IJCRR - 5(13), July, 2013
Pages: 29-36
Date of Publication: 17-Jul-2013
Print Article
Download XML Download PDF
A STUDY OF VARIATIONS IN THE SHORT SAPHENOUS VENOUS SYSTEM WITH CLINICAL CORRELATION
Author: Anupama D., Nagaraj D.N., B.S. Suresh, R. Lakshmi Prabha Subhash
Category: Healthcare
Abstract:The common liability of the superficial venous system of the lower extremity to varicoses has naturally attracted the attention of Anatomists and Surgeons. Variations in the superficial veins of the lower limb are very common. The extent of such variations, their connections to either the Long or Short saphenous venous systems are usually described. Generally the clinical assessment, including tourniquet tests and Doppler ultrasound, of primary varicose veins presents no problem. However, in some patients the information so obtained is inadequate for appropriate management and difficulties arise because of abnormal communication between the Long and short saphenous veins. Sometimes the main trunks alone are affected and in others only the tributaries are anomalous. In few cases both are involved. In extensive varicose veins, because of overlap of the long and short saphenous territories, it can be difficult to assess which system is involved or whether both are affected. Detailed knowledge regarding the anatomical variations such as reduplication of the long saphenous vein and unusual termination of the short saphenous vein is a prerequisite in the diagnosis and management of varicose veins. Usually the short saphenous vein terminates in the popliteal fossa a few cms above the knee joint, but in almost one half of patients it terminates at a higher or lower level. In this study short saphenous vein terminated at unusual sites is described. Although attention has been mainly directed to the great saphenous vein for the elucidation of the causation of the varicose condition, the study of the small saphenous vein, which phylogenetically is the more important vein, throws light upon the problem.Interestingly variations seen in this study should be kept in mind due to its clinical and surgical significance.
Keywords: Short Saphenous vein, Long saphenous vein, Popliteal vein, Anomalous, Varicoses.
Full Text:
INTRODUCTION
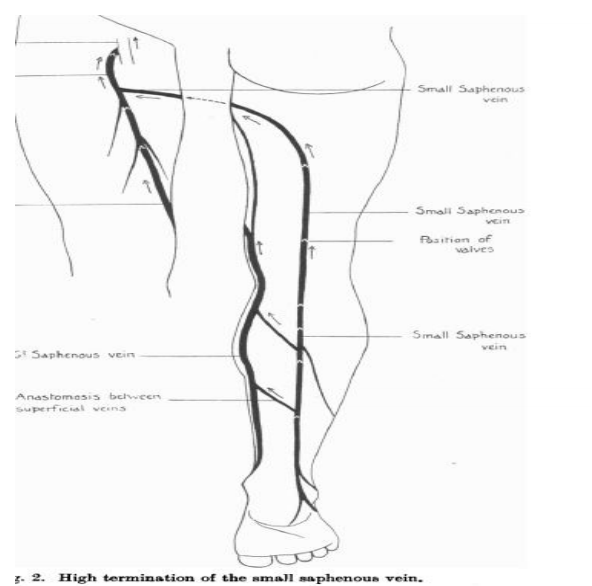
The short(small or lesser ) saphenous vein begins posterior to the lateral malleolus as a continuation of lateral marginal vein. In the lower third of the calf, it ascends lateral to the tendo calcaneus, lying on the deep fascia and covered only by superficial fascia and skin. Inclining medially to the midline of the calf, it penetrates into the deep fascia within which it ascends on gastrocnemius, only emerging between it and the deep fascia gradually at about the junction of intermediate and proximal thirds of the calf. Then it ascends between the two heads of gastrocnemius and proceeds to terminate into popliteal vein. Its mode of termination is variable. Mercier's classification describes six types of terminations: 1: The saphenopopliteal junction is situated 2 to 15 cm above the popliteal crease; this situation is observed in half of all cases; 2: The saphenopopliteal junction is also situated 2 to 15 cm above the popliteal crease, but is prolonged by a trunk which anastomoses with the long saphenous vein; 3: The so-called high saphenopopliteal junction terminates on the posterior aspect of the thigh, in the femoral vein, which communicates with the long saphenous vein; 4: The saphenopopliteal junction does not exist and the short saphenous vein terminates exclusively in the long saphenous vein; 5: The high saphenopopliteal junction terminates on the posterior aspect of the thigh,in the femoral vein; 6: The saphenopopliteal junction is complex, with a number of intramuscular anastomoses. It is important for the surgeons operating the varicose veins to be aware of these unusual modes of termination of short saphenous vein, to allow the surgeon for complete flush ligation of the same failing which recurrence is common.
MATERIALS AND METHODS
50 embalmed lower limb specimens were thoroughly cleaned, carefully dissected and studied in detail. Photographs of the same were taken.
OBSERVATIONS AND RESULTS
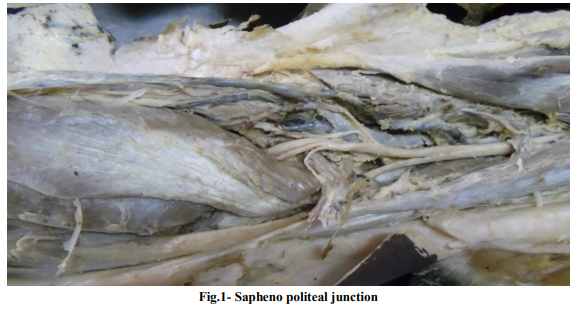
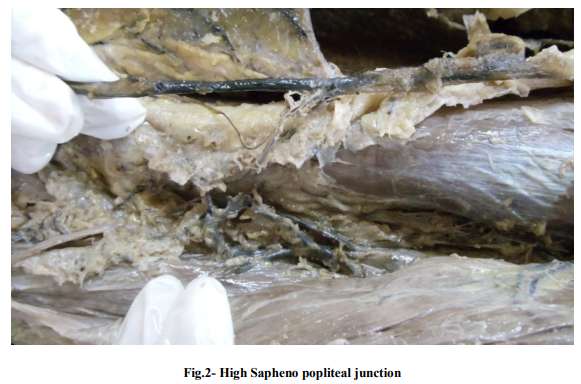
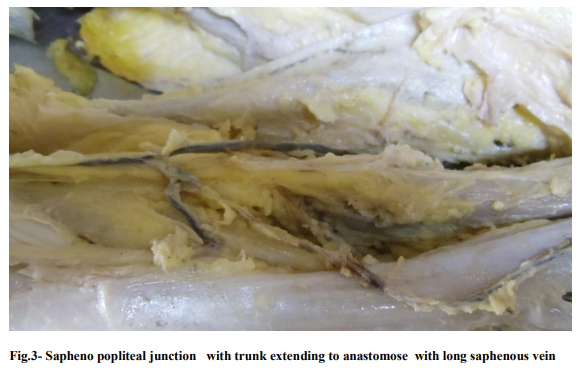
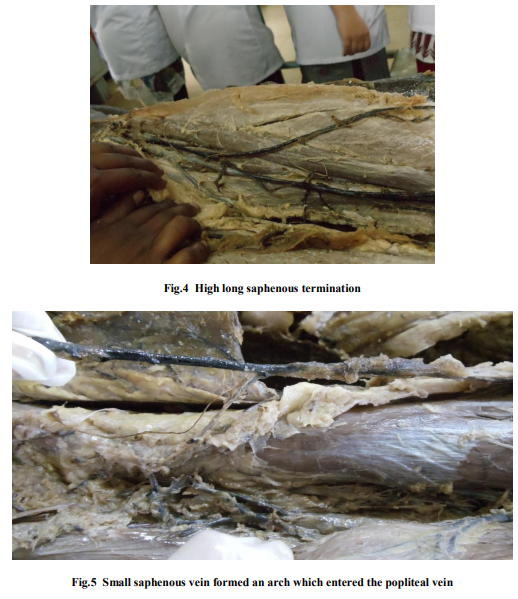
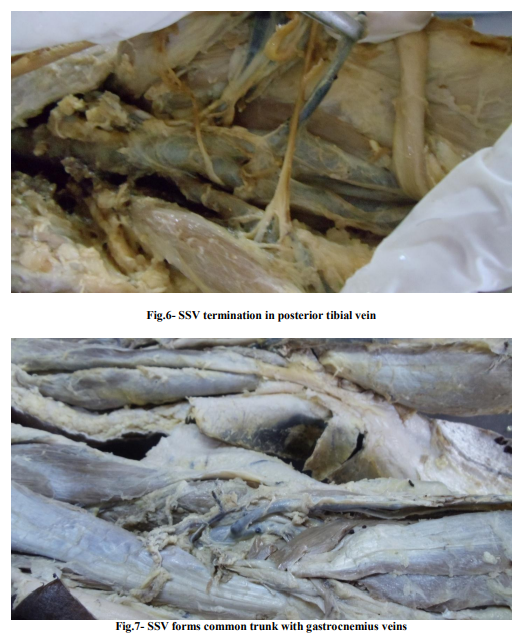
Sapheno politeal junction (Type1) was the most common type of termination as shown in fig 1. The next common mode of termination was high Sapheno popliteal junction (Type 5) which opened in to femoral vein on the posterior aspect of thigh as shown in fig.2. Sapheno popliteal junction with trunk extending to anastomose with long saphenous vein (Type 2) was the third commonest mode of termination as shown in fig. 3. High long saphenous termination only (Type 4) was seen in one of the limbs as in fig.4. Type 3 termination was seen in one case, where in one branch of the small saphenous vein formed an arch which entered the popliteal vein on an average of 4-5 cm. above the knee-joint, just below the middle of the popliteal space. The terminal part of the arch received the small superficial posterior vein of the thigh (v. cut. fem. post. of Meyer, v. femoro-poplitea of Hyrtl). This vein began in the junction of upper and middle third of the thigh, and ran under the deep fascia on the medial side of the sciatic nerve fig.5. In addition, this vein communicated with the deep posterior muscular veins of the thigh. The other branch of short saphenous vein ran round the medial side of the middle of the thigh towards the great saphenous vein. In one of the limbs, it opened directly into the great saphenous vein, just before its termination. In one limb it terminated in posterior tibial vein below the kneejoint fig6. (Type6) In one case, a small cutaneous veins found running down from the popliteal space to join the long saphenous vein which may be regarded as the usual upward continuation of the main trunk. In another case, it trifurcated in the popliteal fossa, one branch opening in to popliteal vein, second joining the posterior deep femoral vein and the third joining the great saphenous vein just above the knee. In two cases, it terminated by forming a common trunk with gastrocnemius veins which further opened in to popliteal vein fig.7and in another it opened in to posterior tibial vein.(Type6)
DISCUSSION
ONTOGENY:
EmbryologIcally the small saphenous vein represents the post-axial vein of the hind limb bud; it is the first vein to appear and originally opens into the internal iliac through the sciatic and gluteal veins. The subsequent transformation into a short vein opening into the popliteal vein, may be an adaptation to the elongation and relative rigidity of the hind limb. This abbreviation of the post-axial vein of the lower extremity is the main difference in the venous system of the fore and hind limbs. Comparative anatomy seems to indicate that the termination of the small saphenous vein into the popliteal vein is an adaptation peculiar to higher mammals including man. In this the small saphenous vein ends exclusively in the popliteal vein.
CLINICAL IMPLICATIONS
Several anatomical studies have described various types of Short saphenous vein termination among which the study of Giacomini stands out. Varicose veins are one of the commonest disease of veins of the lower limb. It affects more than 5% of the adult population in the western countries. More than ½ of adult men and 2/3 of adult women have physically identifiable varicosities. Varicose veins range in severity from the undesirable appearance of venectasia to protuberant tortuous varicosities with or without associated dermatitis, cutaneous ulceration or severe pigmentation. The cause for varicose veins is said to be multifactorial. It is also linked to FOXC2 gene. As a result of anatomical study of the distribution of varicose veins with the aid of investigations, the treatment is usually decided. The present understanding of the anatomy of the area is to allow the selection of treatment on the basis of the probable cause. The particular anatomical and hemodynamic characteristics of veins of the popliteal fossa responsible for a number of therapeutic difficulties which is related to the confluence of popliteal and saphenous collecting vessels and muscle draining veins. The hemodynamic difficulties are to the fact that the popliteal fossa which is the site of very intense pressure variations. As one of the causes for the varicoses is possible variations in the anatomical course of small saphenous vein and its anastomotic channels, it is very important to alienate the varicosity to either short saphenous or long saphenous venous systems. Usually varicoses in the back of the leg with a palpable dialated small saphenous trunk is suggestive of the incompetence of small saphenous vein. Some varicose veins join both the systems where it becomes confusing to define the mode and extent of surgical management. There is some evidence to say that a more accurate surgical approach reduces the incidence of recurrence of varicose vein which is the most common complication. Unless flush ligation is performed, recurrence is likely. Abnormally distributed varices or a suspiscion of lesser saphenous incompetence requires further assement as the termination of the lesser saphenous vein is very variable.8,9 The principles on which the surgical treatment is based, are to ligate the point of communication, the saphenofemoral and /or saphenopopliteal junctions and to remove the major part of the incompetent trunk to prevent connections to the tributaries. The tributaries are then individually removed by making minor cut downs and avulsions. Preoperative ultrasound localization of the junction should ideally be carried. A transverse skin incision is made in the popliteal fossa just below the termination of the vein. The deep fascia is then split to identify vein till sapheno popliteal junction before it is divided. Tributaries may enter the vein just before its termination. After the vein has been divided, careful stripping of the vein is done from above downwards with dissecting off the sural nerve to ensure that the whole of the small saphenous vein is removed. This obliterates the junction with the midcalf perforator vein which is responsible for many recurrences. Recurrent venous reflux in the popliteal fossa with recurrent varicose veins following short saphenous surgery has been reported frequently. 5,6.7. Incompetence of the short saphenous vein was found to be the main source. Recurrent Short saphenous vein varicosity or persistence may be of 4 types Type 1- Intact Sapheno Popliteal Junction as well as Short saphenous vein. Type 2- Varicosities in the popliteal fossa communicating with Short saphenous vein stump. Type 3- Residual Short saphenous vein communicating with the popliteal vein via a tortuous vein. Type 4-Non communicating residual Short saphenous vein. 10 The relation of the arch of the small saphenous vein to the tibial nerve may be important since it explains the obstinate pain in the leg when the veins become varicose, as it is always intimately connected with it. Motor nerve injury (tibial nerve) should not occur if the affected area is carefully displayed during surgical procedures.3 Damage to the other veins and arteries in the vicinity is also avoidable with detailed anatomical knowledge of the region and also helps to prevent recurrence.11 Compartment syndrome is an infrequent but serious complication which can occur post operatively following short saphenous vein surgery where in raised pressure within a tight compartment results in a combination of sensory andmotor symptoms with vascular compromise.12
References:
1. Veins of the lower limbs in Cardio vascular system.In: Susan Standring, Gray’s anatomy. 37th ed, Edinburgh:Churchill Livingstone; p15
2. Hollinsheds surgical anatomy, 4th ed, ch 5, Lower limb as a whole, p 345 .
3. Observations on the superficial venous system of the lower extremity by Charles Kosinski.p131-142.
4. F.P. Keeling andM. Lea Thomas.1987, The British Journal of Radiology,60.235-240.
5. Bailey and Love’s Short practice of surgery.25th ed. Venous disorders. Kevin Burnand. ch54, p9 27-932.
6. Farquharson’s text book of operative surgery.R.F.Rintoul.8th ed, 2002. Churchill Livingstone, p57-63.
7. Carol.E.H, Scott Conner in Operative Anatomy.3rd ed Lippincott Williams.p745
8. Wesley .S. Moore, Vascular surgery- a comprehensive review.6th ed. Ch. 42,Chronic venous insufficiency. Niren angle andJohn.T.Bergan, p826-833.
9. Philippe Blanchemaison, Jerome Camponovo, Short Saphenous TerritoryAnatomy of recurrences following SPJunction ligation- Ectatic gastrocnemius veins.p1-3.
10. Tong Y, Royle J. Recurrent varicose veins after short saphenous vein surgery: a duplex ultra sound study.Cardio vascular surg 1996 Jun;4(3):364-7.
11. S-Y Kim, E-A Park, Y-C Shin Preoperative determination of anatomic variations of the small saphenous vein for varicose vein surgery by 3 dimensional tomography venography.Phlebology28.October 2011 at rsmjournals.com
12. Yousef Shahin,Niteen Tapuria andPeter Lee Chong.Compartment syndrome following short saphenous varicose vein surgery:a case report.Cases Journal 2009;2:7118.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





