IJCRR - 9(12), June, 2017
Pages: 23-26
Date of Publication: 24-Jun-2017
Print Article
Download XML Download PDF
Correlation of Stress with Migraine - A Review
Author: Monika Kajal, Manoj Malik, Reena Kumari
Category: Healthcare
Abstract:Migraine is a widespread and debilitating neurological disorder that has been recognized since antiquity. The World Health Organization has listed migraine as a significant public health concern and major cause of years of life with disability. It is aperiodic disorder that comprises paroxysmal and blinding hemicranial pain, nausea/vomiting, photophobiaand phonophobia. Stress is often linked to the occurrence of migraine headaches. Stress may interact with migraine in several ways that predisposed to migraine attacks. Stress is considered as a most common trigger for their attacks and high level of stress are reported in migraine patients. Migraine attacks themselves can act as a stressor, thereby potentially leading to a vicious cycle of increasing migraine frequency. This review provides an overview that both stress and migraine are reciprocally related i.e. cyclically influencing each other across time.
Keywords: Headache, Epidemiology, Trigger factors
Full Text:
Introduction:
Migraine is one of the most common neurological headache disorder and cause of significant disability for many patients1 with substantial personal and societal burden2. The term migraine has been derived from Galen’s usage of hemicranias, to describe “a periodic disorder that comprises paroxysmal and blinding hemicranial pain, vomiting, photophobia, recurrence at regular intervals, and relief by darkness and sleep”3. Migraine is an inherited and episodic disorder that involves sensory sensitivity.
Epidemiology:
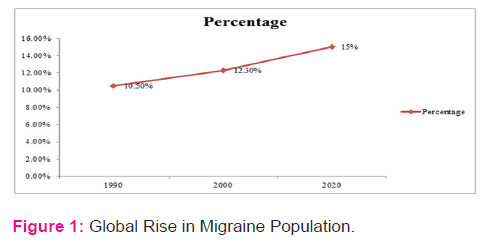
The prevalence of migraine has been extensively studied4. Migraine is ranked 19th among all diseases world-wide that cause disability. The global prevalence of the adult members of the population with an active headache disorder is 11% for migraine5. The prevalence of migraine is age and gender-dependent6. It is more common in boys than in girls before puberty. As adolescence approaches, the incidence and prevalence of migraine increases more rapidly in girls than in boys. In women, prevalence increases throughout childhood and early adult life until approximately age of 40 years, after which it declines4. It is most commonly experienced by individuals between the ages of 15 and 55 years and 70% - 80% of migraineurs have a family history of migraine7. Prevalence rates of International Headache Society - defined migraine are relatively consistent in Western countries, varying from 4% to 9.5% in men and from 11.2% to 25% in women21. In United States population prevalence of migraine is approximately 18% in women and 6% in men that affects 28 million Americans. The data of United Kingdom shows that the overall prevalence of migraine ranged from 3.7% to 4.9%. In Saudi Arabia prevalence for migraine in subjects aged 6 to 15 years was 6.2%. Migraine prevalence was inversely related socioeconomic status4. The prevalence of migraine in London was 28.7%.in women and 19.5% in men. In the Isles of Scilly the prevalence was 23.7 and 15.2% respectively8. In India prevalence was greater among females 31.6% than males 18.5% for migraine subjects aged between 35-45 years in both genders22. In the global burden of disease 1990, these disorders accounted for 10.5% of the worldwide from all diseases and injuries and the re-estimate of global burden of disease 2000 was 12.3% and it is evident that this burden will increase rapidly in the future, with projections indicating 15% by the year 202021.Global figures reveals a rapid rise in migraine, it is shown in figure 1.
Types:
International Headache Society has laid down the criteria which classifies migraine on the basis of International Classification of Headache Disorders9. Classic migraine (migraine with aura) denotes the syndrome of headache associated with characteristic premonitory sensory, motor, or visual symptoms; common migraine (migraine without aura) has no focal neurologic symptoms precede the headache. Complicated migraine is generally describing migraine associated with dramatic focal neurologic features, thus overlapping with classic migraine3. Migraine may be divided in to 2 broad groups based on the number of headache days. If attacks occur less than 15 days per month then termed as episodic migraine (or simply migraine), while headaches occur on 15 or more days per month the terms chronic or transformed migraine20.
Etiology:
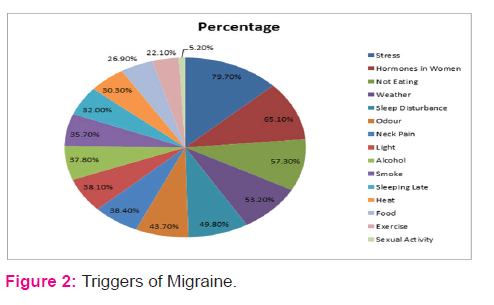
Migraine is a complex genetic disorder with heritability estimates as high as 50%11 and associated with chromosome 1 and 19. Chromosome 19p13 gene mutation is linked to CACNA1A (calcium voltage-gated channel subunit alpha 1 A) and chromosome 1q23 gene mutation linked to Na/K+ ATPase. Dysfunction of neuronal calcium channel might impair serotonin release and predispose patients to migraine12,13. Psychophysical and neurophysiological studies have provided clear statement that the migraine sufferer’s brain stays in a continual state of neuronal hyperexcitabilty7. Migraine pain is caused by inflammation and dilation of meningeal arteries located within dura mater as stated in trigeminovascular hypothesis. Migraine attacks may be precipitated by a number of constitutional and environmental factors, which are often termed migraine triggers1,17. Common migraine triggers are stress1,10,14,15,16,17, hormonal changes in women1,15, certain foods (cheese, chocolate, fruit)1,10,15, missing meals1,15, sleep disturbances, weather changes, alcohol1,10,15, minor trauma10, strong smells, bright light10,15, neck pain, exercise, sexual activity, smoking, heat15. Frequencies of triggers percentage are given in figure 215.
Signs and symptoms:
The sign and symptoms of migraine seem to differ with age. Migraine attacks in children and adolescents differ from those in adults, as the younger often have attacks of shorter duration and bilateral location3. Migraine attack consists of four phases that include premonitory prodrome, aura, headache and postdrome7. Frequency of attacks varies enormously, one or two attacks per months is a common pattern. Repeated episodes of headache (4-72 h) with any two of the features i.e. unilateral, throbbing, worsened by movement, moderate or severe or any one i.e. nausea/vomiting, photophobia and phonophobia are the most characteristics clinical phenotype of migraine23. Typically pain is unilateral and significant number of cases becomes bilateral often, late in an attack. Headache build up to maximum over about 30 minutes and last from hours to one or two days. In majority of cases nausea occurs but in about 50% is there vomiting. Vasomotor changes includes pale face, cold extremity, may be subconjunctival hemorrhage or bruising around eyes. Visual disturbance usually homonymous lasts for 15 to 20 minutes. Symptoms of paraesthesiae and numbness occur in cortical distribution, involving the periphery of the limbs and circumoral region. The lip, face, and tongue may be subsequently affected on one side on one or both sides. Aphasia is usually of the expressive type and accompanied by dysgraphia. The characteristic feature of migraine attacks is the slow speed of the developing neurological disturbance at a rate of about 3 mm/minutes10.
Discussion:
Stress is viewed as a transactional process between an individual and his or her environment in which the individual makes a response to an internal or external constraint. It is trigger for migraine attacks, and is present in approximately 70% of individuals. High levels of stress are reported in migraine patients, particularly in those suffering from chronic daily migraine. Both endogenous (eg, hormone) and exogenous (eg, physical stressors [eg, light]), or psychological stressors add to the burden of the disease. Emotional or physical trauma (eg, abuse, particularly in childhood), and socioeconomic or social stress are examples of psychological stressors16. A study done by Kelman L et al 2007, evaluate and define the triggers of the acute migraine attack. One thousand two hundred and seven patients were evaluated, of whom 75.9% reported triggers (40.4% infrequently, 26.7% frequently and 8.8% very frequently). Study concluded that the trigger frequencies of stress in migraine were 79.7% and triggers were more likely to be associated with a more florid acute migraine attack and stress was one of the most common trigger15.Biology of stress and migraine may be linked on several levels. The first of these is the physiological stress response, which involves both the hypothalamic-pituitary-adrenocortical axis, and sympathetic nervous system including adrenal medulla. Activation of both these system leads to the behavioral and physiological changes observed in response to stress, and these in turn could potentially trigger migraine attacks1. A study done by Martenson M.E et al 2009, indicate that the neural circuitry responsible for stress-induced hyperalgesia. The dorsomedial nucleus of the hypothalamus is a critical component of the central mechanisms mediating neuroendocrine, cardiovascular and thermogenic responses to various stressors. It also contributes to stress-induced hyperalgesia through direct and indirect connections with the rostral ventromedial medulla, a region long implicated in descending control of nociception24. Sauro K.M et al 2009, reported that chronic stress leads to hyperalgesia may include potential mechanism of N-methyl-D-aspartate receptors and the µ-opioid receptor activation. Another way that chronic stress may physiologically impact headache is through alteration of the immune system in such a way that pain transmission is facilitated at the neuronal level and inflammatory mediators such as tumor necrosis factor alpha, interleukin-1 beta, interleukin-6, and nitrous oxide may act as pain mediators that can sensitize the pain matrix1. Schoonman G.G et al 2007, studied the temporal relationship between changes in stress-related parameters and onset of a migraine attack. Study concluded that stress-sensitive patients, in contrast to non-sensitive patients, may perceive more stress in the days before an impending migraine attack14.WacogneC et al 2003, study investigated the intensity of stress, anxiety and depression. Stress was measured using the Perceived Stress Questionnaire, and anxiety and depression using the Hospital Anxiety and Depression Scale. Study concluded that stress is a primordial factor in the triggering and perpetuation of migraine attacks. Women and men display differences in the prevalence of many disorders that could be considered to be stress- related, including migraine18. A study was done by Hedborg K et al 2011, Study was performed on 150 persons, 106 women and 44 man, suffering from at least two migraine attacks a month. All of them answered validated questionnaires regarding personality traits of Swedish universities scale of personality, life events, and perceived ongoing stress. There were high mean scores for psychic and somatic anxiety in women. Study showing that stress is an important factor in migraine. Stress susceptibility, life events, and concomitant psychosomatic illnesses should be considered important when evaluating individuals with migraine, and gender aspects need to be taken into account17. Some studies shows temporal relationship with stress in migraine. A study done by Holm J.E et al 1997, objective of study was examined daily temporal relationships between stress, cognitive appraisal, coping, and migraine. Studied concluded that stress and migraine are reciprocally related (i.e. cyclically influencing each other across time) along with cognitive appraisal and coping are also related to migraine activity in reciprocal fashion19.
Conclusion:
Based on comprehensive literature review it is concluded that stress is a major trigger for migraine attacks and high level of stress are reported in migraine patients. Both stress and migraine are reciprocally related i.e. cyclically influencing each other across time. Thus stress management approaches like cognitive behavioral therapy, various forms of biofeedback and relaxation training can also be incorporated during migraine treatment along with pharmacotherapy.
Acknowledgement:
I hereby acknowledge my co-authors and Jaspreet Kaur for constantly encouraging and supporting and helping me find my literature for this review article. Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
Source of Funding: None
Conflict of interest: There is no conflict of interest.
References:
- Sauro K.M, Becker W.J. The stress and migraine interaction.Headache. 2009;1378-1386.
- Lipton R.B, Buse D.C, Hall C.B, Tennen H, Defreitas T.A, Borkowski T.M et al. Reduction in perceived stress as a migraine trigger. Neurology. 2014;82:1395-1401.
- Rowland L.P. Merritt’s Neurology.10thed. Philadelphia (USA).Lippincott Williams and Wilkins.2000;807-810.
- Lipton R.B, Bigal M.E. Migraine: Epidemiology, impact, and risk factors for progression. Headache. 2005;45:1-3.
- Yavuz B.G, Aydinlar E.I, Dikmen P.Y, Incesu C. Association between somatic amplication, anxiety, depression, stress and migraine. The Journal of Headache and Pain. 2013;14:53.
- Breslau N, Rasmussen B.K. The impact of migraine. Neurology. 2001;56:4-12.
- Capers T. Pathophysiology of migraine. MSN Student Scholarship. 2014;46.
- Waters W.E,O'connor P.J. Prevalence of migraine. Journal of Neurology, Neurosurgery, and Psychiatry.1995;38:613-616.
- International Headache Society. The International Classification of Headache Disorders, 3rd edition (beta version).Cephalalgia. 2013;33(9):613-808.
- Donaghy M. Brain’s diseases of the nervous system. 12th ed. Oxford university press.2009;108-112.
- Pietrobon D, Moskowitz M.A. Pathophysiology of migraine. Annu. Rev. Physiol. 2013;75:365-391.
- Bussone G. Pathophysiology of migraine. 2004;25:239-241.
- Cutrer F.M et al. Pathophysiology of migraine. Semin Neurol. 2010;30:120-130.
- Schoonnman G.G, Evers D.J, Ferrari M.D. Is stress a trigger factor for migraine. Psychoneuro endocrinology. 2007;32(5):532-538.
- Kelman L. The triggers or participants of the acute migraine attack. Cephalalgia. 2007;27(5):394-402.
- Maleki N, Becerra Lino, Borsook D. Migraine: Maladaptive brain responses to stress. Headache. 2012;52:102-106.
- Hedborg K, Anderberg U.M, Muhr C. Stress in migraine: personality-dependent vulnerability, life events, and gender are of significance. Upsala Journal of Medical Sciences. 2011;116:187-199.
- Wacogne C, Lacoste J.P, Guillibert E, Hugues F.C, Jeunne C.L. Stress, anxiety, depression and migraine. Cephalalgia. 2003;23(6):451-455.
- Holm J.E, Lokken C, Myers T.C. Migraine and stress: A daily examination of temporal relationship in women migraineurs. Headache. 1997;37:553-558.
- Bigal M.E, Serrano D, Buse D, Scher A, Stewart W.F, Lipton R.B. Acute migraine medications and evolution from episodic to chronic migraine: A longitudinal population- based study. Headache. 2008;48:1157-1168.
- Leonardi M, Steiner T.J, Scher A.T, Lipton R.B.The global burden of migraine: measuring disability in headache disorders with WHO’s Classification of Functioning, Disability and Health (ICF). J Headache Pain. 2005;6:429–440.
- Kulkarni G, Rao G, Gururaj G, Subbakrishna D.K, Steiner T, Stovner L.J. The prevalence and burden of migraine in india: results of a population-based study in Karnataka state. The Journal of Headache and Pain. 2014;15(1):18.
- Goadsby P.J. Pathophysiology of migraine. Ann Indian Acad Neurol. 2012;15:15-22.
- Martenson M.E, Cetas J.S, Heinricher M.M. A possible neural basis for stress-induced hyperalgesia. Pain.2009;142(3):236–244.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





