IJCRR - 5(17), September, 2013
Pages: 116-123
Date of Publication: 12-Sep-2013
Print Article
Download XML Download PDF
THE NERVE SUPPLY TO EXTENSOR CARPI RADIALIS BREVIS MUSCLE - A STUDY
Author: Jayakumar V. R., Roshni Bajpe, Shubha R.
Category: Healthcare
Abstract:Aim: To study the nerve supply to extensor carpi radialis brevis muscle. Materials and methods: 50 upper limbs of adult human cadavers irrespective of sex were studied in the Department of Anatomy at Kempegowda institute of medical sciences, Bengaluru, Karnataka, the nerve supply to extensor carpi radialis brevis (ECRB) muscle was observed. Study was done by dissection method. The following parameters: source of nerve to ECRB, site of division of radial nerve in relation to lateral epicondyle were noted and the distance between origin of nerve to ECRB and point of entry into the muscle was measured. Results: In 29 specimens the nerve supply to extensor carpi radialis brevis was from posterior interosseus nerve (PIN), in 12 specimens from superficial branch of radial nerve and in 9 specimens from the angle of bifurcation of radial nerve and none of the specimens showed innervation from the radial nerve trunk. In 33 specimens, radial nerve divided at the level of lateral epicondyle, in 15 specimens it was above the level of lateral epicondyle and in 12 specimens showed division below the level of lateral epicondyle. Average length of nerve to ECRB on right and left side was found to be 4.4 cm and 4.1 cm respectively. Conclusion: In 24% of specimens the nerve supply to extensor carpi radialis brevis was from the superficial branch of radial nerve, the knowledge of which is clinically important for surgeons and orthopaedicians before undertaking surgical procedures such as free functional muscle transfer, tenotomy etc.
Keywords: Radial nerve, posterior interosseus nerve, lateral epicondyle, tenotomy.
Full Text:
INTRODUCTION
Extensor carpi radialis Brevis (ECRB) is one of the superficial muscles of the extensor compartment of the forearm. It arises from the lateral epicondyle of the humerus by a tendon of origin along with other forearm extensors, the radial collateral ligament of the elbow joint, from a strong aponeurosis which covers its surface and adjacent intermuscular septa. The tendon passes under extensor retinaculum and is attached to the dorsal surface of the base of the third metacarpal on its radial side, distal to styloid process and on adjoining parts of the second metacarpal bone1 . The muscle acts to extend and radially abduct the hand. It also stabilises the wrist when the fingers are flexed2 . The extensor carpi radialis brevis is innervated by posterior interosseus nerve (PIN) C7 and C8. Branches to ECRB may arise from the main trunk of radial nerve or from the beginning of the superficial branch of radial nerve1 . The radial nerve, a continuation of the posterior cord of brachial plexus consists of fibres from C6, C7, C8 and sometimes T1. It is primarily a motor nerve that innervates the triceps; the supinators of the forearm; and the extensors of the wrist, fingers, and thumb. This nerve is injured most often by fractures of the humeral shaft. Gunshot wounds are the second most common cause of radial nerve injury. Other causes include lacerations of the arm and proximal forearm, injection injuries, and prolonged local pressure. Roles and Maudsley emphasized that entrapment of the posterior interosseous nerve can cause chronic and refractory tennis elbow. Such entrapment is called radial tunnel syndrome and one of the potential compressive anatomical structures is the origin of the extensor carpi radialis brevis muscle. When entrapment is caused by other conditions, however especially in the forearm, surgical exploration and decompression of the nerve usually are beneficial3 . Previous studies done by Salisbury (1938) showed that nerve to ECRB arises most frequently from the superficial branch of radial nerve in 56% limbs4 ; Al-Qattan (1996) reported 48% from superficial branch and 20% from the radial nerve trunk2 . In a recent report by Sharadkumar et al (2012) 42% of specimens were innervated by superficial branch of radial nerve5 . It is a universally accepted axiom that the variation in nerve supply to any muscle, particularly in an extremity is of definite surgical importance.
MATERIALS AND METHODS
The present study was done on 50 upper limbs (26 right sides and 24 left sides) of adult human cadavers irrespective of sex in the Department of Anatomy, Kempegowda institute of medical sciences, Bengaluru, Karnataka. The study was done by dissection method. The nerve to extensor carpi radialis was identified in all the specimens and its length was measured with maximum accuracy using a measuring scale. The following observations were recorded. i. Site of division of radial nerve in relation to lateral epicondyle ii. Number of terminal branches of the radial nerve iii. Source of the nerve to ECRB i.e. radial nerve trunk above its division, angle of its bifurcation, deep branch or superficial branch of radial nerve iv. Distance between origin of nerve to ECRB and point of entry into the muscle
RESULTS
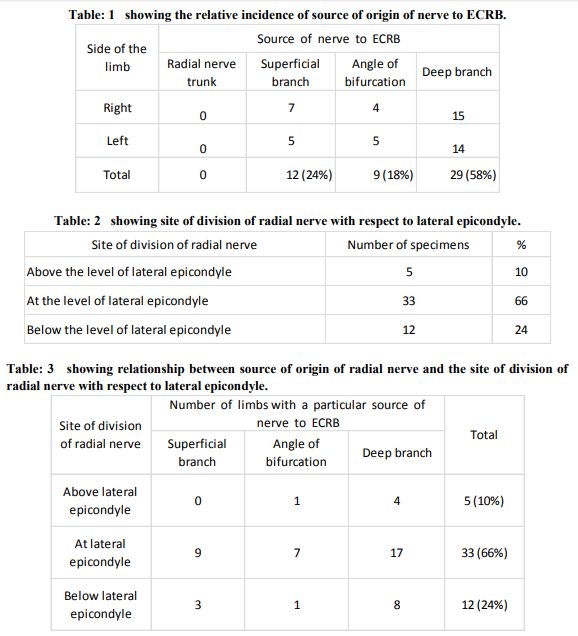
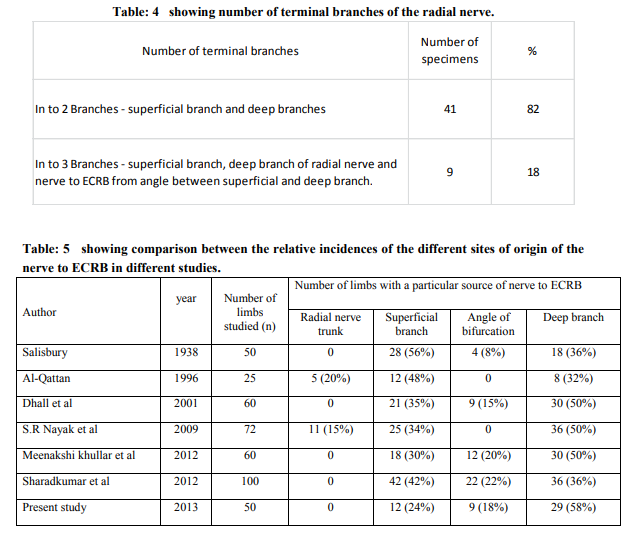
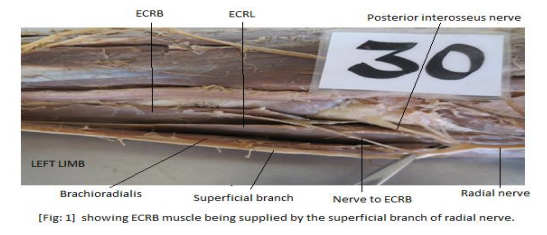
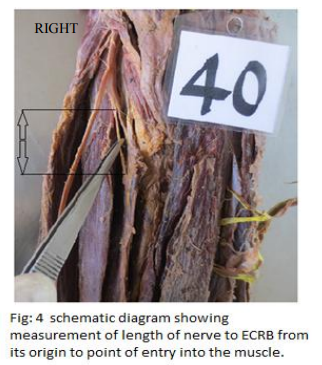
The nerve to extensor carpi radialis brevis arose most commonly from the deep branch of radial nerve in 58% specimens, followed by superficial branch in 24% and from the angle of bifurcation of radial nerve between superficial and deep branch in 18% of the specimens. None of the specimens showed innervation from radial nerve trunk before dividing into terminal branches (Table-1 / Fig: 1, 2, and 3). The radial nerve divided most commonly at the level of lateral epicondyle in 66% limbs, followed by its division below the level of lateral epicondyle in 24% limbs and in the rest 10% it divided above the level of lateral epicondyle (Table-2 and 3). In 82% of the limbs the radial nerve divided into two branches, superficial and deep; in the remaining 18% limbs it showed three divisions, the third being the nerve to ECRB arising from the angle between the superficial and deep branches of radial nerve (Table- 4). Average length of nerve to ECRB from its origin to point of entry into the muscle on right and left sides were 4.4 cm and 4.1 cm respectively. Maximum and minimum length of the nerve was found to be 7.7 cm and 2 cm on the right side and 7.4 cm and 2.3 cm on the left side respectively (Fig: 4).
DISCUSSION
The source of origin of nerve to ECRB has presented many variations in the previous studies, originating either from radial nerve trunk, superficial branch of radial nerve or deep branch of radial nerve or from angle of bifurcation of radial nerve between its superficial and deep branches (Table-5).
The incidence of the nerve supply to ECRB from superficial branch of radial nerve has been reported by Salisbury (1938) in 56% limbs and AlQattan (1996) in 48% of the limbs2, 4. The present study showed that this was the case in 24% of the specimens. The variation in the incidence of innervation of ECRB by superficial branch of radial nerve in different studies may be due to racial factors6 . Dhall et al. (2001) studied 60 specimens and reported the origin of nerve to ECRB from superficial branch in 35% limbs and from deep branch in 50% and from the angle of bifurcation in 15% specimens7 . S.R Nayak et al (2009) studied 72 limbs the origin, nerve supply to ECRB and its role in lateral epicondylitis. In their study, 11 specimens (15%) showed nerve to ECRB arising from radial nerve trunk, in 36 specimens (50%) it arose from deep branch and in 25 specimens (34%) from the superficial branch of radial nerve8 . Among 60 upper limbs that were studied by Meenakshi Khullar et al (2012), the nerve to ECRB arose from deep branch in 50% specimens, 30% from superficial branch and remaining 20% from the angle of bifurcation of radial nerve6 . Sharadkumar et al (2012) recently studied 100 specimens and found that nerve to ECRB arose mostly from the superficial branch in 42 specimens, from deep branch in 36 specimens and from the angle of bifurcation in 22 specimens5 . Division of radial nerve trunk with respect to lateral epicondyle was observed. In studies done by Dhall et al, Meenakshi Khullar et al and Sharadkumar et al the division of radial nerve trunk occur most commonly above the level of lateral epicondyle. In present study it was found to divide at the level of lateral epicondyle in most (66%) specimens5, 6, and 7 . In the present study, we measured the length of the nerve to ECRB as an average of 4.4 cm and 4.1 cm on the right and left sides respectively. S.R Nayak et al observed the above distance at an average of 4.3 cm and 4 cm on right and left sides which is similar to our study. The data regarding the length of the nerve will help the surgeons while exploring the elbow region during the surgical decompression of the posterior branch of radial nerve in between the ECRB and Extensor carpi radialis longus (ECRL) muscles8 . Number of terminal branches of radial nerve has been studied previously. The radial nerve terminated as either 2 branches (superficial and deep branch) or as 3 branches (superficial branch, deep branch and nerve to ECRB from the angle between the superficial and deep branch). Dhall et al reported 85% showed two branches and 15% presented with three branches8 . Meenakshi et al found that nerve divided into two branches in 80% and into three branches in 20% specimens6 . Sharadkumar et al. reported 78% specimens with two branches and 22% with three branches. Present study showed radial nerve termination into two branches in 82% limbs and 3 branches in 18% limbs5 . Variations in the origin of the nerve to extensor carpi radialis brevis muscle are clinically important. ECRB muscle may be spared in injuries to the posterior interosseus nerve thereby explaining the preservation of some wrist function clinically after penetrating injuries which may otherwise result in a complete wrist drop6 . Lacerations of the radial aspect of the proximal forearm resulting in injury to the superficial radial nerve may also involve the nerve to ECRB. Preoperatively, isolated paralysis of ECRB is difficult to detect on clinical examination in the acutely injured patient because weakness of wrist extension may be attributed to pain. Surgical exploration of these cases should therefore include identification of the motor nerve to ECRB2 . Traumatic transection of the superficial radial nerve in the distal forearm may result in a painful neuroma. One of the options is to transect the superficial radial nerve in the proximal forearm and to bury the proximal nerve stump in muscle. If this option is chosen, transection of the superficial radial nerve should be performed distal to its motor branch to ECRB2 .
Recently, ECRB has also gained importance for use in ‘free functional muscle transfer’ i.e. transfer of a muscle with its motor nerve and vascular pedicle from one site of the body to another site in order to restore the motor function. So knowledge of the variations in the origin of its nerve supply is thus important while this muscle is being harvested6 . The normal origin and the course of the nerve to ECRB lie very close to the posterolateral aspect of the radius, a frequent site of pathology, trauma and surgical procedures. The anterior approach to the elbow and the variations in this approach are used frequently in the surgical management of proximal radial fractures as well as variety of other pathologies. Such manoeuvres involve the separation of the ECRB distally with resultant exposure of radial nerve and its branches. Hence the knowledge of variations of nerve supply to the ECRB will assist the surgeon in avoiding an inadvertent injury due to placement of retractors5 . Repeated contraction of wrist extensor muscles especially the ECRB which may compress the deep branch of radial nerve at the elbow during pronation leading to lateral epicondylitis or tennis elbow8 . In tennis elbow muscle involved is ECRB. The non-inflammatory, chronic degenerative changes occur in the origin of ECRB. The surgeons performing ‘Z’ shaped tenotomy on tennis elbow to lengthen the tendon of ECRB must be aware of this variation in order to avoid unwanted complications5 .
CONCLUSION
Our study emphasizes that the nerve supply to ECRB from the superficial radial nerve is not a rare occurrence. The awareness is clinically important for surgeons dealing with compressive neuropathies and orthopaedicians operating on the fractures of the lower end of humerus and plastic surgeons performing free functional muscle transfer. A lack of knowledge of such variations might prove to be a hindrance to the operating surgeons.
ACKNOWLEDGEMENT
The author is thankful to the Department of Anatomy, Kempegowda institute of medical sciences, Bengaluru, for giving an opportunity to do the study. All the authors are grateful to the authors and publishers of those articles or books that are cited in references from where the literature has been reviewed and discussed.
References:
1. Standring S, Borley NR, Collins P, Crossman AR, Gatzoulis MA, Healy JC, et al.Gray’s Anatomy : The Anatomical Basis Of Clinical Practice. 40th ed. London: Elsevier Ltd; 2008;P.849,856.
2. Al-Qattan M.M. The nerve supply to the extensor carpi radialis brevis. J Anat 1996;188:249-50.
3. Canale ST, Campbell’s Operative Orthopaedics. 10th ed. Mosby Ltd; 2003; vol 4: p. 3257.
4. Salisbury CR. The nerve to the extensor carpi radialis brevis. Brit J Surg 1938;26:95– 98.
5. Sawant SP, Shaikh ST, Lele SD, et al. Study of nerve supply of extensor carpi radialis brevis muscle. International Journal of Analytical, Pharmaceutical and Biomedical sciences 2012;1(4):63-70.
6. Khullar M, Kalsey G, Laxmi V, Khullar S. Variations in the nerve supply to the extensor carpi radialis brevis. Journal of Clinical and Diagnostic Research 2012;6(1):13-16.
7. Dhall U, Kanta S. Variations in the nerve supply to extensor carpi radialis brevis. J Anat Soc India 2001;50(2):134-136.
8. Nayak SR, Ramanathan L, Krishnamurthy A, et al. Extensor carpi radialis brevis origin, nerve supply and its role in lateral epicondylitis. Surg Radiol Anat 2010;32(3):207-211.

|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





