IJCRR - 5(17), September, 2013
Pages: 79-81
Date of Publication: 12-Sep-2013
Print Article
Download XML Download PDF
COMPLETELY OSSIFIED SUPRASCAPULAR LIGAMENT - A CASE REPORT
Author: Pushpa N.B., Roshni Bajpe, Shubha R.
Category: Healthcare
Abstract:The suprascapular notch is bridged by the superior transverse scapular ligament, (suprascapular ligament) which is attached laterally to the root of the coracoid process of the scapula and medially to medial limit of the notch. The ligament is sometimes ossified. The suprascapular nerve passes below the ligament and enters the supraspinous fossa, whereas the suprascapular vessels pass backwards above the ligament. During routine osteological class for I MBBS students we came across a scapula with completely ossified suprascapular ligament. Suprascapular nerve is mostly susceptible for entrapment at the suprascapular notch. A narrow notch or a calcified ligament has been shown to cause increased risk of injury to the suprascapular nerve.
Keywords: Suprascapular notch, Transverse scapular ligament, Entrapment syndrome.
Full Text:
INTRODUCTION
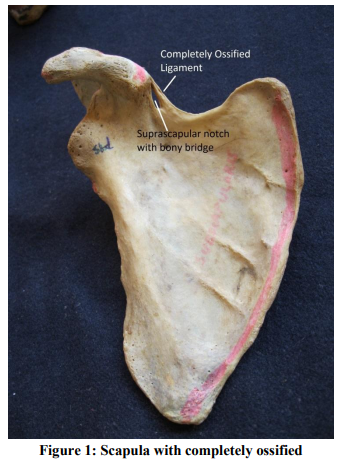
The superior transverse scapular ligament (suprascapular ligament) converts the scapular notch into a foramen or opening. It is sometimes ossified. The ligament is a thin and flat fasciculus, which is narrow at the middle than at the extremities. It is attached by one end to the base of the coracoid process, and by the other end to the medial end of the notch. The suprascapular nerve passes through the foramen and the suprascapular vessels passes above the ligament1 . After passing through the notch, the nerve enters the supraspinous fossa where it supplies supraspinatus and then shoulder capsule, glenohumeral and acromioclavicular joints. The nerve then supplies infraspinatous muscle after crossing the lateral margin of the scapular spine. Most suprascapular nerve entrapments occur at the suprascapular notch as a result of compression by the overlying suprascapular ligament2 . Case report: During routine osteology class for I MBBS students in the department of Anatomy at KIMS Bangalore, we came across a scapula with completely ossified superior transverse scapular ligament with very narrow scapular foramen [Fig1]. The ossified ligament’s dimensions are superior border – 8mm, inferior border – 3.64mm and thickness – 4.40mm. No other deformities were found in the bone.
DISCUSSION
In some animals the suprascapular notch is frequently bridged by bone rather than a ligament, converting the notch into a foramen3 . The incidence of bony foramen in scapulae varied from 0.3% to 13.6%, [where the superior transverse scapular ligament was completely ossified and scapular notch was closed]4 . Kopell and Thompson first described entrapment syndrome of suprascapular nerve at suprascapular notch. According to these authors the movement of abduction or horizontal adduction of the shoulder resulted in compression of the nerve against the ligament as quoted by Antoniadis G et al5 . Gray found foramen in 73 out of 1,151 scapulae (6.34%) but among 87 Indian scapulae none had foramen in them6 . Cohen et al. described a familial case of calcified superior transverse scapular ligament, affecting a 58 years old man and his son too, causing entrapment neuropathy of the suprascapular nerve, clinical symptoms of pain, weakness, atrophy of supraspinatus muscle as quoted by Khan. Khan also reported a case of completely ossified superior transverse scapular ligament in an Indian adult male3 . There are descriptions in the literature of bifid7 and trifid8 superior transverse scapular ligament, with former causing entrapment of suprascapular nerve. Compared to other painful conditions on the shoulder, suprascapular nerve entrapment is an obscure and uncommon syndrome causing severe shoulder pain and disability. It is easily cured if is recognised9 . An arthroscopic approach is a more sophisticated way of addressing the suprascapular nerve entrapment at suprascapular notch but a relative contraindication to arthroscopic release is transverse scapular ligament calcification or ossification10. The identification of the bony bridge is very important, because in these cases apart from dissecting the ligament the bony bridge must also be excised during the procedure, in order to achieve better post-operative results. Radiologists, Neurosurgeons and orthopaedic surgeons should be aware of ossified transverse scapular ligament, as it is necessary to identify and address it during the preoperative radiological examination or intra-operatively, since its existence alters the surgical technique during open or arthroscopic decompression of suprascapular nerve11 .
CONCLUSION
In the present case we are reporting a completely ossified superior transverse scapular ligament, with a very narrow scapular foramen in a south Indian adult which is significant in causing compression of suprascapular nerve.
ACKNOWLEDGEMENT
Authors are grateful to Department of Anatomy, KIMS, Bangalore and also to the authors whose articles are cited and included in the references of the manuscript.
References:
1. Standring S, Borley NR, Collins P, Crossman AR, Gatzoulis MA, Healy JC, et al. Gray’s Anatomy: The Anatomical Basis Of Clinical Practice. 40thedition, London: Elsevier Ltd.,2008: 793, 795
2. Canale ST, Beaty JH, Linda Jones KD, et al. Campbell's Operative Orthopaedics. 11th edition, vol 3, Philadelphia: Elsevier Inc., 2008:2631
3. Khan MA. Complete ossification of the superior transverse scapular ligament in an Indian male adult. Int. J.Morphol., 2006; 24(2):195-6.
4. Polguj M, Jedrzejewski K S, Podgorski M, Topol M. Correlation between Morphometry of the suprascapular notch and anthropometric measurements of the scapula. Folia Morphol. 2011; 70(2):109-15.
5. Das S, Suri R , Kapur V. Ossification of superior transverse scapular ligament and its clinical implications sultan qaboos univ med j.2007;7(2)157-160
6. Gray DJ. Variations in the human scapulae. Am. J. Phys.Anthropol., 1942; 29:57-72.
7. Polguj M, Jedrzejewski K, Majos A and Topol M. Variations in bifid superior transverse scapular ligament as a possible factor of suprascapular entrapment: an anatomical study. International Orthopaedics (SICOT), 2012;36:2095–2100
8. Ticker JB, Djurasovic M, Strauch RJ, April EW, Pollock RG, Flatow EL et al. The incidence of ganglion cysts and variations in anatomy along the course of the suprascapular nerve. J. Shoulder Elbow Surg., 1998 7(5):472-8.
9. Priya R, Manjunath KY, Balasubramanyam V. Morphology of suprascapular notch. Anatomica Karnataka.2004; 1(5):32-35.
10. Millett P, Barton S: Suprascapular nerve entrapment: Technique for arthroscopic release. Techniques in Shoulder and Elbow Surgery. 2006; 7(2):89-94.
11. Natsis K, Totlis T, Gigis I, Vlasis K, Papathanasiou E, Tsikaras P. A bony bridge within the suprascapular notch. Anatomic study and clinical relevance. Aristotle University Medical Journal. February 2008: 35(1), 29-33.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





