IJCRR - 5(17), September, 2013
Pages: 112-115
Date of Publication: 12-Sep-2013
Print Article
Download XML Download PDF
AN ANOMALOUS CORACOBRACHIALIS MUSCLE - A CASE REPORT
Author: Surwase Ramdas Gopalrao, Lakshmi Rajgopal
Category: Healthcare
Abstract:Coracobrachialis a muscle of flexor compartment of the arm is usually attached proximally to the tip of the coracoid process of scapula along with short head of biceps brachii and distally attached to the medial border of middle of shaft of humerus. During routine dissection of the upper limb, an anomalous coracobrachialis muscle was found on the left arm of a male cadaver. Its proximal attachment was from the fibrous band of medial intermuscular septum of arm. Its distal attachment was to the medial epicondyle of humerus and to the antebrachial fascia. Median nerve and brachial artery were seen passing deep to this muscle. This variation is important for clinicians and radiologists.
Keywords: coracobrachialis inferior muscle, Wood’s muscle, musculocutaneous nerve, brachial artery, median nerve, fibrous tunnel.
Full Text:
INTRODUCTION
Coracobrachialis is a muscle of the flexor compartment of the arm. It is attached proximally to the tip of the coracoid process of the scapula together with the tendon of short head of biceps brachii. It ends on an impression, 3-5 cm in length, midway along the medial border of the middle of the humeral shaft between the attachment of triceps and brachialis, where the nutrient foramen of the bone is usually located. It is supplied by the musculocutaneous nerve (C5, C6 and C7), a branch from the lateral cord of the brachial plexus. This nerve supplies the muscle before piercing it and then courses further between biceps brachii and brachialis 1, 2 . Many variations regarding the origin of coracobrachialis, course of related arteries and the positioning of the neurovascular bundle behind the muscle have been described which may result in compression of the neurovascular bundle 3 . These variations remain unnoticed during life, until they become symptomatic and receive the attention of the surgeons or noticed by anatomists during dissection. Several variants of insertion of coracobrachialis muscle have also been described in literature. Coracobrachialis has been reported to insert as an accessory slip to the lesser tubercle, medial epicondyle or medial intermuscular septum. Wood in 1867 and El-Naggar and Zahir in 2001 have described coracobrachialis having distal attachment to the medial epicondyle of humerus or to the medial intermuscular septum of arm, blending with the medial head of the triceps muscle 4, 5 . According to Bergman et al, coracobrachialis muscle actually consists of three parts: i) A proximal part arising from the coracoid process of the scapula and inserted onto the humerus close to the lesser tubercle; ii) A middle part of intermediate size; iii) A distal part, which is the largest and the most superficially placed 6 . In human beings, the proximal and the middle parts are the most constantly present. Distal portion is sometimes present in the form of coracobrachialis inferior or longus (according to Wood, 1867)4 and may be attached to the humerus or to a fibrous band of medial intermuscular septum or even to the medial humeral epicondyle. Knowledge of such variation is of considerable importance during invasive and non-invasive investigative procedures or during orthopedic and reconstructive surgical procedures7 .
CASE REPORT
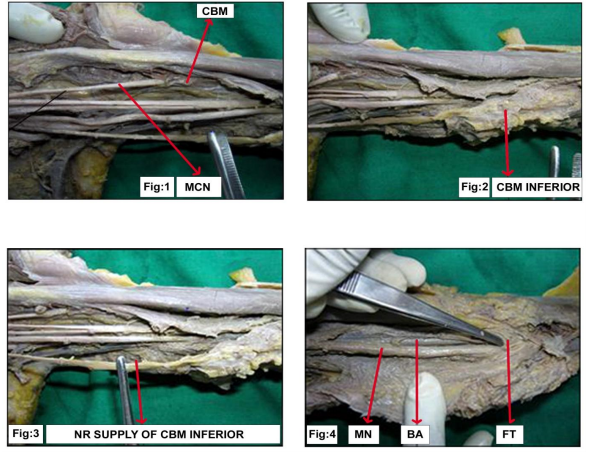
During routine dissection of cadavers, in one left arm, an anomalous coracobrachialis inferior muscle was found. In this specimen, the proximal attachment of coracobrachialis was to the tip of coracoid process along with the short head of biceps brachii and its distal attachment was to the medial border of middle of shaft of humerus. It was seen that musculocutaneous nerve supplied and then pierced the muscle (Fig. 1). Distal to the normal coracobrachialis muscle, an accessory coracobrachialis muscle was found having a proximal attachment to the humerus distal to the insertion of normal coracobrachialis and also to the fibrous band of medial intermuscular septum of arm (Fig. 2). Its distal attachment was to the medial epicondyle of humerus and to the antebrachial fascia. This muscle fits in with the description of coracobrachialis longus or coracobrachialis inferior as described by John Wood in 1867 4 . In this case, it was found that coracobrachialis inferior was supplied by a nerve branch arising directly from the medial cord of brachial plexus (Fig. 3). Deep to the coracobrachialis inferior, there was a fibrous tunnel [which was formed by the medial intermuscular septum from which this muscle was arising] through which the median nerve and the brachial artery were passing (Fig. 4).
DISCUSSION
Variations of the insertion of coracobrachialis are classified by James Doyle et al as proximal and distal 8 . Proximal insertional variation may be to i) Surgical neck of humerus; ii) Capsule of the shoulder joint; iii) Bicipital ridge of humerus about 1 cm distal to the lesser tubercle. The latter variation is called as coracobrachialis superior or coracobrachialis rotator humerii or Gruber’s muscle. Embryologically, this may be the superior portion of the coracobrachialis muscle. Of the proximal insertions, some may be additional slips extending to various structures in the shoulder area like the tendon of latissimus dorsi, the tendon of teres major or the lesser tubercle of humerus. Of these, an accessory slip of coracobrachialis arising from the coracoid process, crossing the radial nerve in the axilla and inserting into the tendon of latissimus dorsi has been named as coracobrachialis minor or le court coracobrachialis of Cruveilhier 8 . Variant distal insertions may be to i) Distal medial margin of humerus / Medial supracondylar ridge; ii) Medial epicondyle; iii) Fibrous band of medial intermuscular septum (Internal brachial ligament); iv) Anomalous supracondylar process; v) Ligament of Struthers; vi) Antebrachial fascia. An anomalous coracobrachialis muscle which is inserted farther distally than usual is referred to as coracobrachialis longus or coracobrachialis inferior or Wood’s muscle 8 . In the case under discussion, the coracobrachialis muscle had a normal origin and a normal insertion and an additional slip was found to prolong into distal arm covering median nerve and brachial artery and getting inserted on to the medial epicondyle and antebrachial fascia. This additional slip is coracobrachialis longus or inferior or Wood’s muscle. This muscle also had an independent nerve supply directly from the medical cord of brachial plexus and such a finding is so far not reported.
CLINICAL SIGNIFICANCE
From clinical viewpoint, the muscle insertion into the medial epicondyle and antebrachial fascia would create a narrower anterior compartment during contraction of coracobrachialis muscle and could produce proximal median neuropathic symptoms and brachial artery compression. Entrapment of median nerve and brachial artery by tendinous arch of coracobrachialis has been reported recently 9 . This additional muscle may cause musculocutaneous or high median nerve paralysis 10, 11, 12 . The coracobrachialis muscle is used as a transposition flap in the reconstruction of soft tissue defects of infraclavicular and axillary areas and in post-mastectomy reconstruction 10. It can be used in graft surgeries as an accessory muscle and its removal may not cause any functional problem 13. It is also a guide to the axillary artery during surgery and anesthesia. Anatomic variations of coracobrachialis muscle may easily be confused with other muscle and pathologic conditions at CT and MRI scans 13. So, surgeons and radiologists should be aware of variations of this muscle.
EMBRYOLOGICAL BASIS
The morphologic variation of the coracobrachialis may be explained on the basis of the embryogenesis of the muscles of the arm. The muscles of the upper limb differentiate in situ from the limb bud mesenchyme. The muscle primordia within the different layers of the arm fuse to form a single muscle mass, thereafter, some muscle primordia disappear through apoptosis. Failure of muscle primordia to disappear during development may account for the presence of the accessory insertion of coracobrachialis muscle reported in this case 14.
CONCLUSION
Surgeons and radiologist should keep in mind about such variations of coracobrachialis muscle while doing the surgeries and any radiological procedure. If this variation present it can be used as transpositional flap in postmastectomy reconstruction and also can be used in graft surgeries. If such variation present clinician should keep in mind that embryological basis of such variation.
ACKNOWLEDGEMENT
The authors wish to acknowledge with gratitude the permission given by Dr. Pritha Bhuiyan, Professor and Head of Anatomy, Seth GS Medical College and K.E.M. Hospital, Mumbai for publishing this article.
References:
1. William PL, Warwick R, Dyson M, Bannister LH: Gray’s anatomy 37th edition, Edinburgh, Churchill Livingstone, 1989; 614-615.
2. McMinn RMH. Editor Last’s Anatomy: Regional and Applied. 8th ed. Edinburgh, Churchill Livingstone, 1990 ; 79.
3. Kumar N, Shetty SD, Somayaji SN, Nayak SB: Presence of accessory coracobrachialis and its clinical importance – A case report, Int. J. Anat. Var. (IJAV). 2012 ; 5:27-28.
4. Wood J.: On human muscular variations and their relation to comparative anatomy, J. Anatomy Physiol. 1867; 1:44-59.
5. El-Naggar MM, Zahir FI: Two bellies of coracobrachialis muscle associated with a third head of the biceps brachii muscle, Clin.Anat.2001; 14(5): 379-82.
6. Bergman RA, Thompson SA, Afifi AK, Saadeh FA: Muscles In Compendium of Human Anatomical Variation Text, Atlas and World Literature. Baltimore, Urban and Schwarzenberg, 1988; 10-11.
7. Ray B, Rai A.L, Roy T.S.: Unusual insertion of coracobrachialis muscle to the brachial fascia associated with high division of brachial artery, Clinical Anatomy, 2004; 17:672-676.
8. Doyle J, Bottle M, Krames C, Roselius E.: Editors Muscle Anatomy In: Surgical Anatomy of the hand and upper extremity. Baltimore, Lippincott, Williams and Wilkins, 2003; 97-98.
9. Rodrigues V, Nayak S, Nagabhodshana S, Vollala VR: Median nerve and brachial artery entrapment in the tendinous arch of coracobrachialis muscle, Int. J. Anat. Var. (IJAV). 2008 ; 1:28-29.
10. Kopuz C, Icten N, Yildirim M.: A rare accessory coracobrachialis muscle: A review of literature, Surgical Radio Anat.2003; 24: 406-410.
11. El-Naggar MM, Al-Saggaf S: Variant of coracobrachialis muscle with tunnel for median nerve and brachial artery. Clin.Anat.2004; 17: 139-143.
12. Potu BK, Rao MS, Nayak SR, Vollala VR, Mandava AK, Thomas H: Variant insertion of coracobrachialis muscle in a south Karnataka cadaver, Cases Journal.2008; 1:291.
13. Kumar N, Shetty SD, Somayaji SN, Nayak SB: Presence of accessory coracobrachialis and its clinical importance –a case report, Int. J. Anat. Var. (IJAV),2012; 5:27-28.
14. Guha R, Satyanarayana N, Reddy CK, Jayasri N, Nitin V, Praveen G, Sunitha P, Datta AK: Variant insertion of coracobrachialis musclemorphological significance, embryological basis and clinical importance, JCMSNEPAL.2010; 6(2):42-46.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





