IJCRR - 5(15), August, 2013
Pages: 87-94
Date of Publication: 17-Aug-2013
Print Article
Download XML Download PDF
GLOBAL HEALTH AND INFANT MORTALITY: APPLICATION OF VERBAL AUTOPSY TOOL TO CATEGORIZE INFANT DEATHS, ASCERTAIN THEIR CAUSES AND IDENTIFY THE GAPS IN HEALTH MANAGEMENT INFORMATION SYSTEM IN INDIA
Author: Vijay Kumar, B.S. Garg
Category: Healthcare
Abstract:Objective: To see the usefulness of verbal autopsy and in assessing the cause of deaths among infants and identify gaps in reporting system in 4 PHCs in India. Methodology: The study incorporated all the infant deaths, which occurred in a one-year period from 2nd Jan 2004 to 1st Jan 2005 in Yavatmal district in Maharashtra. This data was compared with the corresponding district data and the gaps in reporting were identified site-wise. Results: Medical certification of cause of death was done in only 12% of deaths. Under reporting was more than 50% in 2 PHCs and the IMR was found to be 59 per 1000 live births in contrast to 38 per 1000, given by the district authorities. Prematurity and LBW contributed for the 47% deaths during the early neonatal period. In post neonatal period mostly infectious causes like ARI contributed for 35% followed by CNS infections (12%). Majority (73%) of the 90 infant deaths were delivered at home and were attended by unskilled personnel (72%). Overall there were 63% deaths which occurred in the early neonatal period, 13% in late neonatal period and 23% in post neonatal period. Conclusions: Verbal autopsy can be used to give information for the health planners to prioritize health services based on the mortality pattern of an area and for collecting information for action at the local level.
Keywords: Infant mortality, low birth weight, Neonatal period, prematurity, verbal autopsy
Full Text:
Introduction
Global health is the health of populations in a global context and transcends the perspectives and concerns of individual nations. In global health, problems that transcend national borders or have a global political and economic impact are often emphasized. Thus, global health is about worldwide improvement of health, reduction of disparities, and protection against global threats that disregard national borders. Information on causes of death is extremely important for policy-making, planning, monitoring and evaluation of health programmes, as well as being necessary for field research, comparisons and epidemic awareness. In developing countries, where most deaths are neither attended by doctors nor medically certified, this crucial information is often incomplete and of poor quality. Since this situation is not likely to change in the near future, there is an urgent need to search for alternative methods of obtaining information on causes of deaths. This is particularly important for childhood deaths, which constitute a major portion of all deaths, and which many intervention programmes are currently attempting to reduce 1.
Specific targets for reducing the infant mortality rate (IMR) have been set by many governments and international organizations .The Millennium Development Goal is to reduce infant mortality rate to 35 per 1000 and under-five mortality to 45 per 1000 live births by 20152.The goal of National Health Policy-2002 is to reduce IMR to 30 per 1000 live births by 20103and the Tenth Plan goal is to reduce IMR to 45 per 1000 live births by 2007 and to 28 per 1000 live births by 2012.4 Since 1996, India’s IMR has stagnated at 72, which is far above the “Health For All” goal set by the government of India of an IMR of 60 per 1000 live births by the year 2000 5. India faces considerable challenge in the vital registration and cause of death (COD) reporting. Overall, about one in two of all births and deaths are registered in India. More reliable medically certified cause of death is available in only about one in 30 of all death
Materials and Methods
The verbal autopsy technique, which involves questioning the family of a dead infant about the features of the child’s final illness provides a means of obtaining information on the cause of death.
We set up a verbal autopsy system in the study areas of 4 health centers where the deaths occurring at the village level are identified by the Anganwadi workers (Dept. of women and child development). They will inform the infant deaths to the Auxiliary nurse midwife (Dept of health and family welfare) who conducts the verbal autopsy and then the deaths will be discussed in detail during the monthly meetings along with the Medical officer and the research investigator. The study was a prospective, observational study, combining both the qualitative and quantitative methods undertaken to find out the causes of infant deaths and to study the feasibility of infant mortality audit at the PHC level.
Duration and Study Site: The study was undertaken in four PHC areas of Dhanora, Waradh, Dahegaon and Mardi of Yavatmal District in 2005. The populations catered to by these PHCs were 22,449, 21,259, 28,530 and 25,494 respectively.
Study subjects
The study incorporated all the infant deaths, which occurred in a one-year period from 2nd Jan 2004 to 1st Jan 2005. This data was compared with the corresponding district data which was available in 2005 and the gaps in reporting were identified site-wise.
Eligibility criteria for inclusion were those which:
1. Qualified to be classified as infant death according to WHO ICD – 10 classifications
2. Deaths must have occurred within these 4 PHC areas.
3. All the deaths occurred in any health facility or en route to a health facility.
4. The deaths must have occurred between the above mentioned period.
Still births and deaths of infant outside the study area were excluded from the study
In the initial phase, consent from appropriate authorities, development of verbal autopsy questionnaire and piloting was done. Training of Anganwadi workers (AWs) for case identification and reporting and Training of ANMs in the art of conducting verbal autopsy was done in next phase. Finally the investigation of the Infant deaths using verbal autopsy was done ensuring quality, checking the Operational feasibility and data was analysed for report writing.
Consent of appropriate authorities
Permission was obtained well in advance prior to the beginning of the study from the appropriate district authorities to train the ANMs at DTO (District Training Office) and to attend the monthly meetings at PHCs. Co-operation with the ICDS and District Health System was ensured. Individual informed consent was taken from the respondents prior to interview.
Development of verbal autopsy questionnaire
Suitable verbal autopsy questionnaire was developed for the Auxiliary Nurse Midwife and LHV (Lady Health Visitor) with the help of standard verbal autopsy by WHO (WHO 1996), the Verbal Autopsy Method and Criteria developed by SEARCH (Hill 1992), Gadchiroli, the Verbal Autopsy Questionnaire used in the SRS (Hill 1999) and the verbal autopsy from the Primary Health Care Management Advancement Programme (PHC MAP) published by Aga Khan Foundation
RESULTS
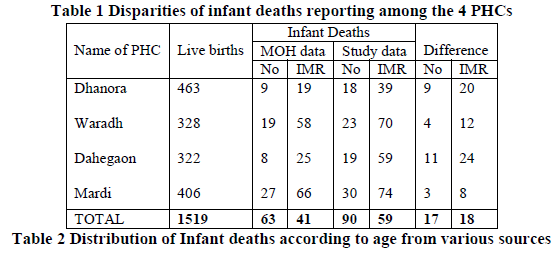
It was observed that from four health centers in the district, there was underreporting of 17 infant deaths during the year 2003-04. Among the 4 health centers it was found that the under reporting was more than 50% in Dhanora and Dahegaon. The reported IMR for these PHCs are 19 and 25 per 1000 live births respectively but it was found to be 39 and 59 per 1000 live births from the study there by leading to different IMR values from various sources as documented in Table 1.
Out of the total of 90 deaths, 59 (65.6%) were males while 31 (34.4%) were females.
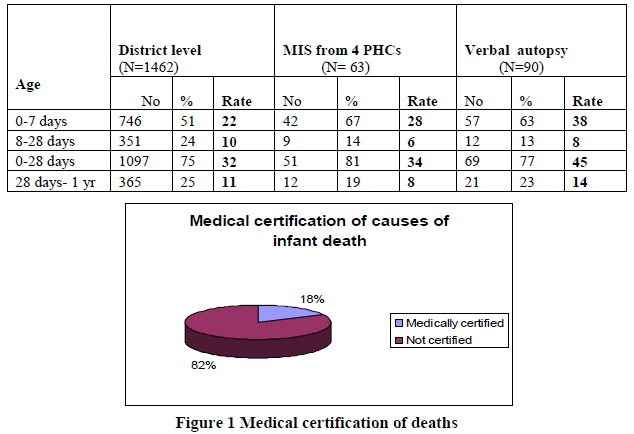
More than three-fourths of the infant deaths 74, (82.2%) were not medically certified
As shown in Figure 1. Out of the total 90 deaths investigated, where age at death was recorded, 57 (63.3%) were early neonatal deaths (0-7 days), 12 (13.3%) were late neonatal deaths (8-28 days) and 21 (23.3%) deaths occurred in the post neonatal period as shown in Table 2
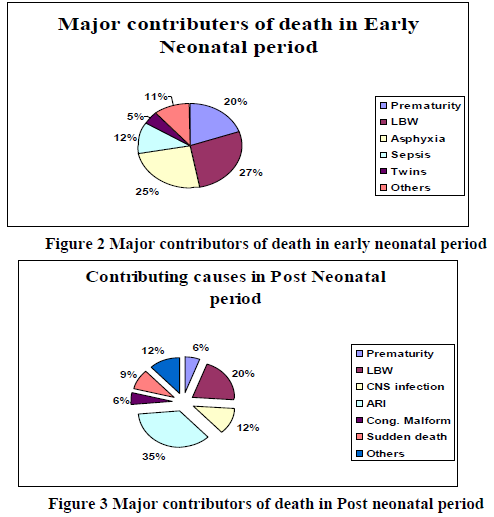
Among the total infant deaths investigated, in 66 (73.3%) cases delivery took place at home. In 23 (25.6%) cases, deliveries were institutional. In 1 (1.1%) case delivery took place during transport. Among the 90 infant deaths, 57 occurred in the early neonatal period and nearly half of the deaths i.e. 47% were contributed by both Prematurity and LBW followed by Asphyxia with 25%which shows the lack of skilled person during delivery as shown in Figure 2.
In contrast to the early neonatal period, in post neonatal period the majority of deaths were contributed mainly by the infectious causes especially acute respiratory infections with 35% followed by CNS infections (12%) as shown in Fig 3. LBW contributes to another 20% of the deaths that occurred in post natal period. It is seen that the deaths due to LBW and Prematurity contributed to 75% of all deaths in the study, whereas it was only around 49% as per the district data. Even though asphyxia contributed to 34%, of the cases, it was under reported as only 10% by management information system of health system.
Discussion
Infant mortality rate (IMR) is considered as one of the most sensitive indicators of health status and development of a community5. Each year, a total of 25 million infants are born in India and at the present neonatal mortality rate of 45 per 1000 live-births. 6 The objective of RCH – II Programme and the Tenth Plan is to decrease the prevailing IMR to 45/1000 by 2007 and 28/1000 live births by 20127.
The choice of Respondent is crucial for the accuracy of information. In the LSHTM workshop8, it was suggested that the interviewer should ask which members from the household were present at the time of death, were close to the deceased and are available for the interview. In the present study, out of the 90 infant deaths investigated, in the majority of deaths (66, 73.3%) the mother was the respondent while the father was the respondent in 18 (20.0%) deaths. The same is also supported by the findings of a previous study by Kalter et al, 1990 9 involving verbal autopsy. Though their methodology was quite different, Garrene and Fontaine, 1990 10 also found that mothers could provide accurate diagnostic information upto one year after the death of the child. In a review of 35 studies, which had used verbal autopsy for assigning causes of death, Chandramohan et al,1994 11 concluded that mothers are the principal respondents for childhood deaths.
In case of the 57 (63.3%) early neonatal deaths, 41 (72%) were males and 16 (28.1%) were females. Among 21 (23.3%) post neonatal deaths, 12 (57.1%) deaths were males while 9 (42.9%) were females. But when the total mortality rate is split into neonatal and post neonatal deaths, neonatal death rate is higher for males than for females while post neonatal death rate is higher for female infants than male infants12. The reverse findings in the study area could be attributed to the fact that gender bias is not yet as severe a problem as in the other parts of the country as depicted by the relatively better sex ratio of Maharashtra State (933 females per 1000 males)13.
Out of the 90 deaths investigated, more than half of the infant deaths (69, 76.7%) occurred at home. This is consistent with the findings of previous studies in rural areas which have demonstrated the unwillingness of parents to move ill infants from home because of traditional beliefs and practical difficulties (14-16) due to which most of the neonatal deaths occur at home.
Out of the 90 deaths investigated, more than three-fourths of the infant deaths (74, 82.2%) were not medically certified. This is consistent with the reported low levels of medical certification in the country.(17)The low levels of medical certification along with the low registration of childhood deaths in Maharashtra (28.2% in age group 0 – 4 years) and other states in India (18) results in the total lack of good quality data on infant deaths.
The encouraging aspect of the study was the identification of Low Birth Weight (LBW) and Neonatal Sepsis as important causes of neonatal and infant deaths. LBW was identified as a cause of death in 47.77% of infant deaths and 52.17% of neonatal deaths. This is in concordance with the high incidence of low birth weight reported in developing countries like India (26% of all live births).(22)
Neonatal sepsis was identified as a cause of death in 26.08% of neonatal deaths. This was consistent with the findings from various studies in India, which have shown that Neonatal sepsis is responsible for 20-27.5% of neonatal deaths.(23-25)The algorithm used in the present study was adopted from the verbal autopsy questionnaire used at SEARCH, Gadchiroli (26)
In the light of the above, it is clear that verbal autopsy conducted by ANMs can serve as a viable alternative to improve the infant mortality data. A study in Chandigarh (19) trained field assistants (PHC worker equivalent) with high school education to investigate infant deaths using verbal autopsy technique. In the study by Kalter et al. 1990,(20)mothers were interviewed by professional interviewers who were Filipino women with undergraduate college degrees. For studies involved in verbal autopsies of adult deaths, workers with higher levels of education were used. Chandramohan et al. 1998(21) utilized interviewers with at least 12 years of formal education. In the present study, the ANMs conducted the verbal autopsy and also assigned the causes of death, which were later reviewed by the PHC Medical Officer.
RECOMMENDATIONS
- Health Infrastructure and Medicines: To provide necessary equipment at the health centers like the essential medicines, equipment, vaccines, resuscitation kits, delivery kits etc to promote safe deliveries and prevent the asphyxial deaths.
- Human resources: Most of the sub centers and primary health centers are over burdened with work and they are understaffed. Good perinatal care will be achieved only if these centers are staffed optimally.
- Capacity building: Capacity building of staff members at the primary and secondary referral levels by providing skills and knowledge regarding the risk concept and appropriate technologies to promote methodology of IMNCI.
- Community Participation: To organize village referral teams with the involvement of community members, to establish community funds to pay for emergency referrals and transport that could be made available in an emergency.
- Leadership and Strengthening of Referral Services: Regular supervisory visits of the referral level staff members will support the TBAs, ANMs and mothers in caring for the newborns.
- Intersectoral Collaboration: Collaboration between sectors like Health, Women and Child Development is essential for complete reporting of infant deaths.
- Health Education: Provide health education to families, monitor the neonates for high risk or sicknesses and improve the health seeking behaviour, and increase utilization of health facilities
CONCLUSIONS
It was seen that the verbal autopsy can be used not only to give information for the health planners to prioritize health services based on the mortality pattern of an area but also the health workers can get a feedback of the information that they have collected. So VA can be used for collecting information for action at the local level.
The results suggest that there should be a shift in child survival programmes to give greater emphasis to maternal and neonatal health, in particular to safe delivery and cord care. In conclusion, the use of the verbal autopsy tool by health workers to find out the cause of death is feasible. It can also provide information for local action by health authorities to reduce the infant mortality rate, according to area-specific causes of death.
ACKNOWLEDGEMENTS
The Researcher is grateful to the Chief Executive Officer of Yavatmal district, PHC staff of Dhanora, Waradh, Dahegaon and Mardi centers in particular the ANMs for taking part in the study so graciously and thanks all the participants in this study. Authors acknowledge the great help received from the scholars whose articles cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. Authors are grateful to IJCRR editorial board members and IJCRR team of reviewers who have helped to bring quality to this manuscript.
Conflict of interest: The Authors declare that there is no conflict of interest
Source of Funding: This research study was supported by Department of Community Medicine, Mahatma Gandhi Institute of Medical Sciences.
Ethical clearance: The study got ethical clearance from the College Ethical Board and all the participants were included only after their consent to participate in this research as mentioned in methodology section.
References:
- Bang A.T, Bang R.A and the SEARCH team, Diagnosis of causes of childhood deaths in developing countries by verbal autopsy: suggested criteria. Bulletin of WHO 70(4) : 499-507 (1992)
- Millennium Development Goals and the UNDP role. UNDP Fast Facts. (www.undp.org). 2000.
- National Health Policy 2002. Ministry of Health and Family Welfare. Government of India, New Delhi.
- Tenth five Year Plan, (2002-07) Planning Commission, Government of India,Vol.1, Chapter 1,page 6.
- Health for All by the year 2000 AD, New Delhi. Report of Working Group of India, Ministry of Health and Family Welfare, India, 1981.
- Jha. P: Reliable Mortality Data : A powerful tool for public health; The National Medical Journal of India Vol 14; No.3 (2001)
- Annual Report – Survey of Causes of Death (Rural). New Delhi: Vital Statistics Division, Office of the Registrar General of India, Ministry of Home Affairs, 1992.
- LSHTM. Verbal Autopsy Workshop; verbal autopsy tools for adult deaths. Workshop report. London: London School of Hygiene and Tropical Medicine, 1993.
- Kalter HD, Gray RH, Black RE,et al. Validation of postmortem interviews to ascertain selected causes of deaths in children. International Journal of Epidemiology 1990: 19:380-386.
- Garenne M, Fontaine O. Assessing probable causes of death using standardized questionnaire: A study in rural Senegal. In: Palloni A,ed. Measurement and Analysis of Mortality. Oxford: Clarendon press, 1990.
- Chandramohan D, Maude G, Rodrignes L and Hayes R (1994) Verbal Autopsies for adult deaths : Issues in their development and validation. International Journal of Epidemiology (23);213-222.
- WHO. Implementation of the global Strategy for Health for All by the year 2000, Second Evaluation, Eighth Report on the World Health Situation, Vol.4, South East Asia Region: WHO,1993
- RGI. Sex Ratio of Maharastra, Census of India accessed on line at www.censusindia.net. New Delhi, 2001
- Bang AT, Bang RA, Morankar VP,et al. Pneumonia in neonate: can it be managed in the community? Arch Dis Child 1993; 68: 550-56.
- Sutrisna B, Reingold A, Kresno S, et al. Care-seeking for fatal illness in young children in Indramayu, West Java, Indonesia. Lancet 1993; 342: 887-89.
- Bhandari N, Bahl R, Bhatnagar V, Bahn MK. Treating sick young infants in urban slum setting. Lancet 1996; 347:1174-75.
- Kumar S. Status of Medical Certification of Cause of Death in India In: Counting the Dead in India in the 21st Century, Proceedings of the Second International Workshop on certification of Causes of Death, Goa, India, 9-12 February, 2000. Vol. Series B. Tata Institute of Fundamental Research, Mumbai.
- Mitra RG. Death Registration in India. In Counting the Dead in India in the 21st Century, Proceedings of the Second International Workshop on certification of Causes of Death, Goa, India, 9-12 February, 2000. Vol. Series B. Tata Institute of Fundamental Research, Mumbai
- Datta N, Mand. M and Kumar V; Validation of causes of infant deaths in the community by verbal autopsy. Indian Journal of Pediatrics 1998;55: 599-604
- Kalter HD, Gray RH, Black RE,et al. Validation of postmortem interviews to ascertain selected causes of deaths in children. International Journal of Epidemiology 1990: 19:380-386.
- Chandramohan D, Maude G, Rodrignes L and Hayes R (1994) Verbal Autopsies for adult deaths: Issues in their development and validation. International Journal of Epidemiology (23); 213-222.
- WHO. Bridging the gaps, The World Health Report, Report of the Director General Geneva: World Health Organization,1995
- Bang AT, Bang RA, Baitule SB, Reddy MH,et al. Effect of Home Based Neonatal Care and Management of Sepsis on Neonatal Mortality. Lancet 1999;354:1955-56
- Kaushik SL, Parmar VR, Grover N, Kaushik R. NMR: Relationship to Birth weight and gestational age. Indian J Pediatr 1998; 65: 429-433.
- Pratinidhi A, Shah U, A.S, et al. Risk approach strategy in neonatal care. Bulletin of the World Health Organization 1986; 64:291-97.
- Bang A.T, Bang R.A and the SEARCH team, Diagnosis of causes of childhood deaths in developing countries by verbal autopsy: suggested criteria. Bulletin of WHO 70(4) : 499-507 (1992).
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





