IJCRR - 5(15), August, 2013
Pages: 55-61
Date of Publication: 17-Aug-2013
Print Article
Download XML Download PDF
LOW PREVALENCE OF DENTAL CARIES IN CHILDREN WITH PERINATAL HIV INFECTION
Author: Sahana Srinath, Srinath S.K., Vishwanath S.K., Ritu Singh, Pravesh Bharadwaj
Category: Healthcare
Abstract:Objective: The objective is to assess the prevalence of caries in children with perinatal HIV infection. Methods: Oral examination was performed on Children aged 2-12 years with perinatal HIV infection who stayed at 'Calvary Chapel home of hope for special children' in Bangalore, to assess dmft/DMFT. Results: Prevalence of tooth decay in primary teeth (dmft) for the age group 2-6 years was 57.15%, for age group 7-12 years was 20.0%. Prevalence of tooth decay in permanent teeth (DMFT), for the age group 7-8 years was 16.60%, for age group 10-12 years was 21.42%. Of the 27 children examined 59.25% were caries free, in which 40.0% were male children and 70.58% were female children. Conclusions: Based on these results we can conclude that oral hygiene can be maintained with a favorable dental behavior
Keywords: Caries, Diet, Dental Health
Full Text:
INTRODUCTION
In worldwide it is estimated that there are 2.3 million HIV positive children from 0 to 14 years infected by mothers (1). In children, the quality of life related to health should be considered differently from adults (2). The high prevalence of HIV infection reinforces the need of dentists and his staff to update the prevention and treatment of diseases and the promotion and maintenance oral health of individuals with HIV/ AIDS (2).
Prior to 1992, informationabout dental caries in HIV-infected children was verylimited (3). Of the published articles on the oral manifestationsof AIDS, virtually all addressed this issue only in anadult population. In one of these studies, HIV-infected adultshad a lower prevalence of dental caries than a comparison groupof healthy adults from the same region of Zaire (4).Another adultstudy found that there was an association between dental cariesand Capnocytophagakeratitis (5). A Russian study found a highincidence of dental caries in symptom free HIV-infectedadults (6). It was not until the late 1980s that investigators startedto turn attention to the oral manifestations of HIV-infectedchildren, but none of those earlier writings reported on thedisease of dental caries (7-9). Between 1992 and 1996 there werethree published cross-sectional studies of dental caries in theprimary teeth of HIV-infected children (10-12).These studiesshowed that there was a higher prevalence of dental caries (including ECC) in the primary dentition of HIV-infectedchildren as compared to healthy children. However, in a 1996case control study of caries prevalence in a group of childrenaged 1.5 to 12 years, Teles, G et al. reported a lower dmft for HIV-infected children as compared tohealthy children, as well as a higher DMFT (13). Vieira, et al., reported that HIV-infectedchildren (aged 2-12 years), who were more immunologicallyaffected (CD4:CD8 < 0.5 ratio) showed a greater DMFT/dmfindex than HIV-infected children who were immunocompetent (14).
Standard antibody testing is now available to determine a person’s HIV status at an early age. However because of the expense of the complex technology, health workers in developing countries – where 95% of the world’s paediatric AIDS cases are found – must rely on early clinical manifestations of HIV infection (15). Moreover, the use of disease markers prevalent in adult HIV infection is not necessarily effective in the paediatric AIDS population. CD4 lymphocytes, for example, where HIV primarily resides and multiplies, decline with the progression of HIV disease in infected adults; in children, however, a CD4 count alone is not as reliable a marker of progressive disease because children tend to have higher and less consistent CD4 levels than do adults (16,17).
In the light of the above factors the aim of this study was to assess the prevalence of dental caries in children with perinatal HIV infection.
HYPOTHESIS
Null Hypothesis (H0): The prevalence of dental caries in children with perinatal HIV infection is not different from that of normal children residing in the same region.
Alternative Hypothesis (H1): The prevalence of dental caries in children with perinatal HIV infection is higher than that of normal children residing in the same region.
MATERIALS AND METHODS
Source of data
Children aged 2-12 years staying at Calvary Chapel home of hope for special children in Bangalore, with perinatal HIV infection were chosen as subjects.
Method of data collection
27 subjects with perinatal HIV infection fulfilled the criteria and were included in the study. The participation of the subjects in the study was voluntary, and a written informed consent was obtained at the beginning of the study.
Inclusion criteria
1. Children with perinatal HIV infection
2. Children stayed at ‘Calvary Chapel home of hope for special children’
3. Age group: 2- 12 years
Exclusion criteria
1. Children with any oral lesions
2. Children on medications other than anti viral therapy
3. Chronic inflammatory diseases like Rheumatoid arthritis which require Medication
TRAINING AND CALIBRATION
The investigator was trained in the department of Pediatric dentistry, Government Dental College and Research Institute Bangalore, on 10 subjects. Calibration was done on 10 subjects, who were examined twice using diagnostic criteria on the same day with a time interval of one hour between the two examinations, and then the results were compared to diagnostic variability. Agreement for assessment was 90 percent.
EXAMINATION
The examination procedure was carried out at the calvary chapel home of hope for special children under natural light by single investigator. The children were made to sit on a cement bench. The oral examination was performed according to World Health Organization guidelines for oral health surveys. The diagnosis of developmental enamel defects was done according to the modified developmental defects of enamel index.
Examination was carried out using 27 mouth mirrors and 27 periodontal probes. Examination of children was undertaken to determine caries prevalence using dmft/DMFT, and developmental enamel defects. The examiner started with the upper left central incisor and continued distally through the second molar in the same quadrant. The same sequence was followed for the upper right, lower left, and lower right quadrants. Tooth surfaces were examined in the following order: lingual, labial, mesial, and distal for anterior teeth, and occlusal, lingual, buccal, mesial, and distal for posterior teeth. (Image 1)
Guardians were interviewed to obtain information on their children’s dental health behaviors such as tooth-brushing, diet, fluoride; oral medication and dental attendance were explored.
Data collected was used to estimate the mean number of teeth, the number of teeth with carious lesions, number of missing/extracted teeth and number of teeth with restorations. Caries was defined by presence of decayed or filled teeth, and was categorized as present or absent.
As the subjects stayed in the special home for children with HIV infection, a suitable control group was not found. Hence the prevalence of dental caries (dmft and DMFT) in children with perinatal HIV infection was compared with the prevalence of dental caries in normal children residing in the same city, which was found in a large study conducted in Bangalore city (18).
RESULTS
The study population was composed of 27 children, there were 62% (n=17) female children and 38% (n=10) male children. 27 children ranged in age from two to twelve (2-12) years, with a mean age of 8.407 years. Developmental enamel defects nor the discrepancies in the average number of teeth for their age were found. All the twenty seven children brushed their teeth twice daily with a tooth brush and tooth paste to clean their teeth.
CARIES
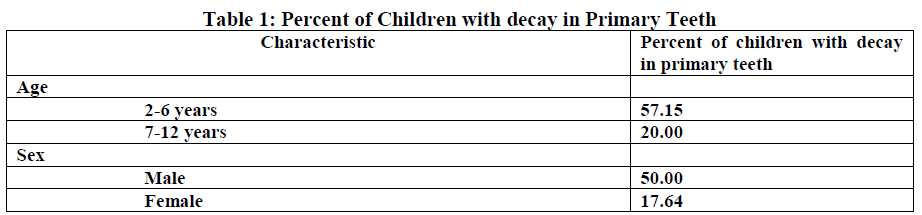
Prevalence of tooth decay in primary teeth (dmft) for the age group 2-6 years was 57.15%, for age group 7-12 years was 20.0%. 50.0% of male children were free of decay in the primary teeth, however 82.36% of female children were free of decay in the primary teeth (Table 1).
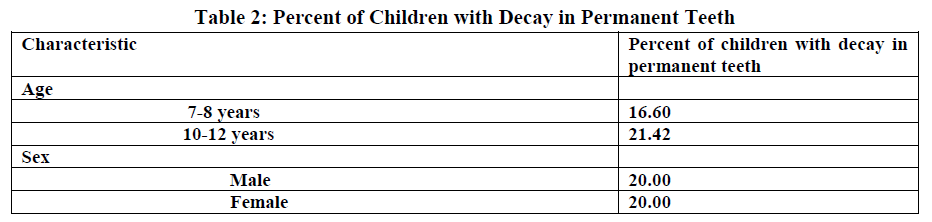
Prevalence of tooth decay in permanent teeth (DMFT), for the age group 7-8 years was 16.60%, for age group 10-12 years was 21.42%. 20.0% of male children had caries in their permanent teeth, and 20.0% of female children had caries in their permanent teeth (Table 2).
Of the 27 children examined 59.25% were caries free, in which 40.0% were male children and 70.58% were female children (Table.3).

The dmft found in these children was 0.55 with a standard deviation of 1.088 and the DMFT was 0.733 with a standard deviation of 1.10. The dmft found in children with perinatal HIV infection was low and was marginally significant (p=0.072, p > 0.05 however p < 0.10,) compared with that of normal children. However no significant differences were found in DMFT of these children when compared with that of normal children (p= 0.238) (Table.4).

DISCUSSION
Oral health care is an important component of all round care for people withHIV infection (19).The lack of healthy, functioning dentition can adversely affect the quality of life, complicate the management of medical conditions, and create or exacerbate nutritional and psychosocial problems (20).Some anti-retroviral drugs are sucrose based in the form of a syrup or suspension, such as Zidovudine, and others may lead to decreased salivation, which makes them potentially cariogenic (21).
In South Africa an oral examination was performed on 87 HIV positive children ranged between 3.2 and 7yrs, who were not receiving antiretroviral treatment. Rampant caries early in childhood was found in 19 (21.8%) children, with 5 children suffering severe pain from multiple carious teeth (22).The study in Romanian population consisted of 173 children at age range 6 to 12 years noted severe dental caries in the majority of children (dmfs/dmft 16.9/3.7 and DMFS/DMFT 8.1/3.1) (23).
According to Howell et al (24). The prevalence of caries in HIV children was very high, especially with deciduous dentition. Tofsky et al.(25) found a mean dmft average of 8.3 for children with HIV, while for children not infected with HIV this average was 3.1 teeth, which showed, according to the authors, the need of guidance and treatment for those infected patients. A comparative study of the prevalence of caries, by Souza et al (26).In HIV infected children and children without evidence of immunosuppression, showed statistically significant difference between the average mean dmft (5.29; 2.59) and DMFT (2.36; 0.74) of the two groups, respectively. Other recent studies showed that the high prevalence of caries in infected children seems to be greater in those that are in advanced stage of disease and with more severe degree of immunosuppression (27).
Poorandokht et al., found that 54 children of the 100 children examined had rampant caries and rampant caries was the most common oral manifestations of AIDS in those children (54%) sfollowed by periodontal disease (44%), further authors suggested that Rampant caries and severe periodontal diseases (mean CD4 count, 523±297) might have caused tooth loss and dentures use in some patients with severe immunosuppression, resulting in not being categorized as rampant caries (28).
Beena JP et al, found that the primary dentition group had a mean deft of 5.07 ± 5.29 and a caries prevalence of 58.62%; in the mixed dentition group the mean deft was 3.81 ± 3.41 and the mean DMFT was 1.40 ± 2.03 with caries prevalence of 86.20%. In the permanent dentition group the mean DMFT was 3.00 ± 2.37 with a caries prevalence of 76.47% (29).
It was however observed that the prevalence of dental caries recorded in the present study was lower than those previously reported. Dental caries prevalence in these HIV positive children although lower than that seen in other studies was however did not differ significantly when compared to reports of healthy children residing in the same city.
|
Although the exact reason for the low levels of dental caries prevalence recorded in this study was not apparent, it may be attributable to the general high level of oral health awareness and the diet they consumed which completely eliminated the added sugars, which leads to good oral health and restorative care. (Image 2)
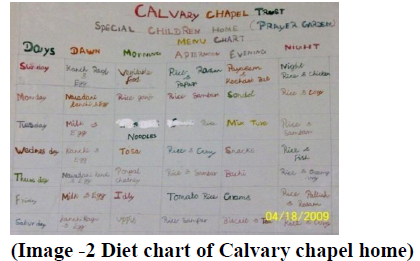
(Image -2 Diet chart of Calvary chapel home)
CONCLUSIONS
Children with perinatal HIV infection who stayed at Calvary chapel home of hope had a favorable dental behavior and the caries experience was low.
IMPORTANCE OF THIS PAPER
Survival rates for children born with HIV who receive antiretroviral therapy are more than double those for children who do not. However Some anti-retroviral drugs are sucrose based in the form of a syrup or suspension, such as Zidovudine, and others may lead to decreased salivation, which makes them potentially cariogenic.
Many recent studies have demonstrated high caries prevalence rates in these children; however in the present study we found a group of children taking ART with low prevalence of caries.
|
References:
- United Nations Programme on HIV/AIDS (UNAIDS). AIDS epidemic update. Special report on HIV/AIDS. Geneva: Joint United Nations Programme on HIV/AIDS (UNAIDS), World Health Organization (WHO); 2006. [cited 2009 Aug 31]. Available from: http://data.unaids.org/pub/EpiReport/2006/2006_EpiUpdate_en.pdf
- Sílvia Helena de Carvalho Sales-Peres, Marta Artemisa Abel Mapengo, Patrícia Garcia de Moura-Grec, Juliane Avansine Marsicano, André de Carvalho Sales-Peres, Arsenio Sales- Peres. Oral manifestations in HIV+ children in Mozambique. Ciência and Saúde Coletiva . 2012;17(1):55-60
- Moyer I, Kobayashi R, Cannon M, Simon J, Cooley R, Rich K: Dental treatment of children with severe combined immunodeficiency. Pediatr Dent. 1983;5:79-82.
- Murray P, Grassi M, Winkler J: The Microbiology of HIVassociated periodontal lesions. J Clin Periodont. 1992;16:636-42.
- Ticho B, Urban R, Safran M, Saggau D: Capnocytophaga keratitis associated with poor dentition and human immunodificiency virus infection. Am J Ophthalm. 1990;109:352- 53.
- Kharchenko OI, Pokrovskii VV: The state of the oral cavity in persons infected with the human immunodeficiency virus. Stomatologiia. 1989;68(5):25-8.
- Leggott P, Robertson P, Greenspan D, Wara D, Greenspan J: Oral manifestations of primary and acquired immunodeficiency disease in children. Pediatr Dent. 1987;9:98-104.
- Tucker B, Schaeffer D, Berson R: A combination of HIV antibody and HIV viral findings in blood and saliva of HIV antibody-positive juvenile hemophiliacs. Pediatr Dent. 1988;10:283-86.
- Falloon J, Eddy J, Wiener L, Pizzo P: Human immunodeficiency virus infection in children. J Pediatr 1989;114:1-23.
- Howell R, Jandinski J, Palumbo P, Shey Z, Houpt M: Dental caries in HIV-infected children. Pediatr Dent. 1992;14:370-71.
- Valdez I, Pizzo P, Atkinson J: Oral health of pediatric AIDS patients: A hospital-based study. J Dent for Children.1994; 61: 114-18.
- Madigan A, Murray P, Houpt M, Catalanotto F, Feuerman M: Caries experience and cariogenic markers in HIV-positive children and their siblings. Pediatr Dent.1996;18:129-36.
- Teles G, Perez M, Souza I, Vianna R: Clinical aspects of human immunodeficiency virus (HIV) infected children. J DentRes.1996;75:316 (abstract #2386).
- Viera AR, Ribeiro IP, Modesto A, Castro GF, Vianna R: Gingival status Of HIV+ children and the correlation with caries incidence and immunologic profile. Pediatr Dent 1998;20:3169-72.
- Falloon J, Eddy J, Wiener L, Pizzo P: Human immunodeficiency virus infection in children. J Pediatr.1989;114:1-23,
- Howell R, Jandinski J, Palumbo P, Shey Z, Houpt M: Dental caries in HIV- infected children. Pediatr Dent 1992;14:370-71.
- Valdez I, Pizzo P, Atkinson J: Oral health of pediatric AIDS patients: A hospital-based study. J Dent for Children.1994; 61:114-18.
- Pramila M, S. S. Hiremath. Oral health status of handicapped children attending special schools in Bangalore city. Int. J.of Cont. Dent 2011;2(1):55-581
- S. G. Damle, A. K. Jetpurwala, S. Saini, P. Gupta. Evaluation of Oral Health Status as an Indicator of Disease Progression in HIV Positive Children. Pesq Bras Odontoped Clin Integr, João Pessoa 2010;10(2):151-156
- Baccaglini L, Atkinson JC, Patton LL, Glick M, Ficarra G, Peterson DE. Management of Oral lesions in HIV-positive pati ents. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007; 103 Suppl:S50.e1-23.
- Charles Mugisha Rwenyonyia, Annet Kutesaa, Louis Muwazia, Isaac Okulloa, Arabat asangakia, Addy Kekitinwab. Oral Manifestations in HIV/AIDS Infected Children. Eur Jou of Dent 2011; 5:291-298
- Blignaut E. Oral health needs of HIV/AIDS orphans in Gauteng, South Africa. AIDS Care 2007; 19(4):532-538.
- Flaitz C, Wullbrandt B, Sexton J, Bourdon T, Hicks J. Prevalence of orodental findings in HIV infected Romanian children. Pediatr dent. 2001; 23(1): 44-50
- Howell RB, Jandinski J, Palumbo P, Shey Z, Houpt M. Dental caries in Hiv-infected children. Pediatr Dent 1992;14(6):370-371.
- Tofsky N, Schoen D, Jandinski J, et al. Dental caries in children with Aids. J Dent Res 1995; 74:191.
- Souza IPR, Teles GS, Castro GF, Guimarães L, Viana RBC, Peres M. Prevalence of dental caries in HIV-infected children. Rev Bras Odontol 1996; 53(1):49-51.
- Castro GF, Souza IP, Chianca TK, Hugo R. Evaluation of caries prevention program in HIV+ children. Braz Oral Res 1997; 15(2):91-97.
- Poorandokht Davoodi, Mina Hamian, Reza Nourbaksh, Fatemeh Ahmadi Motamayel.Oral Manifestations Related To CD4 Lymphocyte Count in HIV-Positive Patients. J. of Dent Research, Dental Clinics, Dental Prospects. 2010;4(4):115-119 Beena JP.Prevalence of dental caries and its correlation with the immunologic profile in HIV-Infected children on antiretroviral therapy.Eur J Paediatr Dent. 2011 Jun;12(2):87-90
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





