angiography difficult because the catheter is inserted into one of the terminal branches, the opacification of the other branch does not occur and an incomplete image of the coronary tree is seen. In the present study, the mean length of left main coronary artery was found to be 9.2 ± 0.31mm which correlates with the above observations. [Table no: 2] Outer diameter of left main coronary artery is important in estimating the extent and severity of dilatation in cases of coronary aneurysm, calcification and stenosis. According to Glagov theory, the outer diameter of coronary artery dilates in the early phases of atherosclerosis, when plaque deposition leads to positive remodeling with preservation of the vessel lumen[16] Reg J et al [12] studied all the characteristics of the main trunk of left coronary artery in 100 autopsy heart specimens. The diameter of the main trunk measured at its midpoint was found to be in between 3 to 7mm with average value of 4.86 ± 0.8 mm. In the present study, the mean outer diameter measured at its mid point was found to be 4.64 ± 1.03 mm which is close to the above observation. [Table no: 2] The termination of left main coronary artery varies from 2 or more branches and accordingly named as bifurcation, trifurcation, tetrafurcation and pentafurcation. Banchi. A [13] described the termination of left main coronary artery varying between two to three branches with the most common pattern of the bifurcation being 64%. Which is close to the observation made in our study i.e. 58.06% hearts. In 35.48% of our present study, the left main coronary artery trifurcated, where as similar observation was also made by cavalcanti JS in 38.18% of heart specimens [14]. Bapista[15] observed that the left main coronary artery tetrafurcated in 6.7% of cases and the similar observation was found in our study i.e. in 6.45% cases. [fig: 2][Table no: 3] The left main trifurcating lesions are generally treated with bypass surgery and left main trifurcation disease is more complex than left main bifurcation disease. Therefore its percutaneous treatment is expected to have a higher rate of adverse events like stent thrombosis. Trifurcation stenting carries a high rate of adverse events and may need to be reserved for patients who are at a high risk of bypass surgery or who refuse surgery [17]. CLINICAL SIGNIFICANCE Anomalous origin of the coronary artery from the opposite sinus of valsalva is particularly important as it has been associated with myocardial ischaemia, ventricular arrhythmias & sudden death, especially when the anomalous artery course is interarterial, intra myocardial or intramural. Surgical repair in the form of uproofing of the vessel seems to be the most promising method for this condition. Isolated coronary hypoplasia, stenosis or atresia are extremely uncommon and the left coronary system is usually hypoplastic and ischaemia is frequent in these conditions. Congenital coronary artery aneurysms are indistinguishable from those acquired conditions secondary to other diseases. Major aneurysms can rupture thrombose or produce infarction due to thromboembolism.
CONCLUSION
Knowledge of coronary circulation is not only important for anatomists but also for radiologists and cardiologists performing angiographies and shunt surgeries, in diagnosis and treatment of congenital, inflammatory, metabolic and degenerative diseases involving the coronary arteries. The advances made in coronary artery bypass surgeries and modern methods of myocardial revascularization led to the present study.
References:
1. Anand M Rahalkar, Mukund.D.RahalkarPictoral essay : Coronary artery variants and anomalies 2009 February;19(1);49-53.
2. David.M.Fiss, Normal coronary anatomy and anatomic variations, Supplement to Applied Radiology January 2007, 14-26.
3. Kalbfleisch H. Hort W. Quantitative study on the size of coronary artery supplying areas postmortem AM Heart.1977; 94:183- 188.
4. G.J. Romanes, Cunningham’s manual of practical anatomy. 15th Ed; Vol: 2; Thorax and abdomen; Pg: 14-15.
5. Yamanaka O, Hobbs RE. Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Cathet cardiovasc Diagn. 1990 ; 21: 28-40.
6. Basso C , Thiene G. Congenital coronary artery anomalies at risk of myocardial ischaemia and sudden death: A report Business briefing : European Cardiology. 2005
7. Desmet W , Vanhaecke J, vrolix M , vande werf F, Piessens J, Williams J. Isolated single coronary
8. artery: A review of 50,000 consecutive coronary angiographies Eur.Heart J.1992: 13:1637-40[pub Med].
9. Decker, G.A.G, duplessis, DJ; Lec Mcgregor’s synopsis of surgical anatomy, 12th edition, ch-22 “The heart and the great vessels”,pg-280; K.M.varghese company, Dadar, Bombay 4000014, India, 1986.
10. Ogden J: The origin of the coronary arteries; circulation 1968[38]: Suppl 6:150.
11. Dr.Jyoti kulkarni, Dr.Lopa Mehta,study of angiographic anatomy of right coronary artery IOSR JDMS (sept-oct 2012) Vol 2[1]:pg.39-41.
12. Green GE, Bernsteins,Repper E.H. The length of the left main coronary artery.Surgery Dec 1967;62:1021-1024.
13. Reg J. petit.M. Main trunk of left coronary artery: Anatomic study of the parameters of clinical interst.clinical Anatomy 2004,17;6-13
14. Bnchi A.Mofolgia della arteriae coronariae cordis Arch ital anat.E Embriol 1904;3:87 Cavalcanti JS. Anatomic variation of the coronary arteries, Arq Bras Cardiology 1995,65(6):489:492
15. Bapista CA.Cel Types of division of left coronary artery and the ramus diagonalis of the human heart.Jpn Heart J.1991, 32 (3):323-335.
16. Paolo Angelini MD, Jorge Monge, Newer concepts regarding adults with coronary artery aneurysm. American heart association 2012: 125: 3076-3078.
17. Nicolas W. shammas, MD. Eric J. Dippel MD, Amber Avila Bsc, Lauren gehbauer, Leslie farland, Stefanie Brosius, Michael Jerin, Mathew winter, Penny stoakes, RN. Jeanette Byrd, RN, Lynne majestic, RN, Gail Shammas, RN, Peter Sharis, MD. Jon Robken MD. “ long term outcomes in treating left main trifurcation coronary artery disease with the Paclitayel-Eluting stent. J. invasive cardiol 2007; 19: 77-82.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





