IJCRR - 5(15), August, 2013
Pages: 66-72
Date of Publication: 17-Aug-2013
Print Article
Download XML Download PDF
EVALUATION OF PRIMARY IMMUNIZATION COVERAGE AND REASONS FOR PARTIAL / NON IMMUNIZATION IN MAHARASHTRA
Author: Sanjay Wagh, Ashok Mehendale, Mohan Raut, Santoshi Wagh, Diwakar Sharma
Category: Healthcare
Abstract:Background: The complete immunization is cost effective method to prevent vaccine preventable diseases. In many areas complete immunization is not achieved due to various reasons. The partial or non immunization can be converted in to complete immunization if situation analyzed. Objective: 1) To find out the immunization coverage in 12- 23 months children. 2) Assess the factor associated with partial / non immunization 3) To find out various reasons for partial / non immunization. Methodology: A cross sectional study was conducted in field practicing area of Dept Community Medicine in Three PHC area of Wardha district Maharashtra by house to house survey. Study period: April 2009 to November 2010. A total 1199 children were included in the study Chi square test was applied for statistical analysis. Result: 84.90% children were fully immunized to primary vaccine. The immunization coverage for BCG (96.7%) Vaccine was highest and lower for Measles (84.9%). Most common reason for partial immunization was unaware about the schedule of vaccine (36.5%), out of station (17.7%) and child was ill (14.9%). Parent's education plays significant role in immunization status of children. IEC activities should be in community to avoid non immunization in children.
Keywords: immunization, partial immunization, various reasons.
Full Text:
INTRODUCTION
Protection through immunization against vaccine preventable diseases, disabilities and death is the right of every child. Vaccines remain one of the most cost-effective public health initiatives1. In India, immunization services are offered free of cost at government hospitals still the coverage remains low. According to the National Family Health Survey (NFHS-3), only 44% of 1to 2 years old children had received the basic immunization, which is much less than the desired goal of achieving 85% coverage2. However it is not an easy task to achieve. In a developing country like India, the sheer logistics of the numbers of the target population that stretches across geographically diverse regions make universal immunization of children a herculean task3. Because of increased accessibility of health care services in both urban and rural areas, an increase was expected in the utilization of the services; however, studies reveal low utilization of health care services 4. It is known that fully immunization status can only protect the children at maximum. Percentage of protection may be reduced in partially immunize child5.
Parents show various reasons for discontinuing or non immunizing their children. Success of immunization coverage depends upon clear understanding of reasons for partial immunization of a child. Hence the present study was planned with the following objectives.
OBJECTIVE
- To find out immunization status among the children in the age group 12-23 months
- To assess the factor associated with immunization
- To find out various reasons for partial immunization
METHOD
Study Design: The cross sectional descriptive study
Study area: Three PHC area of Wardha District (Mahrashtra) Namely Anji, Goul and Talegaon including 67 villages.
Study Population: Children in the age group of 12-24 months.
Study period: April 2009 - November 2010
Data collection technique and tools
Three PHC’s (Population 88131) were selected as it comes under field practice area of the Department of Community Medicine, MGIMS, and Sevagram Wardha district. List of children in the age group of 12-23 months was prepared by house to house visit, separately for each village. In all the families with a child in the age group of 12-23 months, a pre-tested and pre-designed questionnaire was administered to the mother of the child to find out if the child has been immunized with all the vaccines in the national immunization schedule. If she was not available at the time of survey; father, grandmother, grandfather or any care taker more than 18 years of age was asked to provide the information. The respondents were asked whether they had a vaccination card of the child. If the vaccination card was available in the family, particulars about each vaccine was noted. For vaccinations not recorded on the card, the respondent's report that the vaccination has or has not been given the vaccine was accepted. If a house was found locked, the investigator visited the household two more times.
However, if the house was found locked during all three visits, no further visits were paid to the household. For all children, who had not received the full course of the primary immunization, in-depth interview was conducted to find out the cause of non-immunization or partial immunization. The in-depth interview was based on a semi-structured format. The details about the missed dose of partially/ non immunized child was noted. A child was classified as fully immunized if he had received one dose of BCG, three doses of DPT and one dose of measles vaccine. Partially immunized any one of the dose or vaccine was dropped. Unimmunized child means who had not given any vaccine. BCG scar was looked for history of immunization.
Data entry and Analysis: The data for primary dose were entered and analyze in SPSS 16 -Version. P value was generated, p value <0.05 was taken as significant and >0.05 was taken as non significant.
RESULT
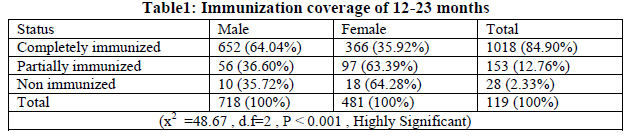
Table 1: A total no 1199 children in the age group of 12-24 months were included in the study. (84.90%) children’s were fully vaccinated against all six vaccine preventable diseases. When compared between gender, the proportion of fully immunize children was higher in male (64.04%) than in female (35.92%), however the difference was highly significant (p-value=<0.001) in male and female.
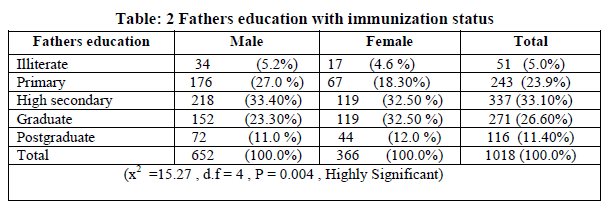
It is observed that immunization coverage was higher in male as compared to female in each group. A highly significant association is found between father’s literacy and immunization status of their children, suggesting the existence of gender discrimination. (p-value = 0.004). In general immunization status was proportionally better in children whose father was educated.
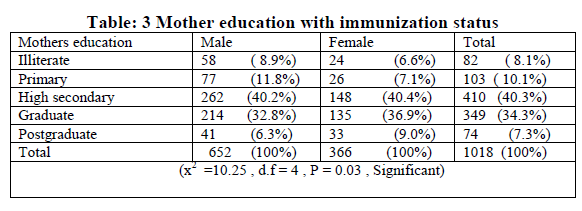
A significant association between mother’s literacy and immunization status of their children is observed (p-Value =0.03). It is also observed that immunization coverage was higher in male as compared to female in only illiterate and primary groups. Education status of mother directly impacts the immunization. When we compare father vs. mother education, father education group has 95.1% children immunized while in mother education group only 91.9% were immunised.
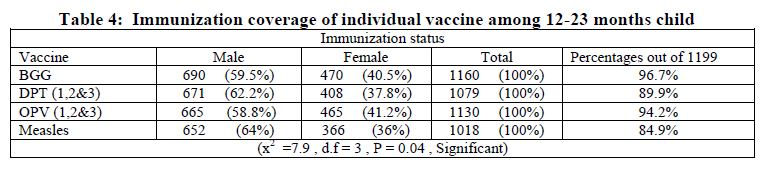
In Immunization coverage individual BCG coverage was highest 1160(96.7%) and lowest for measles (84.9%). It is also observed that immunization coverage was higher in male as compared to female in all vaccine cases this difference was found statistically significant, (P -value=<0.05).
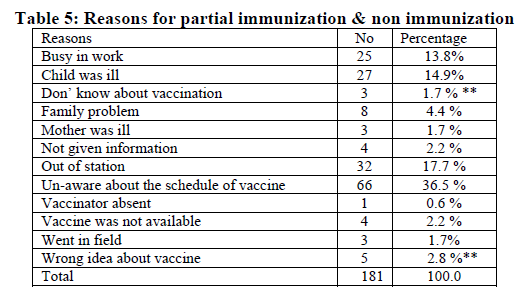
Note: ** denote reason for non immunization.
Unawareness of vaccine schedule was 66 (36.5%) the main reason for partial immunization followed by out of station 32(17.7%).
DISCUSSION
Among the method of prevention of communicable diseases, immunization is very effective and also cost effective method. The complete immunization gives full protection to children. The present study was conducted in three PHC areas to assess the immunization coverage and to find out various reasons for partial/ non immunization. In present study it was found that overall (84.98%) children were fully vaccinated against six vaccine preventable disease. These finding were comparable to that of Dalal6 in Department of pediatric in Goa Medical college (85%), Similarly Punith K7 et al urban area of Banglore city (84.09%), and Maj Joshi RM8 et al Military Station (84.2%).
A survey by Choudhary V et.al3 found that the fully immunization for male was more (68.69%) as compared to female (55.86%). In the present study we found that the immunization coverage was higher in males (64.04%) as compared to female (35.92%). We found much less coverage for female than in male this difference among may be due to gender inequality. However similar type of finding was also reported by study conducted by Khokar et.al11 male 153(59.68%) female 105(40.07%).
In the present we observed that 1160(96.7%), 1079(89.9%)1130 (94.02%)and 1018(84.9%) children were immunized against BCG, DPT3, OPV3and Measles in our study, similar rate was observed by Dalal A et.al6 pediatric ward department of Pediatric in Goa medical college i.e 94%, 96%, 95%, 88% BCG, DPT3, OPV3and Measles.
We found, out of 1160, 690(59.5%) males and 470 (40.5%) female was vaccinated for BCG however the study conducted by Prabar K12 et al in Darjling district of West Bengal reported almost same cover coverage for male and female (81.36%), (80.65%). So in the study it was observed that female vaccination coverage was contrast with the above study and this variation may be due to Geographic variation, gender inequity and survey technique.
In the present study among (84.98%) of fully immunized children 26.60% (Total 271; Male-152,,Female-119) belonged to father who were graduate however 33.10% (Total 337; Male-,218 Female-119), 23.9% (Total 243; Male-,176 Female-67), 5%(Total 51; Male-,34 Female-17), children belonged to father who was high secondary, primary and illiterate respectively. A highly significant association is noted between fathers literacy and immunization status of children (p-Value <0.0004) immunization status improved with fathers literacy.
Similarly for female 34.28% (Total 349; Male-, 214 Female-135) of fully immunize children belonged to mothers with education up to high school, while 40.75 %( Total 262; Male-,148 Female 45), 10.11%(Total 103; Male-,77 Female 26),7.3%( Total 82; Male-,58 Female 24)) children belonged to mother with education level up to primary school, and high school illiterate these finding shows that a significant association between mothers education the finding of the study is similar to study conducted by Inamdar1 et al. our study none of the graduate and post graduate mother had any unimmunized child. This is accordance to a study conducted at Goa6. Where none of graduate mother had any unimmunized child. The findings of low immunization coverage in female as compared to male is due to discrimination of against female as also stated in study done by Vinit Sharma13 and Anuragini Sharma13 they also stated that higher immunization rate in male because of they get more importance. The coverage rate were higher than female male children14 similar Sex bias was seen in the study done on immunization coverage in urban area of Utterpradesh by Nirupam S15, Chandra R, Shrivastav VK.
Earlier studies reported 7,9,10 reported partial immunization coverage ranging from (5.25% to 29.7%). The present study reported (12.76%) of partial immunization, these finding is comparable with the study conducted by Chopra9 et al in urban area of Merut (14.09%). Similarly non immunization percentages in previous studies reported range from (2.3% to 23.9%)6,16,3,2,17. During our study we found non immunization rate was (2.33%) similar finding was also reported (2.3%) by Dalal A6 et al in Goa.
In the present study unawareness about the schedule of vaccine was the most common cause of missed dose. Similar finding was also reported by Khokhar in urban community of Delhi11, unaware of immunization schedule has been mention the main reason for Partial immunization and non immunization.
Out of station was the another main reason for partial In Maharashtra most of the mothers travel frequently husbands home to fathers home during post natal period this finding suggest social behavior as the major obstacle for incomplete or non immunization. Supporting this finding, a study conducted in Anand District Gujrat18 has also mention by children gone another place as third most important reason.
Child was ill was the third reason for partial immunization in the present study however the study institute of Childs health in madras mention the minor illness was 4th important reasons for partial/non immunization14 . The parents must be educated through Mass media and by group individual contact of parents community to have immunize child when it is due, even if the child having minor illness.
CONCLUSION
Immunization coverage has been increase substantially in general in recent year, a sizable proportion of children are not being immunized the study identified association parents education, gender discrimination along with an aware of the parent was the main reason for partial / non immunization. Gender discrimination was responsible for further lowering of immunization coverage in girl. Present day vaccination programme framed by government of India emphasizes six vaccine preventable diseases during 1st year of life. Community need to educate and made aware about the fact. This study provides us important insight in existing level of awareness among the people. Define gender bias exists.
RECOMMENDATION
- The health education should be emphasized to enhance respondents knowledge about complete immunization.
- Immunization programme has to be incorporated in school health programme.
- Special activity should planned to immunize missed children should make aware about the fact and schedule.
- ACKNOWLEDGEMENT We acknowledge the great help received from the scholars whose articles cited and included in references of this manuscript. We are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. We are also thankful to the all auto drivers participated in the study, for their co-operation.
-
Conflict of interest: Authors had not declared any conflict of interest.
Source of funding: None
References:
- Inamdar M, Piparsania S, Inamdar S, Singh K. Exploring the causes of low immunization status in school going children. Journal of Health and Allied Sciences. 2011;10(4):1-4.
- Vikaram A, Amarjir S, Vijaylakshmi ,S Coverage and quality of immunization services in rural Chandigarh. Indian Pediatrics. 2012;49:565-567.
- Varsha C, Rajiv K, Arawal VK, Joshi SH, Sharma M, Evaluvation of Primary immunization coverage in urban area of bareilly city using cluster sampling technique. JIRM.2010;1(4): 10-15.
- Sharma R, Desai VK, Kavishavr A. Assessment of immunization status in slums of surat by 15 cluster multi indicator cluster technique. Indian J community Med. 2009;32(2):152-155.
- Govindarajan PK, Senthilmugan TK. Study on immunization coverage in urban population in Tamilnadu. Nat.J.Res.Com Med.2012;1(4):220-222.
- Dalal A, Silveira MP. Immunization status of children in Goa. Indian Pediatrics. 2005;42:401-402.
- Punith K, Lalitha K,Suman G,Pradeep BS, Jaynath Kumar K. Indian J community Med. 2008;33(3) 151-155.
- Maj RM Joshi, Lt Col (Mrs) Bala. Immunization Coverage at a Military Station. MJAFI,2003; 59(3):223-225.
- Chopra H, Singh AK, JV Bhatnagar,M Garg,SK Bajpai SK. Status of routine immunization in urban are of Merrut. Indian J community Med. 2007;19(1):91-92.
- Chturvedi M, Nandan D, Gupta SC. Rapid assessment of immunization practice in Agra district. Indian Journalof Public Health. 2007;51(2):132-134.
- Khokhar A, Chitkara A, Talwar R, Sachdev TR, Rasania SK. A study of reasons for partial immunization and non immunization among children aged 12-23 months from an urban community of delhi . Indian J.Prev.Soc.Med.2005;36(4):84-86.
- Prabar KM, Kousik C, Debasis D, Debidas G. Child Immunization Coverage o f Some Rural Belt in Relation to Socioeconomic Factors of Jalpaiguri and Darjling district of west Bengal. J Life Sci 2009;1(2):91-95.
- Sharma V, Sharma A. is female child being neglected? Immunization in India. 2010
- Yadav S, Mangal S, Padhiyar N, Mehata JP, Yadav BS. Evaluvation of immunization Coverage In Urban Slums in Jamnagar. Indian J community Med. 2006;31(4) 300-3001
- Nirupam S, Chandra R, Shrivastav VK Sex bias in immunization coverage in urban area of UP. Indian Pediar.1910;27(4):388-4.
- Bhola N, Singh JV, Shally A, Vidya B, Vishwajeet K, Singh SK. KAP Study on Immunization of Children in a City of North India. Journal of Health and Allied Sciences.2008;7(1):1-6.
- Devivanayagam N, Nedunchelian K, Ashok TP, Mala N. Reasons for Partial /non Immunization With Oral Polio /Triple Antegen Umong Children Under Five Year.Pediatrics.1992;29:1347-1351.
- Tushar P, Niraj P. Why infant Miss Vaccination During Routine Immunization Session? Study in a Rural Area of Anand District, Gujrat. Indian Journal of Public Health.2011; 55(4):321-32.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





