IJCRR - 5(15), August, 2013
Pages: 52-54
Date of Publication: 17-Aug-2013
Print Article
Download XML Download PDF
SERRATUS POSTERIOR MUSCLES: ANATOMICAL PROPERTIES, FUNCTIONAL AND CLINICAL SIGNIFICANCE
Author: Sachin Patil
Category: Healthcare
Abstract:There is significant paucity in the literature regarding serratus posterior superior and inferior muscles. Most standard textbooks mention conflicting views on the role of serratus posterior superior and inferior muscles in respiration. This study was aimed at providing a more accurate review about the serratus posterior superior and inferior muscles and their functional importance. For the preparation of this paper we consulted scientific articles published in English and textbooks. The articles were accessed from a basic search in PubMed database. Recent studies have shown that there is no electromyographic evidence supporting a role for either the serratus posterior superior and inferior muscles in respiration. These muscles may function primarily in proprioception and are clinically important.The serratus posterior superior and inferior muscles are considered to be source of myofascial pain, which presumably originates from trigger points within the muscles. Both muscles are implicated in chronic pain syndromes like idiopathic myalgia or painful shoulder syndrome and scapulocostal syndrome. Further investigation need to be done on these muscles to confirm their functional and clinical importance.
Keywords: serratus posterior, scapulocostal syndrome, trigger points, myofascial pain
Full Text:
INTRODUCTION
Serratus posterior superior (SPS) is a thin quadrilateral muscle, which arises by a thin aponeurosis from the lower part of the nuchal ligament, the spines of the seventh cervical and upper two or three thoracic vertebrae and their supraspinous ligaments.1 But study by Satoh describes origin of SPS as high as third cervical vertebrae while lower limit of origin is upto second thoracic vertebrae.2 Textbook of anatomy by Cunningham’s mentions inferior limit of origin upto fourth thoracic vertebrae.3 SPS is inserted as four digitations attached to the upper borders and external surfaces of the second, third, fourth and fifth ribs, just lateral to their angles. Serratus posterior superior is innervated by the second, third, fourth and fifth intercostals nerves.1
Serratus posterior inferior (SPI) arises from the spines of the lower two thoracic and upper two or three lumbar vertebrae and their supraspinous ligaments by a thin aponeurosis that blends with the lumbar part of the thoracolumbar fascia.1 Textbook of anatomy by Cunningham’s mentions thoracolumbar fascia as only origin of this muscle.3 But study by Satoh describes origin of SPI as high as eleventh thoracic vertebrae.4 It ascends laterally, and its four digitations pass into the inferior borders and outer surfaces of the lower four ribs, a little lateral to their angles. Serratus posterior inferior is innervated by ventral rami of the ninth, tenth, eleventh and twelfth thoracic spinal nerves.1
There is no electromyographic evidence supporting a role for either the SPS or SPI in respiration. Thus, the main evidence suggesting such a role is one the basis of their attachments. The clinical importance of these muscles is that both are implicated in chronic pain syndromes like idiopathic myalgia or painful shoulder syndrome and scapulocostal syndrome.
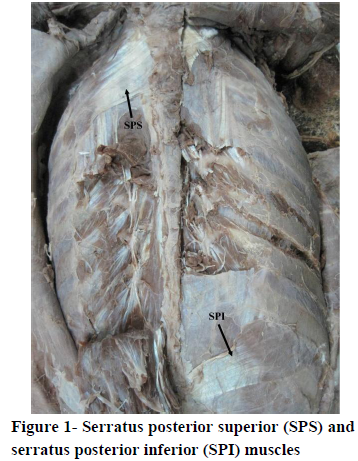
Figure 1- Serratus posterior superior (SPS) and serratus posterior inferior (SPI) muscles
MATERIALS AND METHODS
For the preparation of this paper we consulted scientific articles published in English and textbooks. The articles were accessed from a basic search in PubMed database (http://www.ncbi.nlm.nih.gov/pubmed), using terms like serratus posterior superior, serratus posterior inferior and scapulocostal syndrome. The data concerning anatomy, function and clinical significance of serratus posterior superior and inferior muscles was collected and analysed.
DISCUSSION
The standard textbook of Anatomy mentions conflicting views on function of these muscles.The British edition of Gray's Anatomy indicates that the role of the serratus posterior superior is uncertain in man whereas the American edition describes a specific function for this muscle, namely, elevating the ribs during deep inspiration. Similarly, for the presumably related muscle, serratus posterior inferior , the British edition indicates that the muscle's action is to draw the lower ribs downward and backward, although possibly not in respiration. In contrast, the American edition of this text states that the muscle is active during forced expiration.5 Hollinshead’s Anatomy mentions the serratus posterior muscles as inspiratory muscles which is similar to that stated in clinical anatomy by Moore and Dalley .6,7 But Snell anatomy indicates that the SPS is active in inspiration and the SPI in expiration.8
Regarding the function of muscles other different views are present in previous literatures. Travell and Simons suggested that the SPI functions synergistically with the ipsilateral iliocostalis and longissimus for rotation (unilateral) and extension (bilateral) of the spine while in respiration, the muscle acts synergistically with the quadratus lumborum.5
Vilensky et al suggested that the SPS and SPI have reflex connections with the respiratory muscles such that overstretching results in compensatory movements. The muscles may function to measure stress levels at the superior and inferior limits of the thoracic spine. Considering, the ambiguous relationship between muscle spindle density and presumed proprioceptive function, they suggested that better electromyographic recordings and electroneurography of the motor and sensory nerves of these muscles, rather than further histological analysis, would be the best approach to understanding their function. Authors further stated that until there is supportive evidence, no respiratory function be attributed to either the SPS or the SPI, and that the possible clinical importance of these muscles as generators of pain, especially shoulder pain, which is one of the frequent locations of myofascial pain, should be mentioned in gross anatomy courses and textbooks.5
The scapulocostal syndrome, an insufficiently understood condition was clinically studied in 201 cases by Fourie LJ in 1991. The pain was the presenting symptom in all cases and important cause was from an enthesopathy of the serratus posterior superior muscle. The operation of 'serratotomy' (severing the serratus posterior superior muscle) was performed with excellent results in 6 patients in whom conservative treatment failed. This study supports that SPS is one of the cause of painful shoulder syndrome and scapulocostal syndrome.9
Recent study by Loukas M et al supported that SPS and SPI have role in role in respiration based on their findings that no morphometric difference exists between the SPS and SPI of COPD patients versus controls.10
Further investigation need to be done on these muscles to confirm their functional and clinical importance.
CONCLUSION
We undertook this study with the aim of providing a more accurate report about the serratus posterior superior and inferior muscles, because of interesting relationship with chronic pain syndromes like idiopathic myalgia or painful shoulder syndrome and scapulocostal syndrome. Finally, this study shall be useful for clinicians, surgeons and academics that manipulate and keep particular interest for these mysterious muscles .
ACKNOWLEDGEMENT
Authors acknowledge the great help received from the scholars whose articles cited and included in references of this manuscript. The authors are also grateful to authors/ publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
- Standring, S. (Ed). Gray's Anatomy: The Anatomical Basis of Clinical Practice 40th ed. New York: Churchill Livingstone.2008;2729-31.
- Satoh JI. The serratus posterior superior in certain catarrhine monkeys and man, in particular the structure of the muscular digitations and their nerve supply. Okajimas Folia Anat Jpn. 1969; 46:65-122.
- Sinclair DC. Muscles and fasciae, In: Romanes GJ (ed) Cunningham’s textbook of anatomy. 12th eds. Oxford: Oxford University Press, 1981; 352.
- Satoh J I. The serratus posterior inferior in monkey and man, in particular the structure of the digitations of this muscle and their nerve supply. Okajimas Folia Anat jpn. 1970; 47:19-61.
- Vilensky JA, Baltes M, Weikel L, Fortin JD, Fourie LJ. Serratus posterior muscles: anatomy, clinical relevance, and function. Clin Anat. 2001 ;14(4):237-41.
- Hollinshead WH,Rosse C( eds). In: Textbook of anatomy. 4th ed. Philadelphia.1985;309-310
- Moore KL, Dalley AF II. Clinically oriented anatomy. 4th ed. Baltimore: Lippincott Williams and Wilkins. 1999; 80.
- Snell RS. Clinical anatomy for medical students. Baltimore: Lippincott Williams and Wilkins. 2000; 58.
- Fourie LJ. The scapulocostal syndrome. S Afr Med J 1991; 79:721-724.
- Loukas M, Louis RG Jr, Wartmann CT, Tubbs RS, Gupta AA, Apaydin N, Jordan R. An anatomic investigation of the serratus posterior superior and serratus posterior inferior muscles. Surg Radiol Anat. 2008;30(2):119-23.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





