IJCRR - 5(13), July, 2013
Pages: 88-92
Date of Publication: 17-Jul-2013
Print Article
Download XML Download PDF
THE INCIDENCE OF OSSIFIED SUPERIOR TRANSVERSE SCAPULAR LIGAMENT (STSL) IN TAMIL NADU POPULATION OF INDIA
Author: A. Perumal, Ravichandran D.
Category: Healthcare
Abstract:Background: Suprascapular neuropathy is due to suprascapular nerve entrapment in the suprascapular foramen and it is one of the causes for chronic shoulder pain and dysfunction. The suprascapular notch in the superior border of the scapula is usually bridged by the Superior Transverse Scapular Ligament (STSL). Sometimes the ligament gets ossified and compresses the suprascapular nerve passing deep to it producing the characteristic symptoms of compression neuropathy. The incidence of the ossified STSL varies in different ethnic populations. This study attempts to delineate the incidence of ossified STSL in Tamil Nadu population of India. Materials and Methods: Two hundred and thirty seven (237) dry human scapulae were studied. The presence of ossified STSL noted by macroscopic examination with naked eye. Results were tabulated and statistical analysis done. Results: 9.7% of bones show complete ossification of STSL and 10.9% of bones showed partial or incomplete ossification of STSL. Conclusion: The knowledge of incidence of ossified STSL is essential for surgeons performing surgical decompression of the entrapped supra scapular nerve. This paper adds to the morphological data of the Tamil Nadu population, which would be of use to the Orthopedic surgeons working in this area.
Keywords: Scapula, superior transverse scapular ligament, entrapment, decompression, incidence.
Full Text:
INTRODUCTION
The superior border of the scapula in its lateral aspect presents a notch, called the Suprascapular Notch (SN). The notch is converted into a foramen by the Superior Transverse Scapular Ligament (STSL) which bridges the edges of the notch. The Suprascapular Nerve (SSN) passes deep to the ligament whereas the suprascapular vessels pass superior to the ligament. The SSN gives motor innervations to the supraspinatus and infraspinatus muscles and sensory innervations to the rotator cuff muscles and to the shoulder and acromioclavicular joint. Suprascapular nerve neuropathy is a common cause of chronic shoulder pain and dysfunction1 . The suprascapular notch is one of the potential site for compression of the nerve. The condition was first described by Thomas2 in the year 1936. Other etiologies associated with SSN neuropathy include direct trauma, rotator cuff tear, ganglion cysts causing compression, sports injury due to repeated traction, variation of the SN morphology1,3. Apart from these, the ossification of the STSL has also been attributed to be one of the most important cause of SSN compression 4,5,6,7. The knowledge of this clinical condition is essential for the orthopaedic surgeons operating in this area. There is a paucity of information regarding the incidence of ossified STSL in the literature. The present study aims to estimate the incidence of ossified superior transverse scapular ligament in Tamil Nadu population of India. MATERIALS AND METHODS Data for this study are comprised of 237 dry scapulae (Right - 107 and Left - 130) irrespective of sex and age belonging to Tamil Nadu population. The collection was obtained from the bone bank of Anatomy department, VMKV medical college, Salem, India. As criteria of inclusion, none of the scapulae presented fractures, malformations, damage due to conservation or pathologies that could influence the development of the studied region. Each of the scapulae were examined macroscopically for the presence of ossified superior transverse ligament (complete or partial). The results were tabulated and analyzed statistically.
RESULTS
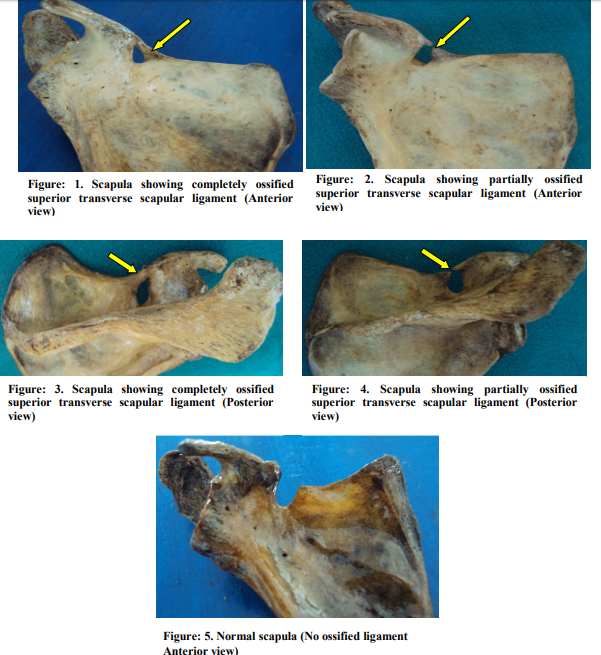
The results are presented in Table 1. Complete ossification of the superior transverse scapular ligament (Fig. 1) was observed in 9.7 % of bones ( 23 bones out of 237). Incomplete or partial ossification of the superior transverse scapular ligament (Fig. 2) was observed in 10.9% of bones (26 bones out of 237).
DISCUSSION
The role of suprascapular nerve entrapment in chronic shoulder pain and dysfunction is well appreciated by Orthopedic surgeons. The morphology of the bony notch altered due to ossification of STSL has been one of the significant causes for entrapment8 . The incidence of ossified STSL has been reported as 1.5% in Finnish population9 , 6.5% in Italian population 10 , 30.76% in Brazilian population 11 and as 10.57% in Indian population 12 . Our study results closely coincide with the results of the other Indian study (Table II). The STSL experiences both compressive and tensile forces. This is indicated by the presence of fibro cartilage entheses13 in the ligament. The incidence of ossification has been noted to increase with age14. This finding indicates that the compressive and tensile forces play a role in the ossification. Research also confirms that the STSL may be calcified partially or ossified completely4,5. Silva 11 has proposed that the pull of muscles and certain habits of life at utilization of the upper limbs are the probable causes of high incidence of calcification in the studied population. Familial cause for calcification has also been described15 . Patients presenting with chronic shoulder pain, dysfunction and wasting of the muscles innervated by suprascapular nerve require surgical decompression of the same. The surgical technique includes direct exploration or arthroscopic release. Arthroscopic release of the STSL is the current trend in the surgical treatment of the suprascapular nerve entrapment neuropathy. The technique of arthroscopic release has been found better when compared to the routine or traditional open release technique16. In arthroscopic release the neurovascular structures and STSL are better visualized and also the procedure is simple and less invasive when compared to direct exploration16. Variation in the STSL as in case of its ossification, the surgical procedure becomes more difficult and risky. Injury to the suprascapular vessels and nerve are the potential risk factors in case of ossified STSL. The choice of instruments (arthroscopic burr VS Kerrison punch) is also to be decided preoperatively in decompressing the suprascapular nerve entrapped due to ossified STSL1,16 . The present study revealed an incidence of 9.7% and 10.9 % of complete and incomplete ossification of STSL respectively. The present study adds to the pre existing data on ossified STSL in Tamil Nadu population and may be useful to the orthopedic surgeons operating in this area.
CONCLUSION
Based on the present study, it can be inferred that the compressive and tensile forces play a role in either partial or complete ossification of STSL. The knowledge of incidence of ossified STSL is essential for surgeons performing surgical decompression of the entrapped suprascapular nerve. The authors recommend cross-sectional studies with large sample size taking into account additional parameters like the age and gender of the bones in future.
ACKNOWLEDGEMENTS
The authors sincerely wish to thank the management, administrators and the Professor and Head of the department of Anatomy of Vinayaka Missions Kirupananda Variyar Medical College, Salem for their whole hearted support and permissions to utilize their resources and conduct this study. The authors acknowledge the great help received from the scholars whose articles cited and included in references of this manuscript. The authors are also grateful to authors/editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. Authors are grateful to IJCRR editorial board members and IJCRR team of reviewers who have helped to bring quality to this manuscript.
References:
1. Vivek Agrawal . Arthroscopy. The Journal of Arthroscopic and Related Surgery 2009; 25 (3): 325-328.
2. Thomas A. La paralysie du muscle sounepineux 1936; 64: 1283-1284.
3. Charalambos P. Economides et al. An unusual case of suprascapular nerve neuropathy: a case report. Journal of Medical Case Reports 2011; 5: 419.
4. Srijit Das, Rajesh Suri, Vijay Kapur. Ossification of Superior Transverse Scapular Ligament and its Clinical Implications. Sultan Qaboos University Medical Journal 2009; 7(2): 157-160.
5. Ticker JB et al. The incidence of ganglion cysts and other variations in anatomy along the course of the suprascapular nerve. J. Shoulder Elbow Surg 1998; 7: 472-478.
6. Lewis OJ. The coracoclavicular joint. J. Anat 1959; 93: 296-303.
7. Harris RI, Vu DH, Sonnabend DH et al. Anatomic variance of the coracoclavicular ligaments. J Shoulder Elbow Surger 2001: 10: 585-588.
8. Rengachary SS, Burr D, Lucas S. Suprascapular entrapment neuropathy: a clinical, anatomical, and comparative study. Part 3: comparative study. Neurosurgery 1979; 5: 452-455.
9. Kajava Y. Uber den Schultergiirtel der Finen. Ann Acad Sci. Fenn. Series A 1924; 21 (5): 1-69.
10. Vallois HV. L’os acromial dans les races humaine. L’Anthropologie, Paris 1925; 35: 977-1022.
11. Silva JG et al. High incidence of complete ossification of the superior transverse scapular ligament in Brazilians and its clinical implications. Int. J.Morphol 2007; 25 (4): 855-859.
12. Jadav SD et al. Supra-scapular foramen in Indian dry scapulae. National Journal of Clinical Anatomy 2012; 1(3): 133-135.
13. Morrigl B. Jax P, Milz S. et al. Fibrocartilage at the entheses of the suprascapular (superior transverse scapular) ligament of man – A ligament spanning two regions of a single bone. J. Anat 2001; 199 (5): 539 – 545.
14. Hrdlicka A. The scapula: Visual observations. Am J Phys Anthropol 1942; 29: 73-94.
15. Cohen SB, Dnes DM, Moorman CT. Familial calcification of the superior transverse scapular ligament causing neuropathy. Clin Orthop Rel Rs 1997; 334: 131-135.
16. Laurent Lafosse, Andrea Tomasi, Gloria Baier et al. Arthroscopic Release of Suprascapular Nerve Entrapment at the Suprascapular Notch: Technique and Preliminary Results. Arthroscopy. The Journal of Arthroscopic and Related Surgery 2007; 23 (1): 34-42.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





