IJCRR - 9(12), June, 2017
Pages: 16-18
Date of Publication: 24-Jun-2017
Print Article
Download XML Download PDF
Role of Subcortical Band Heterotopia in Epileptogenesis - Case Report
Author: Neera Samar, Rattilal Meena, Mayank Sharma, Sourav Shristi, Rohit Garg
Category: Healthcare
Abstract:Band heterotopias are one of the rarest groups of congenital disorder that result in variable degree of structural abnormality of brain parenchyma. Band of heterotopic neurons result from a congenital or acquired deficiency of the neuronal migration. We report a case of 15 year old female patient with subcortical band heterotopia in which disease manifested itself in first decade of life without any such family history.
Keywords: Sub ependymal, Focal subcortical, Laminar or band heterotopia
Full Text:
INTRODUCTION
Seizure is an important neurological disorder which can be due to primary and secondary causes .Primary causes of seizures are many a times due to developmental malformations like cerebral heterotopias which are a type of neuronal migration disorder which can be detected by MRI. Heterotopias are generally divided into three groups, depending on the location of the ectopic formations: Sub ependymal, focal subcortical, laminar or band heterotopia(double cortex)2
Band heterotopia is a type of neuronal migration disorder. Neuronal migration is the process in which neurons move from their place of origin to permanent location. They probably result from an arrest in migrational process of neuroblast from the periventricular layer to the cortex, which usually occurs maximally between the seventh and sixteenth gestational week3 or are due to programmed cell death of group of neuroblasts4
The prevelance of band heterotopias with epilepsy is unknown. The associated epilepsy syndrome is variable and seizures may be generalized or focal often suggesting subcortical white matter of frontoparietooccipital region.
Differential diagnosis: Tuberous sclerosis, polymicrogyria, schizencephaly, hemimegalencephaly, lissencephaly-pachygyria spectrum2
CASE REPORT
This is a case of fifteen year old girl who was admitted to the medicine department of RNT MC Udaipur with history of on & off seizures; which were generalized tonic clonic seizures. She had been given some medication by local doctors but her symptoms persisted despite that .So her parents brought her at R.N.T. Medical college, Udaipur. She had history of five episodes of abnormal tonic clonic movements of body without fever/trauma, each episode was accompanied with classical frothing from mouth, deviation of angle of mouth, tongue bite with urinary incontinence. She presented with low IQ and had history of seizures for last 7 yrs.
Her neurological examinations was also abnormal. Her MMSE score was 22/30,no cranial nerve palsy, in motor examination her tone was normal, power of both upper and lower limb were 5/5,bilateral plantar flexor, DTR normal, no neck rigidity ,normal gait & no cerebellar signs. Other system on clinical examination were normal. At the time of seizure during hospital stay, urgent electrolytes(Na=136,K=3.8,Ca=9.4),ABG and blood sugar(RBS=137) were tested immediately to rule out common reversible causes of seizure. In RNT MC all the routine investigations were performed in which :
S.VitB12 was in lower than normal limits, s vit b12=183.30pg/ml(N=211-911 pg/ml). Hb=12.1gm/dl; WBC=6540/mcl; Pltcount=271000/mcl; PBF=NCNC;
RBS=93mg%;Serum UREA=18.35mg%;
Serum CREAT=0.76mg%;CRP=0.45mg/l(negative);RA factor negative qualitatively; serum TSH=3.840mIU/ml; Coombs direct and indirect test are negative. Chest xray PA view and ECG were normal.
EEG report of the patient showed normal awake EEG Record.
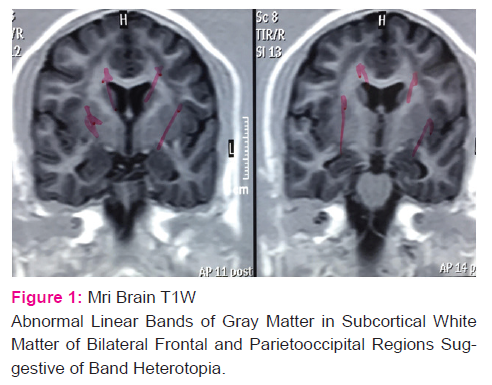
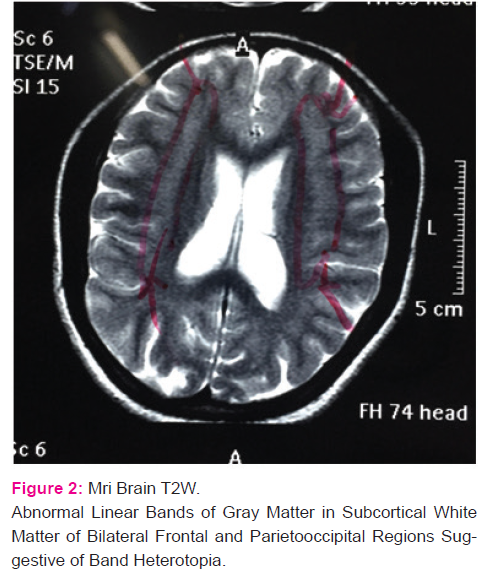
MRI scan of the brain showed abnormal linear bands of gray matter in subcortical white matter of bilateral frontal and parieto occipital regions suggestive of band heterotopia. This band was surrounded by normal white matter. No other significant abnormalities were found on MRI scan.
Based on this finding, diagnsosis of band heterotopia was made which is a rare entity. After the diagnosis was made patient was started on oral anti epileptic drugs ;sodium valproate and phenobarbitone; for last one month she is not having any complaints.
DISCUSSION:
Heterotopias are generally divided into three groups, depending on the location of the ectopic formations: Sub ependymal, focal subcortical, laminar or band heterotopia(double cortex)2 Band heterotopia is a type of neuronal migration disorder. Neuronal migration is a the process in which neurons move from their place of origin to permanent location. They probably result from an arrest in migrational process of neuroblast from the periventricular layer to the cortex, which usually occurs maximally between the seventh and sixteenth gestational week3 or are due to programmed cell death of group of neuroblasts4. The prevelance of band heterotopias with epilepsy is unknown. The associated epilepsy syndrome is variable and seizures may be generalized or focal often suggesting subcortical white matter of frontoparietooccipital region.
In our case patients antenatal history was insignificant and presented with off and on history of grand mal epileptic seizures for last seven years presenting, with MMSE Score22/30 & rest of neurological examination/investigation being normal with MRI findings of subcortical band heterotopias in white matter bilaterally, frontoparietoccipital region. She was diagnosed as case of epilepsy, subcortical band heterotopias, discharged on antiepileptic drugs with control of seizures.
Differential diagnosis could be Tuberous sclerosis, polymicrogyria,
schizencephaly, hemimegalencephaly, lissencephalypachygyria
spectrum2.
During gestational period successive waves of primitive neuroblasts migrate from the germinal matrix to form the cerebral cortex and dep nuclei of the brain between 2-4th month of gestation. Collections of normal neurons in abnormal locations, results from arrest of radial migration of neuroblast, found in gray matter. Band heterotopias is a rare variety of neuronal migration syndrome, usually as a band of gray matter between the lateral ventricle and cerebral cortex and surrounded by normal appearing cortex.These patients have bilateral circumferential and symmetrical ribbons of gray matter located just beneath the cortex and separated from it by a thin band of white matter which led to term “DOUBLE CORTEX SYNDROME”. These patients usually present with behavioural problems, mild mental retardation and seizure disorders in infancy. However, intelligency can be normal and seizure may begin latter in life.
A related syndrome, X linked liscencephaly and SBH also occur in which homozygous males have liscencephaly and heterozygous female have SBH. Recent studies have identified two genes that are linked to these syndromes. One L1S1,maps to chromosome 17p13 and encodes a protein that function as a regulatory subunit of Platelet activating factor acetyl hydrolase, which degrades platelet activating factor and is involved in microtubule dynamics. With regard to its latter role Platelet activating factor acetyl hydrolase controls the distribution and function of the microtubule motor dyenin, thereby controlling the movement of the nucleus during neuronal migration. Studies of mice with targeted LIS1 mutation suggests that this protein is necessary for normal pyramidal cell migration and neurite overgrowth. Another gene DOUBLE CORTIN is located on the X chromosome and is mutated in patient with X linked lisencephaly and SBH. The protein product of DOUBLE CORTIN is highly expressed in fetal neurons and their precursors during cortical development. Like Platelet Activating Factor Acetylhydrolase DOUBLE CORTIN protein is associated with microtubules, suggesting that it is also involved in cell migration5.
References:
1. Band heterotopia.(Alam MS1, Naila N ,J Ayub Med CollAbbottabad. 2010 Apr-Jun;22(2):208-9).
2. Heterotopias: classification and differential diagnosis in pediatric MRI C-0067 ;ECR 2013 ;Educational Exhibit ;I. Villar Blanco, I. MotaGoitia, M. Velasco Ruiz, M. D. C. GarcíaVázquez, J. A. Alvarado Rosas, L. Cubillo De Olazabal; Madrid/ES ;Dysplasias, MR, Neuroradiology brain 10.1594/ecr2013/C-0067 .
3. Rakic P(1978) Neuronal migration and contact guidance in the primate telencephalon,Postgrad med/54:25/40
Rakic P (1995) Radial vs Tangential migration of neuronal clones and the the developing cerebral cortex Proc Natl Acad Sci USA 92:11,323-7
4. Kuida et al(1996) Decreased apoptosis in the brain and prematute lethality in CPP32 deficient mice.Nature 384:368-372
5. Larsen's Human Embryology(By Gary C. Schoenwolf, Steven B. Bleyl, Philip R. Brauer, Philippa H. Francis-West)5th edition Pg-228
6. Barkovich AJ, Subcortical heterotopia: a distinct clinicoradiologicentity. AJNR Am J Neuroradiol 1996;17:1315–22.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





