IJCRR - 5(13), July, 2013
Pages: 99-104
Date of Publication: 17-Jul-2013
Print Article
Download XML Download PDF
INCIDENCE OF HIV INFECTION AMONG KNOWN PULMONARY TUBERCULOSIS PATIENTS AND PULMONARY TUBERCULOSIS AMONG KNOWN HIV SEROPOSITIVE INDIVIDUALS; AND A COMPARATIVE STUDY OF ZIEHL-NEELSEN STAINING AND AURAMINE-O STAINING
Author: S. Saraswathi, T.V. Ramani, Supriya Panda
Category: Healthcare
Abstract:To know HIV seropositivity among known pulmonary tuberculosis individuals and sputum smear positivity for acid fast bacilli among known HIV seropositive individuals and to do a comparative study of Ziehl-Neelsen staining and Auramine-O staining. Methods: 500 symptomatic patients attending to Designated Microscopic Centre were screened for pulmonary tuberculosis by doing Ziehl-Neelsen staining of sputum samples. Sputum smear positive individuals were screened for HIV antibodies. 500 individuals attending to Integrated Counseling and Testing Centre were screened for HIV antibodies according to National AIDS Control Organization guidelines. HIV seropositive individuals were screened for pulmonary tuberculosis by doing Ziehl-Neelsen stain of sputum smear. Auramine O staining was done for randomly selected sputum samples. Results: Incidence of pulmonary tuberculosis was 15.2 %, and among them 5.3 % were HIV seropositive. Incidence of HIV infection was 16.2 %, out of them two were having pulmonary tuberculosis. Out of 50 sputum smear samples selected randomly, 32 were positive for acid fast bacilli in Ziehl-Nelseen stain, 34 were positive by Auramine O stain. Conclusion: In the present study incidence of HIV infection among pulmonary tuberculosis patients was 5.2% and pulmonary tuberculosis among HIV infected individuals was 2.5%. Auramine O stain for detecting M. tuberculosis was more sensitive than Z-N stain.
Keywords: HIV- TB Co-infection, Auramine-O staining
Full Text:
INTRODUCTION
Global annual incidence of Tuberculosis (TB) is 8.5 to 9.2 million in 2010 as per the WHO global TB report 2011with 1.1 million deaths among HIV negative cases of TB and an additional 0.35 million deaths among people who were HIV positive (1). Though India is the second most populous country in the world, India has more new tuberculosis cases annually than any other country. In India annual incidence of TB is 2 million, thus contributing to a fifth of the global burden of TB. It is estimated that about 40% of Indian population is infected with Mycobacterium tuberculosis, but only 10% of them develop disease in life time. Co-infection with HIV increases the risk of developing TB by 5-6 times. Other factors, which increase the risk of TB, are Diabetes mellitus, smoking, malnutrition, silicosis, malignancy, indoor air pollution, poor ventilation, overcrowding, urbanization, migration and poverty. India is third highest HIV burdened country. In India TB is one of the earliest opportunistic diseases to develop among HIV infected individuals, one million people are co infected with TB out of 2.47 million people living with HIV/AIDS (PLHAs) (1). It is the most common opportunistic infection and cause of mortality among PLHAs, difficult to diagnose and treat owing to challenges related to comorbidity, pill burden, co-toxicity and drug interactions. Other way, the incidence of HIV infection in tuberculosis patients varied between states ranging from 0.4 to 20.1 % in India and on average 5% of tuberculosis patients were estimated to be HIV positive (2-12). AIM The present work was taken up to know the incidence of HIV infection in open cases of pulmonary tuberculosis (those who were sputum smear positive) and also to know the incidence of pulmonary tuberculosis by doing Ziehl-Neelsen (Z-N) stain of sputum smear in HIV seropositive individuals. In addition, a comparative study of sputum positivity for M.tuberculosis by two different staining methods, Z-N and fluorescent staining by Auramine O (AO) was taken up.
MATERIALS AND METHODS
Study group: 500 patients suffering from cough and fever for more than 2 weeks attending to Designated Microscopic Centre (DMC) at Maharajah’s Institute of Medical Sciences (MIMS), Nellimerla, Vizianagaram, Andhra Pradesh.500 patients attending Integrated Counseling and Testing centre (ICTC) at MIMS were included in the study after taking written consent from them to undergo the necessary investigations. Study period: For a period of one year from Nov 2009 to Oct 2010. Specimen collection: Two consecutive sputum samples (one spot and one early morning) were collected from each individual attending DMC and HIV seropositive individuals from ICTC.5ml of venous blood was collected from each individual attending ICTC and from those who were acid fast bacilli (AFB) positive in DMC. Both the samples were processed on the same day of collection. Processing: Sputum samples: Smears were prepared from all the specimens collected and stained by ZN stain.50 sputum smears were selected randomly and stained by AO stain. Blood samples: Serum was separated and subjected to HIV antibody testing by using different ELISA kits as per NACO guidelines.
RESULTS
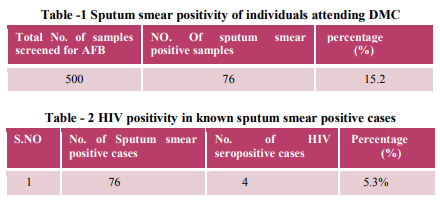
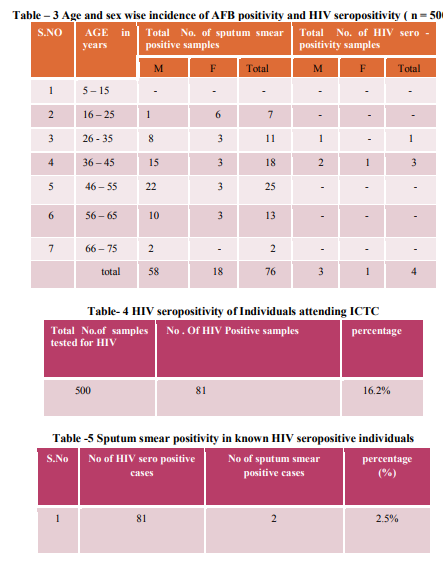
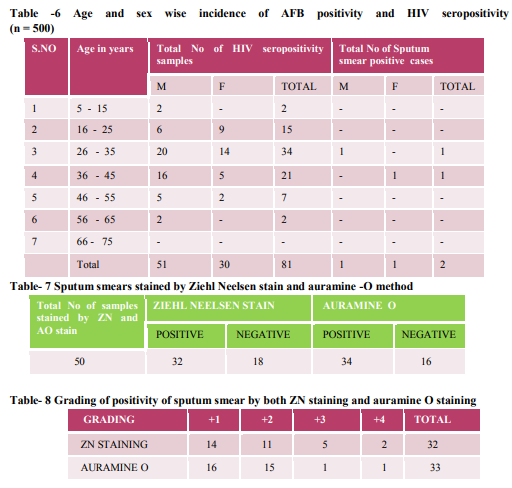
Out of 500 patients attending to DMC at MIMS general Hospital, 76 individuals were sputum smear positive (15.2%) for AFB. Out of 76 sputum smear positive cases, four were HIV seropositive (5.3%). Incidence of pulmonary tuberculosis was more in 46-55 year age and in males. Incidence of HIV infection among pulmonary tuberculosis patients was higher in 36- 45 year age and in males. Out of 500 individuals attending ICTC at MIMS, 81 were found to be positive for HIV antibodies (16.2%). Out of 81 HIV seropositive cases only 2 were found to be sputum smear positive for AFB (2.5%). Incidence of HIV infection was more in 26 -35 year age and in males. Out of 50 sputum samples which were selected randomly, 32 were Ziehl-Nelseen stain positive and 34 were positive by Auramine O stain for M. tuberculosis.
DISCUSSION
A total number of 500 sputum samples over a period of one year from November 2009 to October 2010 were screened for AFB by doing ZN stain. Out of them 76 samples (15.2%) were positive for AFB and maximum incidence was observed in between 46- 55 year age. Percentage incidence of HIV seropositivity in sputum smear positive individuals in the present study was 5.3%, which is higher compare to other studies from India and WHO data. WHO estimated annual rate of tuberculosis among HIV infected is 3.8% (13, 14, 15 ). Out of 500 individuals screened, 81(16.2%) were positive for HIV -1 antibodies and two individuals out of 81 HIV positive were sputum smear positive (2.5%) for AFB in the present study .This is lower than the other studies from India. This low incidence may be due to exclusion of extrapulmonary tuberculosis in the present study (16). In the present study the efficacy of fluorescent staining was found to be more compare to ZN stain and this is as per with the different studies from India (17, 18,19). SUMMARY AND
CONCLUSION
1. Out of 500 sputum smears screened for AFB by ZN staining, 76 individuals (15.2%) were found to be positive for AFB . HIV seropositivity among these sputum smear positive individuals was found to be 5.3%. 2. Out of 500 serum samples screened for HIV antibodies, 81 (16.2%) were found to be HIV seropositive. Sputum smear positivity among these HIV infected individuals was found to be 2.5%. 3. Out of 50 sputum smears selected randomly, thirty two were positive by ZN method and thirty four were positive by Auramine O stain for AFB. So AO staining was found to be more useful for detection and grading than ZN method.
ACKNOWLEDGEMENT
Authors acknowledge the great help received from the scholars whose articles cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. Authors are grateful to IJCRR editorial board members and IJCRR team of reviewers who have helped to bring quality to this manuscript.
References:
1. TB India. RNTCP, 2012, Annual Status Report.
2. Sharma SK, Saha PK, Dixit Y, Siddaramaiah NH, Seth P,Pande JN. HIV Seropositivity among adult tuberculosis patients in Delhi. Indian J Chest Dis Allied Sci 2000; 42: 157- 60.
3. Solomon S, Anuradha S, Rajasekaran S. Trend of HIVinfection in patients with pulmonary tuberculosis in south India. Tuber Lung Dis 1995; 76: 17-9.
4. Paranjape RS, Tripathy SP, Menon PA, Mehendale SM, Khatavkar P, Joshi DR, et al. Increasing trend of HIV seroprevalence among pulmonary tuberculosis patients in Pune, India. Indian J Med Res 1997; 106: 207-11.
5. Samuel NM, Alamelu C, Jagannath K, Rajan B. Detection of HIV infection in pulmonary tuberculosis patients. J Indian Med Assoc 1996; 94: 331-3.
6. Sharma SK, Aggarwal G, Seth P, Saha PK. Increasing HIV seropositivity among adult tuberculosis patients in Delhi. Indian J Med Res 2003; 117: 239-42.
7. Mohanty KC, Nair S, Sahasrabudhe T. Changing trend ofHIV infection in patients with respiratory disease inBombay since 1988. Indian J Tuberc 1994; 41: 147-50.
8. Mohanty KC, Basheer PMM. Changing trend of HIV infection and tuberculosis in a Bombay area since 1988.Indian J Tuberc 1995; 42: 117-20.
9. Purohit SD, Gupta RC, Bhattara VK. Pulmonarytuberculosis and Human Immunodeficiency Virus infection in Ajmer. Lung India 1996; 14: 113-20.
10. Banvaliker JN, Gupta R, Sharma DC, Goel MK, KumariS. HIV seropositivity in hospitalized pulmonary tuberculosis patients in Delhi. Indian J Tuberc 1999; 44:17-20.
11. Gupta PR, Luhadia SK, Gupta SN, Joshi V. Tuberculosis in human immunodeficiency virus seropositives inRajasthan. Indian J Tuberc 1998; 16:147-9.
12. Talib SH, Bansal MP, Kamble MM. HIV-1 seropositivity in pulmonary tuberculosis (study of 340 cases from Marathwada). Indian J Pathol Microbiol 1993; 36: 383-8
13. Dr. V. Sivaraman and Dr. Gilbert Fernandez, TB Sanatorum, Gorimedu, Pondicherry, Dr. R. Sambasiva Rao AIDS Surveillance Centre, JIPMER, Pondicherry. Indian J Tuberculosis.1992; 39:35-39.
14. S.K. Sharma, P.K. Saha, Yogita Dixit, Naveen H. Siddaramaiah, Pradeep Sethand J.N. Pande Departments of Medicine and Microbiology, All India Institute of Medical Sciences, New Delhi, HIV Seropositivity Among Adult Tuberculosis Patients in Delhi. India Indian J Chest Dis Allied Sci 2000; 42: 157-160.
15. Deswal B.S, D. Bhatnagar, D. Kumar, VR Deshpande, A Study of Prevelance of HIV in Tuburculosis Cases. Indian Journal of Community Medicine. Vol. 27, No. 2 (2002-04 - 2002-06)
16. Piramanayagam.P, Mohammad Tahir, S.K. Sharma, Duncan Smith-rohrberg, A. Biswas and M. Vajpayee. Persistently high HIV seroprevalence among adult tuberculosis patients at a tertiary care Centre in Delhi. Indian J Med Res. February 2007; 125 163- 166.
17. Singh N P, Parija S C. The value of fluorescent microscopy of auramine stained sputum smears for diagnosis of pulmonary Tuberculosis.Southeast Asian J Med Public Health 1998 Dec; 29 (4): 860.
18. Prasanthi. K , Kumari A R, Efficacy of flurochrome staining in the diagnosis of pulmonary tuberculosis Co infected with HIV. Indian Journal of Medical Microbiology. 2005.Vol 23,No 3,179-185
19. Kumar N, Tiwari M C, Verma K AFB staining in cytodiagnosis of Tuberculosis without classical features: A comparison of Zeihl- Neelsen and fluorescent methods.Cytopathology,1998 May;vol 9 (3):208 -214.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





