IJCRR - 9(12), June, 2017
Pages: 27-31
Date of Publication: 24-Jun-2017
Print Article
Download XML Download PDF
Effect on Memory and Cognitive Function in Patients Suffering from Stroke - A Review
Author: Preeti Sangwan, Jaspreet Kaur, Annu Malik
Category: Healthcare
Abstract:We examined the evidence for widely held clinical beliefs about effect on memory and cognitive function after stroke, conducting narrative review. We sought to determine whether stroke patients experience problem with memory and cognitive function and which aspects of memory and cognitive functions are affected. The authentication for both memory and cognitive function dysfunction with relevance to stroke are mixed in this review. Various studies which are involved in this review are taken from google scholar, pubmed and springer link. The data is collected mainly through various research articles and reviews. Data collected from various epidemiological studies shows that global burden of stroke is high and India like other developing countries is in the centre of stroke outbreak. Correlation of memory and cognitive impairment is also included in this review. The data collected through various studies involving assessment scales provide significant evident of memory and cognitive impairment after stroke.
Keywords: Cognitive impairment, Epidemiology, Correlation, Consequences
Full Text:
Introduction:
“A stroke is a clinically defined syndrome of expeditiously developing symptoms and signs of focal loss of cerebral function with no obvious cause other than that of vascular origin, but the loss of function can at times be global. Symptoms last more than 24 hours or lead to death1. In daily life, besides physical handicaps the cognitive disorders can also come up with disability2. The risk factor for impaired cognitive functioning is cerebrovascular disease. If specifically hindered cognitive functions are considered, 50-70% of stroke patients are found to be affected depending on age3,4,5. Those patients who abide cognitively unmutilated after their index stroke, hospital-based and population-based studies have disclosed a remarkable risk for developing delayed dementia6,7. As a direct result of a stroke incident, twenty five percent of stroke left overs have dementia8,9,10.
Epidemiology:
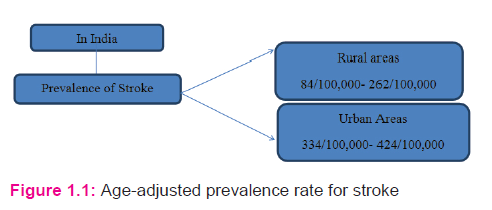
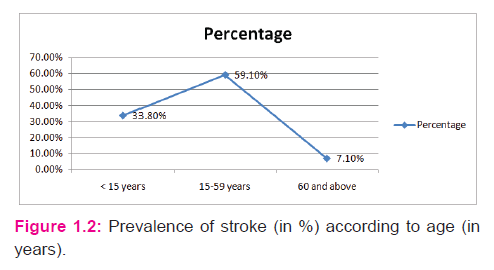
The global load of stroke is high, incorporating of increasing incidence, disability, mortality, Adjusted Life- Years, and economic impact, particularly in low- and middle-income countries. According to World Heart Federation, 15 million people worldwide agonize a stroke every year11. Globally, it is estimated that stroke is the second prime cause of death above the age of 60 years, and the fifth prime cause of death in people aged 15 to 59 years old and it is considered less common below 40 years. According to the American Heart Association, collated to white people, black people have nearly twice the risk of a first –ever stroke and a much higher death rate from stroke. According to Taylor FC et al (2012), the estimated age-adjusted prevalence rate for stroke12, is as shown in figure 1.1.
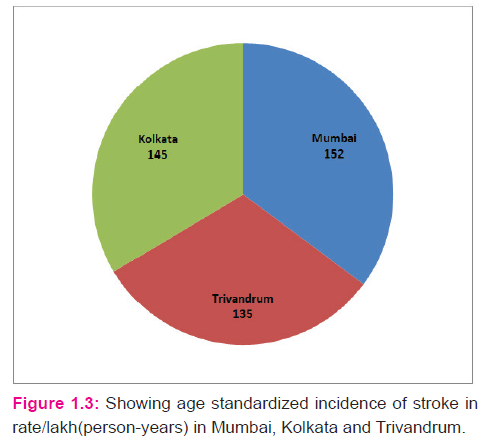
The summarized data of Stroke Epidemiology, according to the ‘World Health Organisation-STEPS Stroke protocol’ during the first decade of the 21st century in Mumbai13, Trivandrum14 and Kolkata15, has shown in figure 1.3.
Stroke is also more likely to influence people if they are obese, aged 55 or older, lack of exercise, drink excessively, have a personal or family history of stroke, stress and depression smoke or use illicit drugs, heart ailments such as recent Myocardial Infarction, atrial fibrillation and presence of blood fat molecules called apolipoproteins.
There are three chief kinds of stroke,16: 1) Ischemic stroke 2) Hemorrhagic stroke 3) Transient ischemic attacks also referred to as mini-strokes.
Etiology:
Narrowing or blocking of arteries can lead to Ischemic Stroke in the brain. It is the most common type of stroke, resulting in around 85% of strokes. Blood clots can lead to these blockages. Bursting or leaking of blood vessels in and around the brain can lead to Hemorrhagic stroke. Hypertension, trauma, blood-thinning medications and aneurysms are the conditions which can lead to rupturing of blood vessels. The most frequent form of hemorrhagic stroke is Intracerebral Hemorrhage and the second type of hemorrhagic stroke is Subarachnoid Hemorrhage. In Transient Ischemic Attack the flow of blood to the brain is only shortly interrupted.. They serve as deterrant signs for future stroke17.A study performed to assess ‘Evolution of cognitive dysfunction after stroke and risk factors for delayed progression’ concluded that cognition is rather stable for 2 years after stroke. Age, poly-pharmacy, previous cognitive decline and hypotension during admission are risk factors for its development18.
The symptoms of memory loss and vascular dementia involve slow movement and thinking, lack of attention and inability to do simple tasks. The symptoms of dementia after stroke can be masked by more evident post stroke conditions such as paralysis, depression, blindness. Other consequences of stroke are: Confusion, Headache, Numbness, trouble with seeing, trouble with walking, bladder or bowel control problems, depression, weakness or paralysis on one or both the sides of body, trouble controlling or expressing emotions. In order to remember the signs of stroke acronym F.A.S.T. is a way, which shows Face drooping; Arm weakness; Speech difficulty, if these symptoms seen then it is the time to call for emergency services19, 20.
Assessment Scales:
Various scales which can be used for assessment of memory and cognitive functioning in stroke patients are: Wechsler Memory scale- Revised21,22, Wechsler Adult Intelligence Scale –Revised 23 ,Mini Mental State Examination24,28, Scafold Objective Recognition Test 25,28 , Recognition Memory Test26,28 , FuldObject Memory Evaluation27.
Memory:
“Memory is the faculty of mind by which information is encoded, stored or retrieved”. Memory is essential to experience and related to limbic systems, it is the withholding of information over time for the determination of influencing future action. Usually, memory comprises sensory processor, short- term (or working) memory, and long term memory .Explicit and Implicit functions of memory are also understood as declarative and non-declarative systems. By information type, there are Topographic memory and Flashbulb memories. By temporal direction, retrospective and prospective memory29.
Correlation with memory and cognitive function:
Hypo-perfusion and functional deactivation in neighboring and distant areas of brain are associated with cognitive dysfunction in the acute stage of stroke. Both pathological ups and downs of glucose concentrations may influence cognition30.A study performed by Glenn T. Stebbins et al, titled, ‘Gray Matter Atrophy in patients with Ischemic Stroke with cognitive impairment’ concluded that there is a central role for the thalamus and lesser role for other cortical regions in the development of cognitive impairment after ischemic stroke.31
General cerebral atrophy has also been related to the development of cognitive impairment after stroke31. Severe white matter hyper-intensities are related to global cognitive dysfunction. A study performed by Emma J. Burton et al, titled ‘White matter hyper-intensities are associated with impairment of memory, attention, and global cognitive performance in older stroke patients’ concluded that in older stroke patients, cognitive processing speed and performance on measures of attention are remarkably related to White Matter Hyper-intensity volume, particularly in frontal lobe regions, whereas memory dysfunction is related to the volume of temporal lobe White Matter Hyperintensity32.
Memory impairment has been reported to be one of the most common cognitive deficits experienced by leftovers of stroke 33.Awareness of the lateral asymmetry, termed “hemispheric specialization”, is critically important for understanding the nature of memory impairment following unilateral brain damage33. Memory deficit may be an important predictor for cognitive decline34.
Discussion:
Cognitive impairment occurs frequently after stroke, commonly involving memory, orientation, attention and language. Some studies which shows memory and cognition decline in stroke patients included which are: A study performed to evaluate the ‘Incidence and relationship of post-stroke dementia to the influence of pre-stroke cognitive decline’ concluded that the risk of Post-stroke dementia is high, and enhanced in patients with pre-stroke cognitive shrinkage, with about one-third of patients summiting the basis for Alzheimer Disease and two-thirds meeting the basis for Vascular Dementia. These inferences confirm that, in stroke patients, an underlying degenerative pathology may play a role in the evolution of Post-stroke dementia35. Another study performed in order to investigate ‘Cognitive impairment after stroke’ concluded that stroke-associated cognitive impairment is encircled by many issues with respect to prevalence, relevance heterogeneity and uniqueness. There is no consistent phenotype because strokes can rap any part of the brain. Moreover, it is difficult to establish a causal link between stroke and dementia, or to exclude the possibility that Alzheimer disease is responsible for the cognitive impairment36.
Another study is performed to detect the ‘ Cognitive functioning after stroke’ concluded that few patients become demented after stroke, and most cognitive disturbances are in the field of mental speed and calculation37. Late emergence of Cognitive dysfunction following stroke also occurs in neonatal stroke in order to detect this a study performed by Robyn Westmacott et al, ‘Late emergence of cognitive deficits after Unilateral Neonatal Stroke’ concluded that the children with unilateral neonatal stroke, particularly males, are at increased risk for emerging deficits in higher-level cognitive skills during the school years38.
A combination of diffusion-weighted imaging, T1 and T2-weighted images has been used to determine tissue aberrations in Stroke patients39.Therapies or medicines almost never fully restore memory after stroke. However, many people do recover at the very least some memory instinctively after stroke20.A study performed by Fregni et al, reported that left prefrontal anodal stimulation for 10 minutes at 1 mA in healthy participants increased working memory performance40.A study performed ‘To investigate whether anodal trans-cranial direct current stimulation over the left dorsolateral prefrontal cortex affected the working memory performance of patients after a stroke’ concluded that the anodal trans-cranial direct current stimulation over the left dorsolateral prefrontal cortex was related to increased working memory interpretation as indexed by the recognition accuracy in patients after a stroke41.Now- a- days, mnemonics either plays a little role in treatment program or is not used at all. Memory impaired patients benefit more from images generated by the experimenter than by those self-produced. These findings decrease the practical value of mnemonics because rehabilitation is focused at administering interventions to be used independently from therapy setting42.
A study performed to examine the ‘Prognosis of acute cognitive disorders post-stroke, and to evaluate which clinical factors estimate domain-specific cognitive recovery’ concluded that recovery in visual perception/construction (83%) and visual memory (78%) was the most common. Cognitive recovery is related to age, lesion volume, lesion location, preexistent ability and diabetes mellitus30.
Conclusion:
Like other evolving countries, India is in the centre of a stroke outbreak. There is an enormous burden of stroke with remarkable geographical variations. Through various studies involving various assessment scales also it is concluded that stroke can lead to various memory and cognitive dysfunctions. Stroke allied cognitive dysfunction is encircled by many difficulties with respect to relevance, prevalence, heterogeneity and uniqueness.
Acknowledgement:
I hereby acknowledge my co-authors for constantly encouraging and supporting and helping me find my literature for this review article. Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors/ editors/ publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
Source of funding: Nil
Conflict of interest: Nil
References:
- Warlow CP. Epidemiology of stroke.1998;352: 1-4.
- Hochstenbach J, Mulder T, Limbeek J. The neuropsychology of stroke: changes in cognition, emotion and behavior. TSG 1997;75:479-485.
- Hachinski V, Munoz D. Vascular factors in cognitive impairment: where are we now?Ann N Y AcadSci 2000;903:1-5.
- Tatemichi TK, Desmond DW, Moroney JT, Stern Y. Cognitive impairment after stroke: frequency, patterns and relationship to functional abilities. J Neurol Neurosurg Psychiatry 1994;57:202-207.
- Desmond DW, Moroney JT, Paik MC. Frequency and clinical determinants of dementia after ischemic stroke. Neurology 2000;54:1124-1131.
- Tatemichi TK, Paik M, Begiella E. Risk of dementia after stroke in a hospitalized cohort: Results of a longitudinal study. Neurology 1994;44:1885-1891.
- Kokemen E, Whisnant JP, O’Fallon WM, Chu CP. Dementia after Ischemic stroke: Apopulation based study in Rochester, Minnesota. Neurology 1994; 46:154-159.
- Sacco RL, Shi T, Zamanillo MC, Kargman DE. Predictors of mortality and recurrence after hospitalized cerebral infarction in an urban community: the Northern Manhattan Stroke Study. Neurology 1994;44:626-634.
- Tatemichi TK, Foulkes MA, Mohr JP, Hewitt JR, Hier DB, Price TR et al. Dementia in stroke survivors in the stroke data bank cohort. Prevalence, incidence, risk factors and computed tomographic findings. Stroke 1990;21:858-866.
- Censori B, Manara O, Agostinis C, Camerlingo M, Casto L, Galavotti B et al. Dementia after first stroke. Stroke 1996;27:1205-12
- Mukherjee D, Patil CG. Epidemiology and global burden of stroke. 2011;76(6):85-90.
- Pandian JD, Sudhan P. Stroke Epidemiology and Stroke care services in India. Journal of Stroke 2013;15(3):128-134.
- Dalal PM, Malik S, Bhattacharjee M, Trivedi ND, Vairale J, Bhat P et al. Population based stroke survey in Mumbai, India: Incidence and 28-day case fatality. Neuroepidemiology 2008;31:254-261.
- Sridharan SE, Unnikrishnan JP, Sukumaran S, Sylaja PN, Nayak SD, Sarma PS et al. Incidence, types, risk factors, and outcome of stroke in a developing country: The Trivandrum Stroke Registry.Stroke 2009;40:1212-1218.
- Das SK, Banerjee TK, Biswas A, Roy T, Raut DK, Mukherjee CS et al. A prospective community-basedstudy of stroke in Kolkata, India. Stroke 2007;38:906-910.
- Sudlow CLM, Warlow CP. Comparable studies of the Incidence of stroke and its pathological types. 1997;28:491-499.
- Markus H,‘Stroke causes and clinical features’. Neurology 2008 36(11):586-591.
- Ser T, Barba R, Morin MM, Domingo J, Cemillan C, Pondal M et al. Evolution of cognitive impairment after stroke and risk factors for delayed progression. Stroke 2005;36:2670-2675.
- Rathore SS, Hinn AR, Cooper LS, Tyroler HA, Rosamond WD. Characterization of Incident stroke signs and symptoms. 2002;33:2718-2721.
- Novitzke J, RN. Privation of memory. Journal of vascular and Interventional neurology 2008;1(4):122-123.
- Wechsler D. Wechsler Memory Scale-Revised Manual. San Antonio, Tx, Psychological corporation, 1987.
- Wechsler D. Wechsler Memory Scale-Revised. San Antonio: The Psychological corporation, 1981.
- Wechsler D. Wechsler Adult Intelligence Memory Scale-Revised. New York: The Psychological Corporation, 1981.
- Sachdev PS, Brodaty H, Valenzuela MJ, Lorentz L, Wen W, Zagami AS. The Neuropsychological profile of vascular cognitive impairment in Stroke and TIA patients. Neurology 2004,62:912-919.
- Burgess IS, Dean M, Lincolin NB, Pearce MJ. Scafold Objective Recognition Test. Nottingham Rehabilitation 1996.
- Warrington EK. Recognition Memory Test. Windsor:NFER-NELSON,1984.
- Fuld PA. Fuld Object Memory Evaluation. Chicago: Stoelting, 1982.
- Blake H, Mckinney M, Treece K, Lee E, Lincolin NB. An evaluation of screening measures for cognitive impairments after stroke.Age and ageing 2002;31:451-456.
- Attkinson RC, Shiffrin RM. Human memory: A proposed system and its control processes. In the Psychology of learning and motivation:11 Oxford, England:1968;7421(08):60422-3.
- G.M.S. NYS, Zandvoort MJE, Kort PLM, Jansen BPW, Worp HB, Kappelle LJ, Haan EHF. Domain-specific cognitive recovery after first-ever stroke. Journal of the Neuropsychological Society, 2005,11, 795-806.
- Stebbins GT, Nyenhuis DL, Wang C, Cox JL, Freels S, Bangen K et al. Gray matter atrophy in patients with Ischemic stroke with cognitive impairment. Stroke 2008;39:785-793.
- Burton EJ, Kenny RA, O’Brien J, Stephens S, Bradbury M, Rowan E et al White Matter Hyper-intensities are associated with impairment of memory, attention, and global cognitive performance in older stroke patients. Stroke 2004;35:1270-1275.
- Gillespie DC, Bowen A, Foster JK. Memory impairment following Right Hemisphere stroke. The clinical Neuropsychologist 2006;20:1,59-75.
- Ingles JL, Wentzel C, Fisk JD, Rockwood K. Neuropsychological predictors of incident dementia in patients with vascular cognitive impairment, without dementia. Stroke 2002;33:1999-2002.
- Henon H, Durieu I, Guerouaou D, Lebert F, PasquierF, Leys D. Poststroke dementia: Incidence and relationship to prestroke cognitive decline. Neurology 2001;57:1216-1222.
- Hans-Peter Haring. Cognitive impairment after stroke. Curropin Neurol 2002,15:79-84.
- Rasquin SMC, Lodder J, Ponds RWH, Winkens L, Jolles J, Verhey FRJ. Cognitive functioning after stroke. Dement GeriatrCognDisord,2004;18:138-144.
- Robyn W, MacGregor D, Askalan R, Verber G. Late emergence of cognitive deficits after Unilateral Neonatal Stroke.Stroke 2009;40:2012-2019.
- Jacobs MA, Mitsias P, Soltanian-Zadeh H, Santhakumar S, Ghanei A, Hammond R et al. Multiparametric MRI tissue characterization in clinical stroke with correlation to clinical outcome. Stroke 2001;32:950-957.
- Fregni F, Boggio PS, Nitsche M. Anodal transcranial direct current stimulation of prefrontal cortex enhances working memory. Exp Brain Res 2005;166:23-30.
- Jo JM, Kim Y-H, Ko M-H, Ohn SH, Joen B, Lee KH. Enhancing the working memory of stroke patients using tDCS. Am J Phys Med Rehabil 2009;88:404-409.
- Kaschel R, Della Sella S, CantagalloA, Fahlbock A, Laaksonen R, Kazen M. Imagery mnemonics for the rehabilitation of memory. 2002;12(2),127-153.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





