IJCRR - 9(11), June, 2017
Pages: 48-52
Date of Publication: 12-Jun-2017
Print Article
Download XML Download PDF
Significance of Aldose Reductase in Diabetic cataract
Author: Geeta Bhatia, Subodhini Abhang, A. N. Sontakke
Category: Healthcare
Abstract:Background: Cataract is a major cause of blindness. Diabetes mellitus is a major risk factor for the development of cataract. Diabetic patients have 25 times higher risk of cataract than non-diabetic population. The metabolic changes accompanying hyperglycemia is increased activity of the polyol pathway and aldose reductase (AR) is a key enzyme of polyol pathway. Aldose reductase is responsible for generation of more oxidative stress by decreasing GSH in diabetic patients which is thought to be a major factor to initiate the process of cataractogenesis. The present study was designed to determine significance of aldose reductase diabetic cataract and its correlation with reduced glutathione (GSH) and Malondialdehyde (MDA) in diabetic cataract patients.
Methods: In this study we measured MDA as oxidative stress marker andGlycated Hb (HbA1c) glycemic index marker levels of GSH and AR in erythrocytes of Type2 diabetic cataract patients (n = 30) and non diabetic senile cataract patients (n=30) compared with age matched normal controls(n=30).
Results: We found increased levels of AR, HbA1c and MDA, and decreased levels of GSH in diabetic cataract patients compared to non diabetic senile cataract patients and normal controls.
Conclusions: From the result it is concluded that AR play a major role in generation of more oxidative stress in diabetic patients which may be the cause of early cataractogenesis in diabetic patients as compared to non diabetic senile cataract patients.
Keywords: Cataract, Aldose Reductase (AR), Malondialdehyde (MDA), Reduced Glutathione (GSH), Glycated Hb (HbA1c).
Full Text:
INTRODUCTION:
Population growth, ageing, urbanization, sedentary lifestyles and an increasing prevalence of obesity are increasing the number of people with diabetes mellitus. The global prevalence of diabetes was estimated to be 2.8% in 2000 and is expected to reach 4.4% by 2030. Cataract is the leading cause of blindness in the world, responsible for 48% of blindness worldwide. A putative cause for age-related cataract is oxidative stress 1 . Chronic hyperglycemia is a major determinant in the development of secondary complications of diabetes, such as diabetic cataract. Evidence indicate that both the duration of diabetes and the quality of glycemic control are the most important risk factors for cataract formation 2. According to WHO survey, India will be the world’s diabetic capital in near future. Globally, cataract remains the leading cause of blindness, affecting approximately 18 million people. Cataract occurs at an earlier age and is 2–5 times more frequent in patients with diabetes, thus the visual loss has a significant impact on the working population 3
Diabetes mellitus is recognized as a leading located in the eye (cornea, retina, lens) is a key enzyme of polyol pathway. Under normal glycemic conditions, only a small fraction of glucose is metabolized through the polyol pathway, as the majority is phosphorylated by hexokinase, and the resulting product, glucose-6-phosphate, is utilized a substrate for glycolysis or pentose phosphate metabolism4. However, in response to the chronic hyperglycemia found in diabetics, glucose flux through the polyol pathway is significantly increased. Up to 33% of total glucose utilization in some tissues e.g. eye can be through the polyol pathway5.
In hyperglycemia excessive amount of glucose is diverted to the polyol pathway, where AR reduces glucose into sorbitol at the expense of NADPH. Sorbitol is as an osmolyte leads to osmotic swelling ,changes in the membrane permeability ,leakage of glutathione, myoinositol ,the generation of free radicals and hydrogen peroxide which primarily causing the diabetic complications such as cataract, retinopathy and neuropathy6. Since NADPH is essential for generation of GSH (intracellular antioxidant) from GSSG, the depletion of NADPH by the AR pathway may impair intracellular antioxidant defence. Sorbitol is then converted to fructose by SDH with the production of NADH, potentially leading to increased ROS via NADH oxidase Activity of aldose reductase is dependent on NADPH. GSH is required for regeneration of NADPH. So indirectly the activity of AR is in turn depends on GSH. So in present study was designed to determine the levels of aldose reductase and GSH and their role in contribution of oxidative stress to diabetic cataract.
MATERIALS AND METHODS:
The study comprises of total 90 subjects were divided into three groups aged between
50 -80 years. The subjects were selected from ophthalmic OPD of B. J. Medical College and Sassoon Hospitals Pune
GROUP I - (n = 30) Senile cataract patients.
GROUP II- (n =30) Diabetic cataract patients and
GROUP II- (n =30) Normal healthy controls
Inclusion criteria – Senile cataract subjects had normal fasting blood glucose level with no history of diabetes. Diabetic cataract subjects having diabetes for last 12-15 years and were using oral hypoglycaemic agents
Exclusion criteria: - Patients with ocular surgery, trauma, infection inflammation of eye, known cases of cardiovascular disorders, rheumatoid arthritis and carcinomas where free radical damages has been commonly incriminated were excluded from the study.
The study was approved by the Institutional Ethics Committee of B.J. Medical college Pune. A written informed consent was taken from the subjects.10 ml of venous blood was collected during preoperative period in plain vacutainer, EDTA and ACD (Acid Citrate Dextrose) bulb under aseptic precaution. Serum and hemolysate was used for investigations.
Blood samples of all three groups were analyzed for following parameters .
Aldose reductase activity (AR) –by Hayman and Kinoshita 1965 7
Glycated Hb (HbA1c) - by Ion exchange resin method 8
Reduced glutathione (GSH) - by Beutler et al.1963 9
Malondialdehyde (MDA) - by Buege and Aust. 1978 method 10
Statistical analysis: The data were expressed as mean ± standard deviation. Mean values were compared by one-way ANNOVA . Differences between comparison groups were considered to be significant where p<0.05. Post hoc donnet test for inter group comparison and correlation was used.
RESULTS:
Table no 1: The mean age of diabetic cataract patients ( Group II) was significantly lowered as compared to controls (Group III),and as compared to senile cataract patients (Group I) (Difference in age in between Senile and control were not statistically significant.
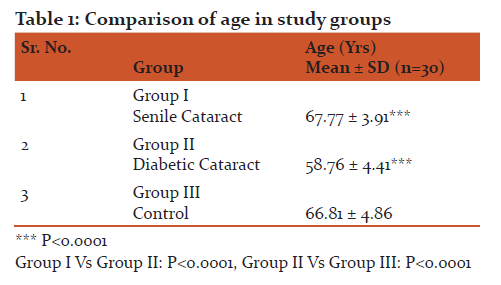
Table no 2: It is observed that the levels of HbA1C were significantly increased in diabetic cataract patients(Group II) as compared to controls (Group III) and the levels of HbA1C in diabetic cataract were significantly higher as compared to senile cataract patients
Difference of mean of HbA1C between senile and control was not statistically significant.
It is observed that activity of AR in diabetic cataract patients were significantly increased as compared to controls .Also activity of AR was significantly higher in diabetic cataract patients as compared to senile cataract patients .
There was no statistically significant difference was seen in activity of AR of senile cataract patients as compared to controls
MDA represents lipid peroxidation and act as oxidative stress marker . It is observed that levels of MDA in diabetic cataract patients (Group II) were significantly increased as compared to controls (Group III)
MDA levels in senile cataract patients (Group I) were significantly increased as compared to controls (Group III) )
In diabetic cataract patients (Group II) the levels of MDA were significantly higher as compared to senile cataract patients (Group I)
It is observed that levels of reduced glutathione were significantly decreased in senile cataract (Group I) and diabetic cataract patients (Group II) as compared to controls statistically significant difference in reduced glutathione levels between senile and diabetic cataract were seen .

Table no 3 Showed Pearson’s coefficient Correlation (r) between AR and other parameters in study group I (senile cataract patients).It is observed that There was no correlation between ,AR and HbA1c AR and MDA and AR and GSH in Senile cataract patients.

Table no 4 :Showed Pearson’s coefficient Correlation (r) between AR and other parameters in study group II (Diabetic cataract patients) It is observed that There is no correlation between AR and mean age and between AR and duration of diabetes of diabetic cataract patients . ii) There is highly significant positive correlation between AR and HbA1c AR and MDA in diabetic cataract patients iii) There was a significant negative correlation between AR and GSH.

Discussion:
In this study, we attempted to evaluate the role of Aldose Reductase in cataractogenesis of diabetic patients. In present study it is found increased levels of HbA1C, AR, MDA and decreased levels of GSH in diabetic cataract patients as compared to senile cataract patients and as compared to controls.The mechanism of cataractogenesis in diabetes is associated with oxidative stress and osmotic stress. Eye is an organ that is continuously being exposed to oxidative stress throughout the life. Aging is a major risk factor for cataract and the prevalence is slightly higher in women considering all types of cataract. Increasing age is directly related with all types of cataracts11.
The mean age of diabetic cataract patients were significantly lower as compared to senile cataract patients (Table no 1).From the results it is observed that the process of cataractogenesis occur at early an age in diabetic patients as compared to non diabetic senile cataract patients. Our results are supported by the findings of studies of Deepa K et al 12 and Anjuman Gul et al 13.
Complications in diabetes depending on duration of diabetes and glycemic control HbA1c ( glycated Hb) is a good indicator of glycemic control . Measurement HbA1c reflects glycemic control for last 4-6 weeks
In present study the levels of HbA1c were significantly increased in diabetic cataract patients as compared to senile cataract patients and as compared to controls (Table no 2). Increased levels of HbA1c in diabetic cataract patients indicated the poor glycemic control which might be responsible for early cataract formation in diabetic patients as compared to non diabetic senile cataract patients .From this It is clear that an increased glycated haemoglobin level is associated with increased risk of cataract in patients with diabetes14,15. Our results are strongly supported by studies of various investigators M Lind et al 16, Anjuman Gul et al13, Bhavna et al 17.
Poor glycemic control leads to hyperglycemia and hyperglycemia induces polyol pathway. Aldose reductase is a key enzyme of this pathway.
We found high levels of AR in diabetic cataract patients as compared to senile cataract patients and as compared to controls (Table no 2). Hyperglycemia causes more and more glucose to enter in the polyol pathway which stimulates Aldose reductase (AR) that might facilitate the process of cataractogenesis.
A significant positive correlation between AR and HbA1c in diabetic cataract group (Table no 4) indicates that a significant increase in Aldose reductase activity in diabetic cataract patients due to hyperglycemia. Aldose Reductase (AR ) catalyzes the reduction of glucose to sorbitol through polyol pathway. The sorbitol pathway is stimulated in diabetes in those tissues that do not require insulin for cellular glucose uptake, such as the retina, kidney, peripheral nerves and blood vessels18. So there is free entry to glucose in lens and retina. AR reduces glucose to sorbitol. Which accumulates in lens and exerts osmotic stress leads to cataract formation. Our results strongly support the hypothesis that hyperglycemia induces/stimulates polyol pathway at the same time the diabetes reduces age of cataractogenesis.
In our study we found significant decreased levels of GSH in diabetic cataract group as compared to controls and as compared to senile cataract patients (Table no 2).
In addition to this a significant negative correlation was found in between AR and GSH (Table 4). Hyperglycemia is characterised by increase oxidative stress. Thus hyperglycemia is also responsible for increased flux of glucose in polyol pathway increasing the AR activity. In this Sorbitol is formed by AR at the expense of NADPH. Increased activity of AR decreases the concentration of GSH as there is less availability of NADPH for generation of GSH. This is explained by figure 1. Thus these results shows that depletion in GSH level might be responsible for increased oxidative stress. Our results are supported by the work of various investegators who reported the increase in oxidative stress in diabetic cataract by Oshi et al19 and G. Bhanuprakash Reddy et al 20.
Oxidative stress is characterized by an increase in the concentration of free radicals which can cause damage at different levels of cellular organization. Oxidative stress causes ocular membrane lipid peroxidation as well as lens protein oxidation MDA is a indicator of lipid peroxidation21.
In our study we have observed high levels of MDA in diabetic and senile cataract patients as compared to controls. An increase in MDA levels in diabetic cataract patients is more as compared to senile cataract patients may be due to poor glycemic control because a strong significant positive correlation was found in between MDA and HbA1c in diabetic cataract patients ( r = 0.88,p< 0.0001).These findings are supported by the work of Garg et al22 and Donma et al 23. They showed that increased levels of lipid peroxidation product (MDA) in diabetes was due to increased production of reactive oxygen species caused by hyperglycemic status, hyperinsulemia and hyperlipidemia, which are commonly associated with diabetes 24-26. This indicates that in diabetes due to hyperglycemia there is increase in lipid peroxidation which might be responsible for additional oxidative stress in diabetics .Based on the results of the AR in current study ,it is reasonable to hypothesize that AR activity above the threshold level in diabetics, might be predisposed to develop cataract. Secondly polyol pathway is responsible for generation of osmotic stress and oxidative stress in diabetics
Conclusions: From the result it is concluded that the extent of oxidative stress in diabetic cataract patients are more as compared to non diabetic senile cataract patients and AR is responsible for that generation of more oxidative stress. More oxidative stress may be the cause of early cataractogenesis in diabetic patients as compared to non diabetic senile cataract patients.
Further studies are required for therapeutic use of ARI (Aldose reductase inhibitors) to diabetic patients which may be beneficial in delaying the cataract formation in diabetics.
Acknowledgement:
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
DECLARATIONS:
Sources of Funding: No funding sources
Conflict of Interest: None declared
Ethical approval: The study was approved by the institutional ethics committee of B.J. Medical college Pune.

FIGURE 1| : Role of aldose reductase (AR) in hyperglycemia-induced oxidative stress. Excessive amount of glucose is shunted to the polyol pathway, where AR reduces glucose into sorbitol at the expense of NADPH. Since NADPH is essential for generation of GSH (intracellular antioxidant) from GSSG, the depletion of NADPH by the AR pathway may impair intracellular antioxidant defense .Sorbitol is then converted to fructose by SDH with the production of NADH ,potentially leading to increased ROS via NADH oxidase
References:
- Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes estimates for the year 2000 and projections for 2030. Diabetes Care 2004;27:1047-1053.
- World Health Organization. http://www.who.int/blindness/causes. Accessed7 September 2006.
- Kim SI, Kim SJ. Prevalence and risk factors for cataracts in persons with type 2 diabetes mellitus. Kor J Ophthalmol. 2006;20:201–4
- Morrision A D, R S Clements, S B Travis, F Oski, A I Winegrad. Glucose utilization by the polyol pathway in human erythrocytes. Biochem Biophys Res Commun 1970; 40:199–205.
- R G, P Barnett, J Aguayo, H M Cheng, L T J Chylack. Direct measurement of polyol pathway activity in the ocular lens. Diabetes 1984; 33:196–199.
- Jung HA, Isla MD, Kwon YS, Jin SE, son YK, Park JJ (2011). Extraction and identification of three major aldose Reductase inhibitors from Artemisia Montana food chem. Toxicology, 49; 376-384.
- Hayman S, Kinoshita J H. Isolation and properties of lens aldose reductase. J Biol Chem 1965; 240:877-82.
- Glen Hortin, Bruce Goldberger, Chromatography and Extraction. Textbook of clinical chemistry and molecular diagnostics by Carl A Burtis. Tietz; 5th edition; page 308.
- Buege J A and Aust S D. Microsomal lipid peroxidation. Methods in enzymology. Academic press, New York, 1978, 302 –316
- Beutler E, Duron O, Kelly B M. Improved method for the determination of blood glutathione. J Lab Clin Med 1963; 61(5):882-888.
- Shyamala M V, Joe Prasad Mathew, and Issac Thomas Dandona. Prevalance and potential risk factors of cataracts in certain regions of Ernakulam district, Kerala, India (2009); XVI: 1 and 2 S B Academic Review 2009:129-137.
- Deepa K, Manunatha Goud BK, Nandini M, AshaKamath and SudhirBhavanaNayal.Oxidative stress and calcium levels in senile and type 2 diabetes patients.IJPBS 2011;1(1):110-116.
- Anjuman Gul Memon, Ata ur Rahman, and Nessar Ahmed. Serum glycoproteins in diabetic and non diabetic patients with and without cataract.Pak J Opthalmol 2008; 24(3):122-126.
- BEKKlein, RKlein, and KELee. Diabetes ,cardiovascular disease, selected cardiovascular disease risk factors, and the 5-year incidence of age-related cataract and progression of lens opacities: The Beaver Dam Eye Study. American Journal of Ophthalmology 1998; 126(6):782–790.
- BE K Klein, R Klein, and S E Moss. Prevalence of cataracts in a population-based study of persons with diabetes mellitus. Ophthalmology 1985; 92(9):1191–1196.
- Marcus Lind, Anders Odén, Martin Fahlén, and BjörnEliasson. The true value of hba1c as a predictor of diabetic complications: simulations of HbA1c variables. Plos one2009; 4(2):4412.
- Manjunatha Goud BK, Bhavna Nayal, Sarsina Devi O, Sathisha T G, Shivashanker, Devaki R Sweta. Relation of calculated HbA1C with fasting plasma glucose and duration of diabetes. IJABPT 2011; 2(2):58-61.
- Stevens M J, I Obrosova, E L. Feldman D A Greene (2000). The sorbitol osmotic and sorbitol-redox hypothesis. In: D Le Roith, S I Taylor, J M. Olefsky (eds), Diabetes mellitus: a fundamental and clinical text, Lippincott Williams and Wilkins, Philadelphia, 972–983.
- N Oishi, S Morikubo, Y Takamura, et al. Correlation between adult diabetic cataracts and red blood cell aldose reductase levels. Investigative Ophthalmology and Visual Science 2006; 47(5):2061–2064.
- G Bhanuprakash Reddy, A Satyanarayana, N Balakrishna. Erythrocyte aldose reductase activity and sorbitol levels in diabetic retinopathy.MolVis2008;14:593–601.
- Dincer Y, Akcay T, Aldemir Z, Iikova H. Effect of OS on glutathione pathway in red blood cells from patients with insulin dependent diabetes mellitus. Met 2002; 51:1360-1362.
- Renu Garg, ManjuVerma, S P Mathur, P S Murthy. Blood lipid peroxidation products and antioxidants in senile cataract.Indian Journal of Clinical Biochemistry 1996; 11(2):182-186
- Donma O, Yorulmaz E, Pekel H, Suyugül N. Blood and lens lipid peroxidation and antioxidant status in normal individuals, senile and diabetic cataractous patients. Curr Eye Res 2002; 25(1):9-16.
- Evans J L, Gold Fine. Oxidative stress and stress activated signaling pathways a unifying hypothesis of type 2 DM. Endocrine review.2002; 23:599-622.
- Jacob Vaya, Michael Aviram. Nutritional antioxidant mechanism of action, analysis of activities and medical applications. Free Rad Biol Med 2000; 28:141-164.
- Gort A, Imlay J A. Balance between endogenous super oxide stress and antioxidant defenses. Journal Bacterial 1998; 180:1402-10
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





