IJCRR - 5(16), August, 2013
Pages: 35-37
Date of Publication: 28-Aug-2013
Print Article
Download XML Download PDF
A COMPLICATED BANG'S DISEASE - CASE REPORT
Author: Sunny D.A.N., Amirtha B.G., Tevethia H.V., Kadavanu T., Panchbhaya R., Siva P.K., Somasundsaram S.
Category: Healthcare
Abstract:An uncommon organism or IE at an uncommon site is sufficient to create a diagnostic concondrum. Since its signs and symptoms are nonspecific, getting an absolute etiological diagnosis becomes a herculean task. A 45 year old man presented with fever, drenching sweats, right shoulder pain, low back ache and weight loss for 9 months. He gives history of travel to the middle east and was a gardener by occupation. H/O Ingestion of Unpasteurized milk was present. H/O rearing farm animals in middle east was present. Blood cultures were negative, 2D echo and Trans esophageal echo confirmed the presence of vegetations, So with the specific history IgM antibody for Brucella melitensis was done and showed positive. The titres showed 1:320. A Lumbosacral and Hip X-ray showed Sacroilitis. He was started on streptomycin and doxycycline. After 1 week he developed acute onset of breathlessness subsequently went to cardiogenic shock and was diagnosed to have rupture of sinus of valsalva and acute aortic regurgitation. He was immediately taken up for surgery for valve replacement. He is doing well on subsequent post operative follow ups. The purpose of presenting this case report is that, brucellosis is very rare and is an even rarer cause of endocarditis in our country. It also signifies the importance of detailed history taking in terms of travel and occupational history. Brucella accounts for 2% of all IE cases. We here present a case diagnosed as brucella endocarditis, who had later landed up in complications.
Keywords: Brucellosis, Endocarditis
Full Text:
INTRODUCTION
Brucellosis has been present for over a millennia1 . Brucella accounts for less than 2% of all infective endocarditis (IE) cases2 . We here present a case diagnosed as brucellosis who later presented with complications.
CASE REPORT
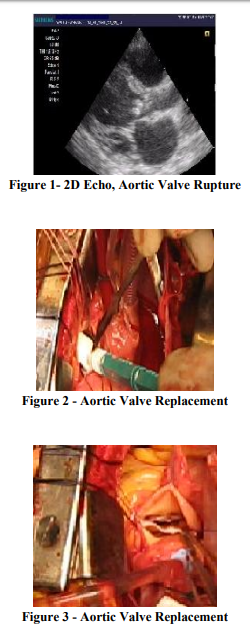
A 45 year old man presented with fever, drenching sweats, right shoulder pain, low back ache and weight loss for 9 months. He travelled to the middle east and was a gardener (who used to rear farm animals) by occupation. He had Ingested Unpasteurized milk. On Examination his was pulse96/min, Blood pressure-120/70 mmHg, On auscultation a grade 2/6 Ejection Systolic murmur with soft Early Diastolic Murmur was present in the Aortic area, other systems were within normal limits. Investigations showed High Serum Transaminases levels with all other routine investigations being normal. Blood cultures were negative, 2D echo and Trans esophageal echo confirmed the presence of vegetations with normal left ventricular function, IgM antibody for Brucella melitensis was positive in which titres showed 1:320. A Lumbosacral and Hip X-ray showed Sacroilitis, Right Shoulder X-ray showed peri arthritis. Tuberculin test was negative. He was started on streptomycin and doxycycline. He was discharged at request due to his personal reasons. He presented to the ER after 1 week with acute onset of breathlessness with cardiogenic shock and was diagnosed as rupture of sinus of valsalva and severe aortic regurgitation with moderate left ventricular dysfunction. He was immediately taken up for surgery for valve replacement. He was doing well on subsequent post operative follow ups.
DISCUSSION
Brucellosis is common over a wide regionof middle-east.3 . About half a million cases of brucellosis have been reported worldwide, though detection rate varies around 30-40% of actual incidence10 . Although Brucellaendocarditis is a rare entity, it is associated with high mortality rates in animals in the Middle East, Brucella melitensis (serovar 2 or 3) predominates; in humans, serovar 3 is the cause of most cases3 . Brucellosis often involves the spine4 . Peripheral arthritis is the most common and is nonerosive5 . A second form, characterized by sacroiliitis6 . This patient had both fever and osteoarticular disease. In Suspicion of endocarditis, a transesophageal echocardiogram may help with the diagnosis2 . Culture, though considered as gold standard, is not being always positive, isolation rates varying from 20 to 50% and may take up to one month and molecular techniques like PCR, though sensitive and specific,9 are not available at all places due to limitation of resources. Endocarditis remains the principal cause of mortality in the course of brucellosis,It usually involves the aortic valve and typically requires immediate surgical valve replacement. Early recognition, adequate antibiotic treatment, and the absence of signs of heart failure can guide the practitioner toward prolonged, conservative treatment7 . Vegetations were revealed on transthoracic echocardiography. The treatment was given as per guidelines. The streptomycincontaining regimen is slightly more efficacious in preventing relapse8 . In this patient the guideline treatment was initiated at the earliest and after surgery which lead to drastic improvement.
CONCLUSION
The purpose of presenting this case report is that, brucellosis is very rare and is an even rarer cause of endocarditis in our country. It also signifies the importance of detailed history taking in terms of travel and occupational history. Optimization of medical therapy for cardiac failure which has normalized ventricular function in this patient during his follow ups. We hereby stress the role of optimal medical therapy in addition to surgery.
References:
1. Capasso L. Bacteria in two-millennia-old cheese, and related epizoonoses in Roman populations. J Infect 2002;45:122-127
2. Mylonakis E, Calderwood SB. Infective endocarditis in adults. N Engl J Med2001;345:1318-1330
3. Refai M. Incidence and control of brucellosis in the Near East region. Vet Microbiol 2002;90:81-110
4. Bouaziz MC, Ladeb MF, Chakroun M, Chaabane S. Spinal brucellosis: a review. Skeletal Radiol2008;37:785-790
5. Bosilkovski M, Krteva L, Caparoska S, Dimzova M. Hip arthritis in brucellosis: a study of 33 cases in the Republic of Macedonia (FYROM). Int J Clin Pract 2004;58:1023-1027
6. Ariza J, Pujol M, Valverde J, et al. Brucellar sacroiliitis: findings in 63 episodes and current relevance. Clin Infect Dis 1993;16:761-765
7. Reguera JM, Alarcon A, Miralles F, Pachon J, Juarez C, Colmenero JD. Brucella endocarditis: clinical, diagnostic, and therapeutic approach. Eur J Clin Microbiol Infect Dis 2003;22:647-650
8. Solera J, Martinez-Alfaro E, Saez L. Metaanalysis of the efficacy of rifampicin and doxycycline in the treatment of human brucellosis.Med Clin (Barc) 1994;102:731-738
9. Probert WS, Schrader KN, Khuong NY, Bystrom SL, Graves MH. Real-time multiplex PCR assay for detection of Brucella spp, B. abortu s and B. melitensis. J Clin Microbiol 2004; 42 :1290-3.
10. World Health organization; Fact sheet N173. World Health Organization: Geneva; 1997.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





