IJCRR - 5(15), August, 2013
Pages: 42-45
Date of Publication: 17-Aug-2013
Print Article
Download XML Download PDF
ROLE OF FINE NEEDLE ASPIRATION CYTOLOGY IN DIAGNOSING THYROID LESIONS - A RETROSPECTIVE STUDY
Author: Pratibha Vyas, Sulabh Bansal, Tarun Ojha, Amit Singhal, Suresh Kumar
Category: Healthcare
Abstract:Background: One of the most common problems among patients attending ENT OPD (particularly female patients) is the thyroid enlargement. Though Thyroid cancer is not common; incidence of Thyroid nodule (Simulating thyroid cancer in appearance) is high. This study was conducted to evaluate efficacy of Fine Needle Aspiration Cytology (FNAC) at Mahatma Gandhi Medical College & Hospital, Jaipur in diagnosing thyroid lesions (benign or malignant) and to compare its advantages & results with histopathology. Method: This retrospective study was conducted in Department of ENT and Head-Neck surgery at Mahatma Gandhi Medical College and Hospital, Jaipur during the period January 2008 to January 2013. In all 282 cases were evaluated by detailed history, thorough clinical examination, ultrasonography (USG) of neck, complete thyroid profile (Serum T3, Serum T4 & Serum TSH) and histopathology of thyroid lesion. Results: In our study, sensitivity and specificity of FNAC was 70.2% and 97.3% respectively (in diagnosing thyroid lesions as benign and malignant). Conclusion: FNAC is safe, less expensive, less invasive and cost effective diagnostic tool in diagnosing thyroid lesions and distinguishing benign from malignant ones.
Keywords: Thyroid, FNAC, Malignant, Cytology
Full Text:
INTRODUCTION
Thyroid lesions are quite prevalent and globally thyroid enlargement affects 15% of the population.1But incidence of thyroid cancer is very low i.e. 3.6 per 100,000 population (.0036 percent)2
The most common indication for thyroid surgery is presence of Thyroid nodule which may be benign or malignant. Prevalence of thyroid nodule is about 4-7%.3 Because of very low incidence of thyroid cancer; thyroid nodules must be identified as benign or malignant; as treatment options in both the conditions are different. Thyroid cancers are treated surgically, while benign lesions must be followed strictly.4
FNAC was first reported in 1930 by Martin and Ellis.5 Since then, it has become reliable and cost effective method to distinguish benign from malignant lesion in neck. 6
FNAC is technically easy to perform, safe and inexpensive diagnostic tool. Sensitivity of FNAC in detecting malignancy in thyroid lesions is high.7 Any solitary or dominant nodule larger than 1 cm should be subjected for FNAC as smaller nodules carry very low risk of morbidity.8
Many studies show accuracy rate of FNAC more than 80%.9 Pitfalls of FNAC include false negative and false positive results, inadequate aspirate and suspicious results.10
Present retrospective study was conducted to evaluate efficacy of FNAC in diagnosis of thyroid lesions and to compare the results with histopathology after surgery.
MATERIAL AND METHODS
This study was conducted at Mahatma Gandhi Hospital and Medical College, Jaipur in the Departments of ENT and Head-Neck Surgery during the period between January 2008 and January 2013. Patients with features of hyperthyroidism, Hot and toxic nodule were excluded from the study. Patients with systemic diseases for example hypertension or hepatic or renal failure were also excluded from the study. A detailed history was taken followed by thorough clinical examination, thyroid profile, USG neck, and FNAC.
CT scan was advised in patients in whom malignancy was suspected to see the extent of tumour. After surgery the specimen was sent for HPE in 10% formaldehyde. The specimen was properly labeled.
RESULTS
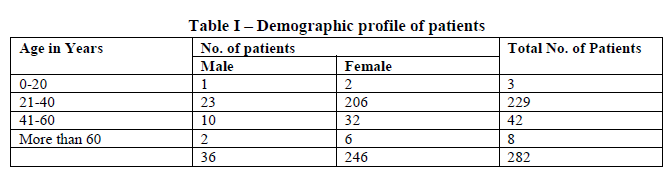
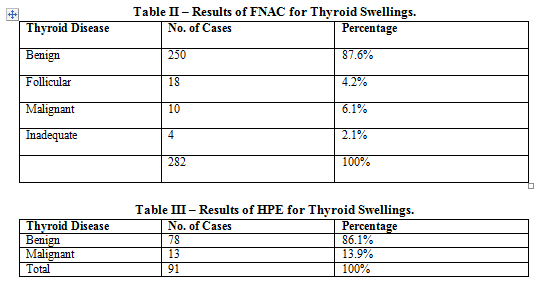
In our series of 282 patients, 31 were male and 251 were females with male to female ratio being 1:9. Duration of thyroid swelling in the present study was from 4 months to 5 years. The average size of Goiter was 2-3 cm. The highest incidence of thyroid lesion was found in the age group of 20-40 years. On FNAC, 250 (87.6%) cases were benign as compared to 10 (6.1%) malignant cases.
DISCUSSION
To evaluate a thyroid nodule, a battery of investigations is needed including USG neck, thyroid profile, thyroid imaging, complimented by thorough clinical evaluation.
In diagnosing thyroid neoplasms, the highest rate of sensitivity and specificity is achieved by FNAC.2
A complication rate for FNAC is low. 2Complications include hematoma, tracheal puncture and transient laryngeal palsy.11 Tumour implantation following FNAC is reported only once.12
In our study, sensitivity and specificity of FNAC in diagnosing thyroid lesions is 70.2% and 97.3% respectively. Humberger reported sensitivity at 65.53% and specificity at 72-100%.13 In a study by Safirullah 94.2% sensitivity and 94% specificity in diagnosis of Malignant thyroid diseases was reported.
Results of this study are comparable with other data. Agrawal et. al. (1995)14 in Tata Memorial Hospital, Mumbai found accuracy of FNAC to be 90.9% in evaluating thyroid nodules, Kumar et.al. (2008) 15 reported accuracy of 97.7%. Both these findings are comparable with our study.
Reported sensitivity, specificity, and accuracy of Thyroid FNAC in detecting malignancies are between 65 – 98%, 72 – 100%, 65 – 95% respectively. 16, 17, 18
CT guided and US guided FNAC have a higher probability of accuracy along with any wet stain.8
FNAC has some very distinct advantages. It requires no preprocedural investigations or hospitalization. As a result, it is very easy to convince patients to give consent to it. Patients were also very willing as it reduced their expenditure, which otherwise they would have had to incur; had they opted for open biopsy. Post procedure complications are also very rare.
CONCLUSION
This study conclusively shows that FNAC could be first line diagnostic test in any case of thyroid swelling. FNAC of thyroid swelling is very safe, accurate, much less expensive, relatively simple and five minute OPD procedure. FNAC being much less expensive and quite painless is very well accepted by patients. With all these advantages, FNAC is very effective tool in diagnosis of thyroid pathology. Though FNAC is not the substitute for conventional open biopsy and subsequent histopathology, particularly in old patients but definitely should be first choice in diagnostic modalities in any case of thyroid swelling.
References:
- JA Franklyn, J Daykin, J Young, et.al.: Fine needle aspiration cytalogy in diffuse or multinodular goitre compared with solitary thyroid nodule, BMJ 1993; 307: 240
- Theodar R. Miller, MD; John S., et.al.: Fine-Needle Aspiration Biopsy in the management of thyroid Nodules : West J Med 134: 198-205, Mar 1981
- Wienke JR, Chong WK, Fielding JR, et.al.: Sonographic features of benign thyroid nodules. J Ultrasound Med 2003; 22:1027-31
- Polyzos SA, Kita M, Avarmindis A. Thyroid nodules-stepwise diagnosis and management. Hormones (Athens) 2007; 6: 101-9
- Martin HE, Ellis EB; Biopsy by needle puncture and aspiration. Ann Surg. 1930; 92: 169-81
- Lowhagen T, Gargberg P.O., Ludell G, et.al.: Aspiration biopsy cytology (ABC) in nodules of the thyroid gland suspected to be malignant. Surg. Clin N Am 59: 3-18, 1979.
- Mahar SA, Hussain A, Islam N. Fine needle aspiration cytology of thyroid nodule; diagnostic accuracy and pitfalls. J Ayub Med Coll Abbottabad 2006: 18 (4): 26-9
- Arup Sengupta, Ranbir Pal, Sumit Kar, et.al. J. Natural Science, Biology, Medicine. 2011; 2(1) 113-118
- Gharib H. Diffuse nontoxic and Multinodular goitre. Curr Ther Endocrinal Metab 1944; 5: 99-101
- Baloch MN, Ali S, Ansari MA, et.al.. Contribution of Fine needle apsiration cytology in the diagnosis of malignant thyroid nodules Pak J. Surg 2008; 24(1) : 19-21
- Wang C, Vickery A, Maloog F: Needle biopsy of thyroid. Surg Gynocol obs 143: 365-368, 1976
- Sinner WN, Zajicek J; Implantation metastasis after percutaneous transthoracic needle aspiration biopsy. Acta Radial [Diagn] (Stockh) 17: 473-479, 1976
- Humberger JI. Diagnosis of Thyroid nodule by fine needle aspiration cytology of thyroid nodules. J Clin Endorcinal metab 1994, 79:335-9
- Agrawal A, Mishra SK. Completion total thyroidectomy in the management of differentiated thyroid carcinoma. Aust N Z J Surg 1996;66:358-60.
- Kumar S, Aqil S, Dahar A. Role of fine needle aspiration cytology in thyroid disease. J Surg Pak 2008;13:22-5.
- Gharib H. Fine needle aspiration biopsy of thyroid nodules: advantages, limitations and effects. Mayo Clinic Proc 1994;69:44-9.
- Hamburger JI. Diagnosis of thyroid nodules by fine needle biopsy: Use and Abuse. J Clin Endocrinal Metab 1994;79:335-9.
- Ali K. Ageep. Efficacy of Fine needle aspiration cytology in the diagnosis of thyroid swelling in Red Sea State, Sudan. Sudan JMS Vol 8 Issue 1, March 2013.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





